

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cancer is a serious disease not only physically but also socially; morbidity and mortality reduce community productivity.1 Although the cancer survival rate is gradually increasing in Korea, cancer treatment costs are also rising, heavily burdening patients of low socioeconomic status.2 Thus, early detection of resectable cancer is essential to improve survival and reduce costs.1
As life expectancy has increased over the past few decades, the numbers of patients with diabetes and hypertension have also increased, along with the prevalence of end-stage renal disease (ESRD).3 Furthermore, cardiovascular survival and the quality of dialysis have improved, and thus the life expectancies of dialysis patients have increased.4 Reduced renal function is associated with an increased risk of malignancy5; thus, as ESRD populations increase in size, cancer detection and management are essential. However, the incidence of cancer in ESRD patients remains unclear, and the primary cancer sites may differ from those of the general population.
Although some population-based studies explored cancer incidences in dialysis patients,678910 the differences in cancer incidences and affected sites between such patients and the general population remain unclear. Also, there is still lack of research dealing with the whole dialysis population of the country. We explored cancer incidences in Korean dialysis patients and used national health insurance data to guide cancer screening in dialysis clinics. We compared the cancer characteristics of dialysis patients with those of age-matched controls in terms of age, economic status, and dialysis modality.
METHODS
Study design and data
Data on dialysis patients were obtained from the National Health Information database. The Korean National Health Insurance Service (KNHIS), the only national insurance provider in Korea, has operated since July 1989 and covers over 97% of the Korean population. The database contains records of reimbursements to all Korean medical facilities, and we used this information to create our cohorts. We compiled our control group from the general population of the KNHIS National Sample Cohort of the National Health Information database established by the KNHIS in 2011. These cohort data were collected from approximately 1,000,000 subjects (2.2% of the Korean population), extracted via sampling of the 2002 records of the National Health Information database.11 The data include insurance and socioeconomic statuses, details on utilization of healthcare services, and the KNHIS biannual health examination results of eligible participants enrolled from January 2002 to December 2013.
Definition and selection of the ESRD patients
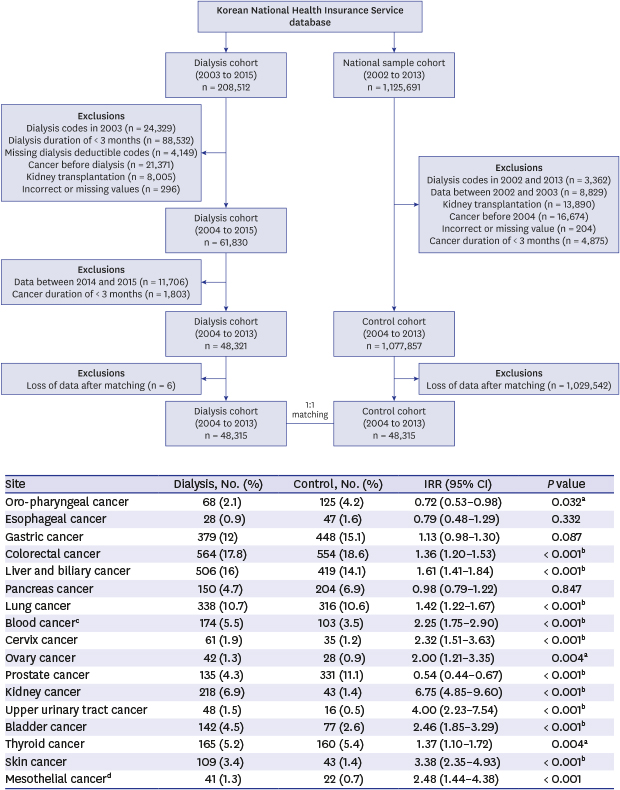
All ESRD patients who underwent dialysis for more than 3 months and were diagnosed with ESRD from 2004 to 2013 in Korea served as the exposure cohort. The dialysis cohort included patients who submitted claims for any procedure or material associated with either hemodialysis or peritoneal dialysis, as revealed by the Korean electronic interchange codes (special dialysis claim codes of V001 and V003, treatment codes of O7020 for hemodialysis and O7061 for peritoneal dialysis) combined with the International Classification of Diseases (ICD) code for chronic kidney disease and end state kidney disease (N18.**). We also reviewed dialysis specific deductible claims of the data. Patients with ESRD who used medical services in 2003 were excluded to rule out those who had chronic ESRD before the investigation commenced. Patients on transplantation were also excluded by renal transplantation operation code claim of insurance data (Fig. 1).

