

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hypoglycemia is a major obstacle to tight glycemic control and the most unwanted acute complication in the treatment of diabetes. In 2004, the American Diabetes Association defined five categories of hypoglycemia based on glucose levels and the accompanying symptoms. Within this categorization, severe hypoglycemia is defined as an event that requires assistance of another person who actively takes resuscitative actions, and it can result in brain injury, seizures, coma, and even death [1]. Severe hypoglycemia has been confirmed to show an association with an increased risk of cardiovascular events and death [23]. Recurrent hypoglycemic events also increase the risk of dementia and reduce quality of life [4]. Therefore, the balance between ensuring optimal glucose control to prevent chronic diabetic complications and avoiding hypoglycemia is key to the treatment of diabetes.
A gradual decline in plasma glucose concentrations leads to a sequence of neuroendocrine counterregulatory responses, which comprise a physiological defense mechanism that restores balance and prevents hypoglycemia. In healthy individuals, when plasma glucose level falls within the physiological range (>80 mg/dL or 4.4 mmol/L), insulin secretion by pancreatic β-cells decreases. When the plasma glucose level falls just below the physiological range (65 to 70 mg/dL or 3.6 to 3.9 mmol/L), counterregulatory hormones are released. This includes glucagon from pancreatic α-cells, and epinephrine as part of the sympathoadrenal response. These hormones result in various warning symptoms and metabolic alterations to defend against the aggravation of hypoglycemia. In contrast to the rapid effects of glucagon and epinephrine on glucose regulation, the effects of cortisol, growth hormone, and other critical counterregulatory hormones during severe hypoglycemia are delayed. Growth hormone and cortisol start to be released at glucose levels of 66 mg/dL (3.7 mmol/L) and 58 mg/dL (3.2 mmol/L) respectively, stimulating gluconeogenesis, ketogenesis, and lipolysis in liver and adipose tissues [5].
The important role of the sympathoadrenal response in protecting against severe hypoglycemia has been widely studied [6]. Changes in counterregulatory hormone responses to hypoglycemia in healthy subjects have also been studied. Rizza et al. [7] and Feldman et al. [8] found that growth hormone and cortisol may not be essential for the recovery of hypoglycemia. Rather, glucagon and epinephrine can contribute to the recovery of normal glucose levels after insulin-induced hypoglycemia [78]. Interestingly, Boyle and Cryer [9] found that patients with deficient cortisol and growth hormone levels due to hypopituitarism had significantly lower glucose levels than healthy people.
The role of growth hormone and cortisol responses in effective glucose counterregulation during severe hypoglycemia has not been addressed in patients with type 2 diabetes. The characteristics of type 2 diabetes patients with impaired cortisol and/or growth hormone response also have not been described.
In this study, we investigated the prevalence of impaired cortisol and/or growth hormone counterregulatory responses in patients with type 2 diabetes during severe hypoglycemia and evaluated the factors associated with impaired hormonal responses.
Go to : 
METHODS
Study subjects
We reviewed the medical records of patients with type 2 diabetes who visited the emergency department of Konkuk University Medical Center with severe hypoglycemia from August 2006 to December 2015 with available data about cortisol and growth hormone levels. Severe hypoglycemia was defined as a plasma glucose level <40 mg/dL with loss of consciousness. Only hypoglycemic patients with plasma glucose level <40 mg/dL and loss of consciousness at the time of emergency department admission were included in this study. We excluded subjects with (1) type 1 diabetes, (2) any history of glucocorticoid and/or growth hormone administration (including patients with a history of pituitary disease), (3) a serum albumin level <3 g/dL, (4) no growth hormone data, and (5) cardiac arrest with unknown origin. A total of 112 patients were enrolled. We collected data about age, sex, duration of diabetes, number of episodes of severe hypoglycemia, admission rate, anthropometric measurements (including blood pressure, heart rate, and body mass index [BMI]), comorbidities, and medications. Laboratory data were also collected, including growth hormone, cortisol, adrenocorticotropic hormone (ACTH), glucose, hemoglobin A1c (HbA1c), C-peptide, insulin, glucagon, hemoglobin, albumin, blood urea, creatinine, electrolyte, calcium, phosphate, and liver enzyme levels.
