

 PDF
PDF ePub
ePub Citation
Citation Print
Print



CASE REPORT
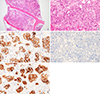
Bone marrow metastasis of colon cancer is an uncommon finding. Here, we report a rare case of a patient who presented with bone marrow metastasis of colon cancer as primary diagnosis, along with pancytopenia. A 56-year-old woman visited the hematology-oncology outpatient department due to pancytopenia (white blood cells 2.95×106/L, reference range 4.0–10.0×106/L; hemoglobin 90 g/L, reference range 120–160 g/L; platelets 97×106/L, reference range 150–400×106/L). She also complained of back pain and weight loss (5 kg per month). Magnetic resonance imaging of the spine showed diffuse signal changes in the first and second thoracic vertebrae, with heterogeneous enhancement of the whole spine, which was suggestive of malignant bony metastasis. Abdominal and pelvic computed tomography (CT) and colonoscopy revealed a large mass that completely obstructed the ascending colon. A biopsy identified moderately differentiated adenocarcinoma, and molecular analysis of the biopsy specimen detected a missense mutation in the 12th codon of the KRAS gene. Subsequent chest CT and positron emission tomography-CT showed metastasis of colon cancer to the lymph nodes, lungs, and the axial skeleton. Peripheral blood morphology showed pancytopenia with leukoerythroblastosis. Bone marrow aspiration and biopsy were performed. The aspirate was markedly diluted, and the biopsy revealed hypercellular marrow with patchy infiltration of malignant cells and glandular formation. The presence of metastatic carcinoma was subsequently confirmed by positive immunohistochemical (IHC) staining with an anti-pan-cytokeratin (pan-CK) antibody. Then, we performed additional IHC staining with anti-cytokeratin 7 (CK7) and anti-cytokeratin 20 (CK20) antibodies. The sample was positive for anti-CK20 IHC staining, but negative for anti-CK7 IHC staining, strongly suggesting that it originated from colon cancer (Fig. 1). She is undergoing chemotherapy using bevacizumab, 5-fluorouracil, leucovorin, and irinotecan, and is in the fourth cycle without significant adverse events.
DISCUSSION
Colon cancer is the third most common cancer in Korea [1]. The most common metastatic sites are the liver and lungs, and the incidence of bone and bone marrow metastases from colon cancer is quite low [23]. In a study of 252 patients with colorectal cancer, only 5.5% were diagnosed with bony metastases [4]. The most frequent histological types are poorly differentiated adenocarcinoma and signet-ring cell carcinoma [5]. To the best of our knowledge, only two cases of bone marrow metastasis of colon cancer have been reported in Korean adults. In the first case, bone marrow metastasis was the primary diagnosis [6], and in the other case, the bone marrow was the first site of recurrence [3]. In our patient, the bone marrow metastasis was not highly suspicious because the histological type was moderately differentiated adenocarcinoma, and the sites of metastases were limited to the lungs and axial bones. Bone and bone marrow metastases of colon cancer are regarded as clinically uncommon.
Cytokeratins are filamentous proteins found in epithelial cells that are expressed in a tissue-specific manner [7]. The expression patterns of CK7 and CK20 have been found to be useful for the differential diagnosis of carcinomas of epithelial origin [8]. CK7 is expressed in carcinomas originating from tumors in the lung, breast, ovary, and bile ducts. CK20 is expressed in all colorectal carcinomas, and in a majority of gastric and pancreatic carcinomas. Carcinomas originating from the prostate and kidney, sarcomas, and hepatocellular carcinomas have been found to be negative for both CK7 and CK20 staining [78]. In our patient, the IHC staining was positive for pan-CK and CK20 and negative for CK7, which is consistent with carcinoma originating from the colon.
The prognostic significance of bone marrow metastasis of colon cancer is still controversial, because of the limited number of cases that have been reported, and comparison of the data is difficult due to somewhat different disease definitions and evaluation methods [91011]. There is emerging evidence that bone marrow micrometastasis of stage I–III colon cancer is related to poor prognosis for disease-free and overall survival [1213]. Our patient has been treated with the standard chemotherapy regimen for stage IV colon cancer. Frequent follow-ups regarding the response status of the disease are necessary because the clinical presentation of the metastatic pattern is unusual.
In conclusion, a bone marrow study should be promptly performed when unexplained cytopenia is detected in patients with solid tumors, even if the origin of the carcinoma is known to rarely metastasize to bone marrow. In the case of metastatic carcinoma, IHC staining with anti-CK7 and anti-CK20 antibodies is useful for determining the origin of carcinoma, especially in the case of metastatic carcinoma of unknown origin.
 XML Download
XML Download