Definition and selection of control cohort
The control cohort was selected from the KNHIS National Sample Cohort which covered 1,125,691 Korean subjects and contained both healthy individuals and patients; including those with chronic kidney disease, ESRD, and transplantation. These conditions represent 2.2% of the whole Korean population disease entities. We excluded all dialysis patients, renal transplantation patients, patients who had cancer before 2004 and patients with a cancer duration of < 3 months (Fig. 1).
Definition of cancers
Cancers were defined using the ICD-10 codes C00.0–99.9. We also regarded diseases coded D00–D09, D37–D48, D61 as cancers. Any secondary malignancies were excluded and chemotherapy, radiotherapy claim codes were also deleted. V193, a cancer specific deductible insurance code in Korea could not be used in this study because the control group was from National Sample Cohort which contained no deductible codes (only ESRD group had V193 code). So we defined cancers as follows to compare with the control group without V193. If a patient's cancer code above was claimed as a major insurance code at least one time from an inpatient claim or 3 times or more from the outpatient system, we regarded that as a diagnosis of cancer. ICD codes for cancers require special co-payments (5% deductible) in Korea; all cancer codes are listed in the KNHIS. Then we proved patient numbers were similar which of V193 codes and our method (Supplementary Tables 1 and 2). Although the patient number was smaller, our method was more specific. We excluded patients diagnosed with cancer before initiation of dialysis and also excluded cancer within 3 months after the initiation of dialysis.
Propensity score matching
We included patients who commenced dialysis prior to a diagnosis of cancer (based on their visit dates). Eligible patients who commenced dialysis from 2004–2013 (the dialysis cohort) were identified after excluding potentially those who previously underwent dialysis or had pre-existing cancer. We identified individuals without ESRD in the KNHIS National Sample Cohort database (the control cohort) and used propensity score matching to assign them to an equal number of ESRD cases. Propensity score matching featured the nearest-neighbor method to identify similar individuals in the dialysis and control cohorts.12 Logistic regression was used to create a propensity score for each patient based on age, gender, and income level. Individuals in each cohort were randomly ordered and matched in a 1:1 ratio using the nearest-neighbor method (Fig. 1).
Statistical analysis
Proportional differences in independent variables between the ESRD and control cohorts were analyzed using the Wald χ2 test. The cancer incidence was defined as the number of newly diagnosed cancers per 100,000 person-years, as revealed by the database. We calculated the incidence rate ratio (IRR) of ESRD relative to that of controls and the 95% confidence interval (CI), using free OpenEpi software (version 3.01; OpenEpi, Atlanta, GA, USA). We entered all independent variables into multivariate Cox's proportional hazards models (after combining the two cohorts) to determine the hazard ratio (HR) of ESRD in terms of cancer development. The follow-up period commenced on the first day of dialysis for cases and on random visit dates (yet during the years of dialysis initiation in the cases) for controls. The follow-up period ended on the date of cancer diagnosis or the date of last follow-up. Cumulative cancer incidence curves were generated using the Kaplan-Meier method and compared between the two cohorts using the log-rank test. All analyses were performed using the SAS statistical package ver. 9.4 (SAS Institute Inc., Cary, NC, USA) and R ver. 3.4.3 (R Foundation for Statistical Computing, Vienna, Austria). A P value less than 0.05 was taken to indicate statistical significance.
RESULTS
Characteristics of the dialysis patients and controls
We selected 208,512 dialysis patients with newly diagnosed ESRD from the KNHIS database. Patients on dialysis prior to 2003 (24,329), with dialysis durations less than 3 months (88,532), without dialysis deductible code (4,149), who had cancer prior to dialysis (21,371), or who had kidney transplantation (8,005) were excluded. Those who developed cancer less than 3 months after the initiation of dialysis (1,803) were also excluded. We finally evaluated 48,315 patients and compared them with 48,315 non-dialysis subjects selected from the national sample cohort of 1,125,691 Koreans via propensity score matching (Fig. 1).
Of the 48,315 dialysis patients, 27,182 were male and 21,133 were female; the mean observation period of dialysis duration was 3.8 ± 2.6 years and control was 5.0 ± 2.7 years; 41,396 were on hemodialysis (85.7%) and 4,415 on peritoneal dialysis (14.3%). ESRD patients were compared with the same numbers of age-matched controls (Table 1), in whom dialysis commonly commenced at 50–69 years of age (24,616, 50.9%). The economic statuses of the patients and controls were similar (Table 1).