This study protocol was approved by the Institutional Review Board of Konkuk University Medical Center (KUH1011002). The informed consent from the participants was waived from the Institutional Review Board as it was a retrospective analysis based on existing data sets for routine patient care.
Measurements of cortisol and growth hormone
Blood samples were obtained at the time of arrival to the emergency unit to check serum cortisol and growth hormone concentrations. Cortisol and growth hormone levels were measured on a Siemens ADVIA Centaur XP analyzer (Siemens Diagnostics, Deerfield, IL, USA) and a Siemens Immulite 2000 analyzer (Siemens Diagnostics, Malvern, PA, USA), respectively, using automated chemiluminescent immunometric assays. Serum cortisol levels above 18 µg/dL and growth hormone levels above 5 ng/mL during severe hypoglycemic episodes were considered to indicate a normal response [1011].
Statistical analysis
Data were analyzed with SPSS version 17.0 (SPSS Inc., Chicago, IL, USA), and P values <0.05 were considered to indicate statistical significance. Data are represented as mean±standard deviation or median (interquartile range [IQR]) for continuous variables and as number and percentage for categorical variables. Statistical significance for comparisons between two groups (normal group vs. other groups) was tested using the independent t test or the Mann-Whitney test for continuous variables. Categorical variables were compared using the Pearson chi-square test or the Fisher exact test. Multiple logistic regression models (adjusted) for an abnormal cortisol response (serum cortisol <18 µg/dL), an abnormal growth hormone response (serum growth hormone <5 ng/mL), and an abnormal cortisol and growth hormone response were constructed using predictors that were entered to estimate the odds ratio (OR) with a 95% CI.
Go to :
RESULTS
Baseline characteristics
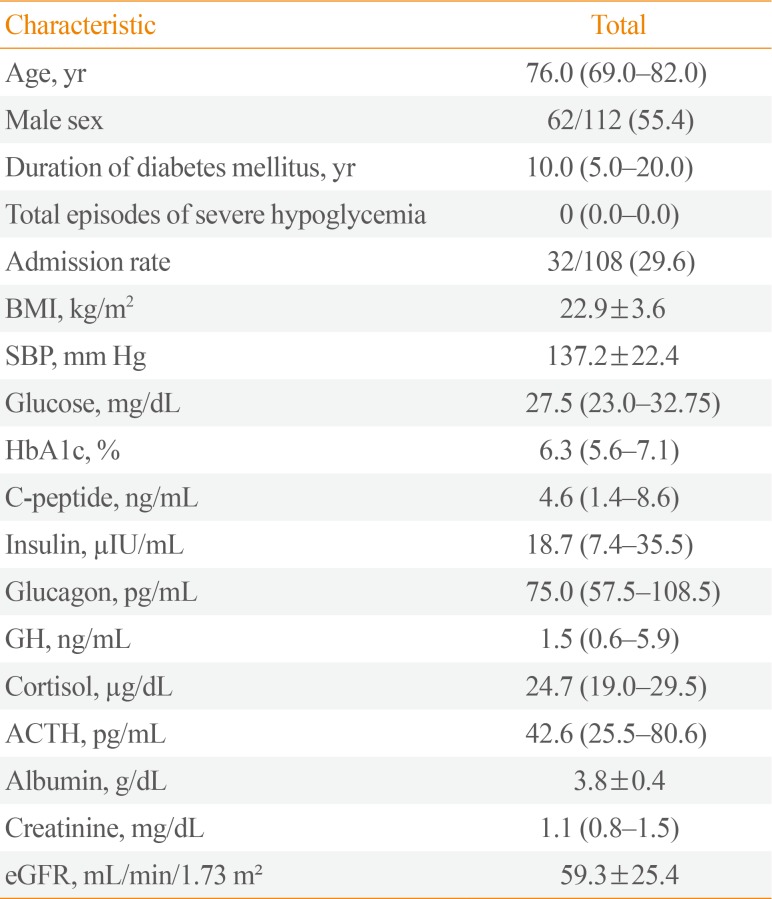
Of the 112 patients with severe hypoglycemia, 62 (55.4%) were male. Their median age was 76.0 years (IQR, 69.0 to 82.0) and the median duration of diabetes was 10.0 years (IQR, 5.0 to 20.0). The median blood glucose level at the time of severe hypoglycemia was 27.5 mg/dL (IQR, 23.0 to 32.75) and the median HbA1c was 6.3% (IQR, 5.6% to 7.1%). The median C-peptide and insulin levels were 4.6 ng/mL (IQR, 1.4 to 8.6) and 18.7 µIU/mL (IQR, 7.4 to 35.5), respectively. The median cortisol, growth hormone, and ACTH levels were 24.7 µg/dL (IQR, 19.0 to 29.5), 1.5 ng/mL (IQR, 0.6 to 5.9), and 42.6 pg/mL (IQR, 25.5 to 80.6), respectively (Table 1).