Table 1
Baseline characteristics of the dialysis patients and controls
Overall cancer incidence and risks in dialysis patients
A total of 2,504 of the 48,315 dialysis patients developed cancer (5.2%), as did 2,201 (4.6%) of the 48,315 controls. The overall cancer incidence was significantly higher in dialysis patients (IRR, 1.52; 95% CI, 1.43–1.61) and in females compared with males (IRR, 1.63 vs. 1.46). Peak cancer incidence age was 60–69 years in both groups. However, younger dialysis patients exhibited a much higher cancer incidence (IRR, 3.27; 95% CI, 1.39–8.52) than that of the general younger population (Table 2).
Table 2
Characteristics of the cancer cases among the dialysis patients and controls
The cumulative cancer incidence was also significantly higher in dialysis patients (P < 0.001) (Fig. 2). The overall cancer risk was 1.54-fold higher than that of the general population (adjusted HR, 1.71; 95% CI, 1.61–1.81). Although the cancer incidence of younger dialysis patients was high (Table 2), and the risk of cancer increased significantly with age (Table 3), and the risk of cancer was highest at > 80 age compared with younger ages in dialysis patients (adjusted HR, 6.77; 95% CI, 4.59–10.01; P < 0.001). Those of mid-economic status were at a significantly lower risk of cancer, but we found no overall correlation between economic status and cancer (Table 3).
Fig. 2
Cumulative cancer incidence of ESRD patients and controls. The cumulative cancer incidence was also significantly higher in dialysis patients (P < 0.001).
ESRD = end-stage renal disease.
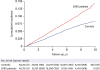
Table 3
Univariate and multivariate analysis of cancer risk factors in the dialysis patient

Primary sites of cancer in the dialysis patients and control
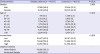
The most common site of malignancy in both the ESRD patients and controls was the colon; the major primary cancers by organ are shown in the order of risk in Table 4. Liver and biliary, lung, and gastric cancers were prominent in both groups. Although stomach cancer showed higher prevalence in the dialysis patients, the incidence rate was not different than the general population, as was the incidence of pancreatic cancer than in the controls (IRRs, 1.13 and 0.98; P = 0.087 and P = 0.847, respectively).
Table 4
Site-specific cancer risk of dialysis patients
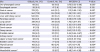
Compared with the general population, kidney cancer (IRR, 6.75; P < 0.001), followed by upper urinary tract cancer (IRR, 4.00; P < 0.001), and skin cancer (IRR, 3.38; P < 0.001) posed the highest malignancy prevalence for the ESRD patients. Different from urinary tract malignancies, prostatic cancer and pro-pharyngeal cancer showed significantly lower prevalence than control group (IRR, 0.54 and 0.72; P < 0.001 and P = 0.032, respectively) (Table 4).
Cancer risk by dialysis modality
Cancers developed in 2,289 (4.6%) of 41,396 hemodialysis patients and in 215 (5.2%) of 4,415 peritoneal dialysis patients. Peritoneal dialysis patients were at a higher risk of malignancy than that of hemodialysis patients (adjusted HRs, 1.91; 95% CI, 1.59–1.79 vs. adjusted HRs, 1.69; 95% CI,1.66–2.2, respectively) (Table 5).
Table 5
HRs and 95% CIs according to type of dialysis

D code malignancies of dialysis and control
D code malignancies were 11.6% vs. 10.4% in the dialysis and control. The numbers of D code malignancies showed no statistical difference between groups (Table 6). All C and D ICD codes of cancer incidence in the dialysis and control were described on Supplementary Table 3.

DISCUSSION
Patients with ESRD are at higher risk of malignancy,1314 and the cancer risk increases by 29% for every decrease in the glomerular filtration rate (GFR) of 10 mL/min, with the greatest risk at a GFR < 40 mL/min.15 Although the causes of malignancy in dialysis patients are poorly known, chronic inflammation may be an important precancerous condition,16 and recurrent urinary tract infections and cystic changes in sclerotic kidneys may predispose to cancer.17 We found that the cancer risk of dialysis patients was 1.54-fold that of the general population. Patients with CKD are at a higher risk of mortality than the general population,18 and this is particularly true of patients with a GFR < 45 mL/min.19 The cumulative cancer mortality in dialysis patients is remarkably higher than that of the general population.8 Although we did not compare the cancer-related mortality rate between the dialysis and control groups, this is needed in the future to better understand the cancer risks and affected sites in Korean dialysis patients.