Prevalence of patients with impaired cortisol and/or growth hormone response during severe hypoglycemia
Of the 112 hypoglycemic patients, 23 (20.5%) showed an impaired cortisol response (<18 µg/dL), 82 (73.2%) showed an impaired growth hormone response (<5 ng/mL), and 19 patients (17.0%) impaired responses of both cortisol and growth hormone (Fig. 1).
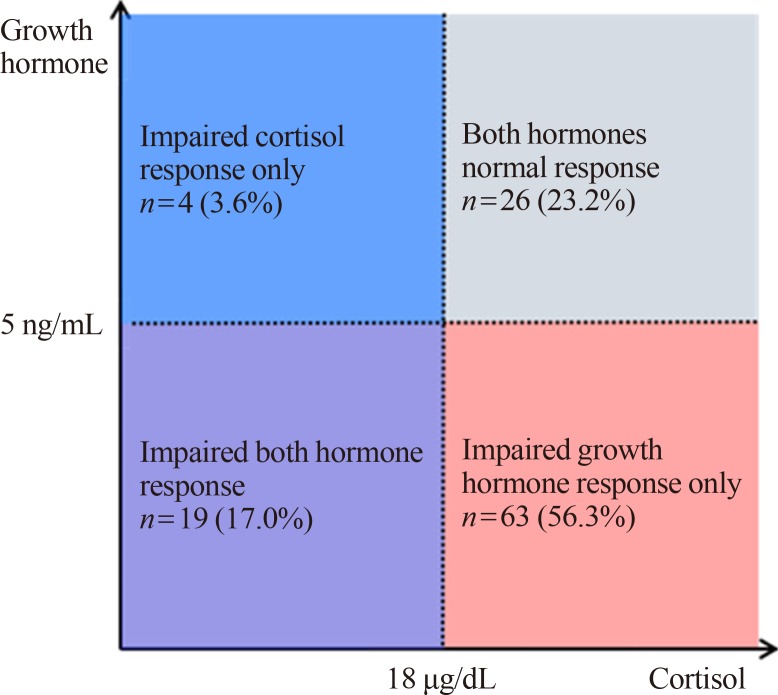 | Fig. 1Number of patients with impaired cortisol and/or growth hormone response during severe hypoglycemia. The impaired cortisol response group includes patients with an impaired cortisol response only (blue box) and those with impaired responses of both hormones (purple box). The impaired growth hormone response group includes patients with an impaired growth hormone response only (red box) and an impaired response of both hormones (purple box).
|
Comparison of clinical characteristics between patients with an impaired cortisol and/or growth hormone response and those with a normal response
To investigate the characteristics of patients with an impaired cortisol and/or growth hormone counterregulatory response, we compared them with patients who had normal hormonal responses (Table 2).
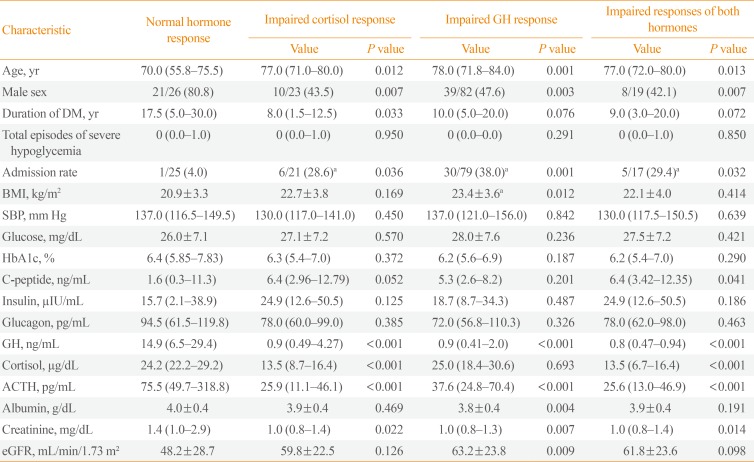
The patients with an impaired cortisol response were older (77.0 years [IQR, 71.0 to 80.0] vs. 70.0 years [IQR, 55.8 to 75.5], P=0.012) and more likely to be female (43.5% vs. 80.8%, P=0.007), and had a shorter duration of type 2 diabetes (8.0 years [IQR, 1.5 to 12.5] vs. 17.5 years [IQR, 5.0 to 30.0], P=0.033), a higher admission rate (28.6% vs. 4.0%, P=0.036), a lower growth hormone response (0.9 ng/mL [IQR, 0.49 to 4.27] vs. 14.9 ng/mL [IQR, 6.5 to 29.4], P<0.001), a lower ACTH response (25.9 pg/mL [IQR, 11.1 to 46.1] vs. 75.5 pg/mL [IQR, 49.7 to 31.8.8], P<0.001), and lower creatinine levels (1.0 mg/dL [IQR, 0.8 to 1.4] vs. 1.4 mg/dL [IQR, 1.0 to 2.9], P=0.022) than patients with a normal hormonal response. Higher admission rate means the percentage of patients who are admitted to the hospital from the emergency department due to hypoglycemia.
The patients with an impaired growth hormone response were older (78.0 years [IQR, 71.8 to 84.0] vs. 70.0 years [IQR, 55.8 to 75.5], P=0.001) and more likely to be female (47.6% vs. 80.8%, P=0.003), and had a higher admission rate (38.0% vs. 4.0%, P=0.001), a lower ACTH response (37.6 pg/mL [IQR, 24.8 to 70.4] vs. 75.5 pg/mL [IQR, 49.7 to 318.8], P<0.001), lower albumin levels (3.8±0.4 g/dL vs. 4.0±0.4 g/dL, P=0.004), lower creatinine levels (1.0 mg/dL [IQR, 0.8 to 1.3] vs. 1.4 mg/dL [IQR, 1.0 to 2.9], P=0.007), and a higher estimated glomerular filtration rate (63.2±23.8 mL/min/1.73 m2 vs. 48.2±28.7 mL/min/1.73 m2, P=0.009) than patients with a normal hormonal response.
The patients with impaired responses to both cortisol and growth hormone were older (77.0 years [IQR, 72.0 to 80.0] vs. 70.0 years [IQR, 55.8 to 75.5], P=0.013) and more likely to be female (42.1% vs. 80.8%, P=0.007), and had a higher admission rate (29.4% vs. 4.0%, P=0.032), higher C-peptide levels (6.4 ng/mL [IQR, 3.42 to 12.35] vs. 1.6 ng/mL [IQR, 0.3 to 11.3], P=0.041), a lower ACTH response (25.6 pg/mL [IQR, 13.0 to 46.9] vs. 75.5 pg/mL [IQR, 49.7 to 318.8], P<0.001), and lower creatinine levels (1.0 mg/dL [IQR, 0.8 to 1.4] vs. 1.4 mg/dL [IQR, 1.0 to 2.9], P=0.014) than patients with a normal hormonal response.