The cancers that are most prevalent in dialysis patients remain controversial. Yoo et al.10 reported that colorectal, stomach, and kidney cancers were most common. Cheung et al.20 found that although colorectal, kidney, and lung cancers were most prevalent, and the incidence ratios of kidney, tongue, and cervical cancer were higher than those of general population. Lin et al.8 reported that although bladder, liver, and colorectal cancers were most common, the incidence ratios of upper urinary tract, bladder, and kidney cancer were higher than general population. The malignancy sites in the dialysis patients that we identified were similar to those reported in previous studies. Colorectal, liver, and stomach cancers were as common in dialysis patients as in the general population. Kidney and upper urinary tract cancers were significantly more common in dialysis patients than controls, as also found in other studies.
We present a few interesting findings. First, the highest cancer incidence rate ratio by age was < 30 years (IRR, 3.27; P < 0.05) comparing control without dialysis, which showed similar result of Lin et al,7 that implicate younger dialysis patients need to do intensive cancer screening. Second, similar with other studies, we found kidney and urinary tract cancers were the highest incidences in the dialysis patients and most malignancies were developed frequently in the dialysis patients. However, prostatic cancer and oropharyngeal cancer showed lower incidence in the dialysis patients comparing with control (145 [4.3%] vs. 331 [11.1%]; IRR, 0.54; P < 0.001 and 68 [2.1%] vs. 125 [4.2%]; IRR, 0.72, P = 0.032, respectively). Decreased incidence ratio of prostatic cancer is consistent with other studies.71520 However, a few earlier studies found that oral cavity cancer was relatively more common in dialysis patients than in controls,820 our data showed adversary result which needs further investigations to reveal difference. Third, unlike other studies,581014 we added D codes as a malignancy which were usually treated as a pre-cancerous condition, such as carcinoma in situ. As there was no statistical difference of D code-malignancies between dialysis and controls (11.6% vs. 10.4% of total malignancies), our study implicates the importance of considering early stage of malignancies.
Clinico-epidemiological studies based on big data, which aid our understanding of cancer incidence and outcomes, are increasing in Korea.212223 Although large numbers of patients are evaluated,9 comparisons with the general population remain difficult. Lin et al.8 compared national cancer data between dialysis patients and matched controls, but the data were old and the age distribution limited. Here, we used propensity score matching to compare cancer incidences between patients and controls of the same age and social status,12 which assists in the analysis of specific diseases. Our study is important in terms of understanding cancer in dialysis patients.
Our study had certain limitations. First, we have some missing data of malignancies of the whole dialysis population in Korea. A cancer specific insurance claim code, V193 might be used for detecting cancer from the full Korean population with ESRD. However, the control group which was extracted from a national sample cohort study of 1,125,691 (from the whole Korean population) was not based from the insurance payment system, that contains no V193 codes. We compared the number of cancer patients between our cancer definition methods with V193 codes in the control and ESRD groups, and the patient number was similar (Supplementary Tables 1 and 2). Second, we did not include the comorbidity of dialysis and control patients in our analysis, and thus our data were somewhat restricted because national insurance claim data could detect only ICD codes, medications, and procedures. However, we calculated the real-world incidences of malignancies in a Korean dialysis population. Third, we did not evaluate cancer-related death/survival of the patients or controls; this is a limitation of big data analysis. Further, large randomized case-control studies considering co-morbidities and cancer survival would be useful. Fourth, we did not include patients on kidney transplantation for the cancer risk and incidence in this study. Patients on transplantation show higher risk of malignancies and show higher mortality.24 However, as we roughly analyzed the incidence of cancer codes in the transplantation patients, there was no significant difference comparing with dialysis patients (Supplementary Table 2). It might be related with the relatively short observation period. Further investigation would be necessary to reveal these associations.
In conclusion, patients on dialysis are at higher risk of malignancy and should be screened in terms of colorectal, liver, lung, kidney and urinary tract malignancies in the dialysis clinic. Further investigations are required to explore the development and prognosis of malignancies in ESRD patients.
 XML Download
XML Download