Predictive factors of impaired cortisol and/or growth hormone responses
Logistic regression analysis was performed to evaluate the predictive factors of impaired cortisol and/or growth hormone counterregulatory responses during severe hypoglycemia (Table 3). An impaired cortisol response was positively associated with advanced age (OR, 1.070; P=0.044) and a higher admission rate (OR, 21.265; P=0.015), and negatively associated with male sex (OR, 0.208; P=0.021), duration of type 2 diabetes (OR, 0.942; P=0.042), growth hormone levels (OR, 0.669; P=0.004), and ACTH levels (OR, 0.962; P=0.007). The multivariate analysis confirmed that a higher risk of an impaired cortisol response was associated with age (OR, 1.131; P=0.030), whereas a lower risk was associated with male sex (OR, 0.104; P=0.035). Furthermore, an impaired cortisol response was associated with a higher admission rate (OR, 40.406; P=0.010).
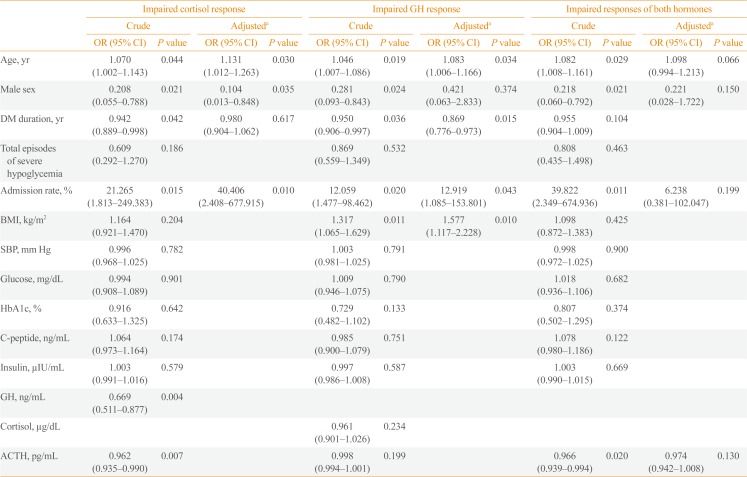
In comparison to patients with a normal hormonal response, an impaired growth hormone response was positively associated with age (OR, 1.046; P=0.019), a higher admission rate (OR, 12.059; P=0.020), and BMI (OR, 1.317; P=0.011), and negatively associated with male sex (OR, 0.281; P=0.024) and duration of type 2 diabetes (OR, 0.950; P=0.036). Multiple logistic regression analysis showed that an impaired growth hormone response was associated with age (OR, 1.083; P=0.034), duration of type 2 diabetes (OR, 0.869; P=0.015), a higher admission rate (OR, 12.919; P=0.043), and BMI (OR, 1.577; P=0.010).
We also analyzed impaired responses of both cortisol and growth hormone as a dependent variable. Logistic regression analysis showed that an impaired response of both hormones was positively associated with age (OR, 1.082; P=0.029) and a higher admission rate (OR, 39.822; P=0.011), whereas a negative association was shown with male sex (OR, 0.218; P=0.021) and ACTH levels (OR, 0.966; P=0.019). However, multiple logistic regression analysis found that no risk factors were significantly associated with impaired responses of both hormones.
Go to :
DISCUSSION
In this study, we showed that considerable numbers of patients with type 2 diabetes had blunted counterregulatory responses of cortisol and/or growth hormone to severe hypoglycemia; 20.5% and 73.2% of type 2 diabetes patients showed an impaired cortisol or growth hormone response, respectively, which is a much higher prevalence than has been observed in the general population [1112]. The prevalence of hormone deficiencies in the general population is as follows: 0.015% to 0.028% for primary adrenal insufficiency, 0.0093% to 0.0144% for secondary adrenal insufficiency, and 0.001% for growth hormone deficiency. Therefore, the high prevalence of impaired cortisol levels and growth hormone deficiency in patients with type 2 diabetes is very unusual.
The exact causes of the impaired cortisol or growth hormone response in each subject is unclear. The counterregulatory cortisol or growth hormone response is mainly regulated through the central nervous system (CNS) [13]. Whether an impaired cortisol or growth hormone response to hypoglycemia is causally related to severe hypoglycemia or reflects disrupted integrity of CNS function, leading to susceptibility to hypoglycemia, should be investigated in further studies. Furthermore, we need to consider the possibility that some of these patients may have had adrenal insufficiency or growth hormone deficiency, and further investigations should assess whether patients with an impaired hormonal response need hormone replacement therapy.
Many studies have investigated the various factors that affect the strength of the counterregulatory response in healthy persons. The recurrence of hypoglycemia blunted the acute counterregulatory response to subsequent hypoglycemia [141516]. Other studies have shown that antecedent exercise, stimulation of the hypothalamic-pituitary-adrenal axis, age, and female sex blunted the counterregulatory response in healthy persons [171819202122]. Hyperinsulinemia can also weaken the counterregulatory response to hypoglycemia [23]. However, few studies have investigated factors affecting the counterregulatory response to hypoglycemia in patients with type 2 diabetes. We analyzed the characteristics and risk factors of type 2 diabetes patients with a normal hormonal response, an impaired cortisol response, an impaired growth hormone response, and impaired responses of both cortisol and growth hormone.
When we compared the characteristics of patients who had an impaired cortisol and/or growth hormone response to those of patients with a normal hormonal response during severe hypoglycemia, those with an impaired cortisol and/or growth hormone response were significantly older, showed a female predominance, had a higher admission rate, and had lower ACTH levels. The patients with impaired responses of both cortisol and growth hormone showed higher C-peptide levels, whereas C-peptide levels were not significantly elevated in those with only an impaired cortisol response or an impaired growth hormone response. Since C-peptide levels reflect blood insulin levels, high levels of C-peptide in the impaired hormone response group is consistent with the previous result that hyperinsulinemia suppresses the counterregulatory hormone response to hypoglycemia in normal individuals [23]. The admission rates were significantly higher in patients with impaired cortisol and/or growth hormone responses than in those with a normal hormonal response. It is noteworthy that patients with abnormal hormonal responses were more likely to be hospitalized and may have had more severe conditions than those with a normal hormonal response.
Multiple logistic regression analysis demonstrated that an impaired response of growth hormone was associated with age, female sex, duration of type 2 diabetes, the admission rate, and BMI. Age, duration of type 2 diabetes, and BMI were confirmed to be significant risk factors for an impaired growth hormone response in the multivariate analysis. A study about inducing hypoglycemia in normal people showed that growth responses were significantly lower in female than in male during hypoglycemia, and there was no difference in cortisol response between male and female [22]. The results of this study suggest that there may be a difference between male and female in the growth hormone response. Johannsson et al. [24] reported that body fat and lean body mass were inversely correlated with growth hormone during growth hormone treatment in growth-hormone–deficient adults. We found that overweight type 2 diabetes patients might have a higher risk of an impaired growth hormone response during severe hypoglycemia. A shorter duration of diabetes diagnosis tends to lower blood glucose targets, and low glycemic target may increase the frequency of recurrent hypoglycemia. We carefully think that the increased frequency of recurrent hypoglycemia might lead to more abnormal counterregulatory responses.
The current study had several limitations, including a small number of patients, a retrospective design, and the fact that it only presented experiences from one tertiary center. However, to our knowledge, this is the first report to explore impaired counterregulatory cortisol and/or growth hormone responses to severe hypoglycemia in patients with type 2 diabetes. We explored the characteristics of type 2 diabetes patients who showed inappropriate cortisol and growth hormone responses to severe hypoglycemia and attempted to identify the corresponding risk factors. Our findings underscore the importance of maintaining a higher HbA1c target in older patients, and especially women, to avoid hypoglycemia and the fact that patients with recurrent hypoglycemia and frequent admissions due to hypoglycemia require a further diagnostic evaluation of cortisol and/or growth hormone deficiencies.
Go to :
 XML Download
XML Download