

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In 1959, after Avery and Mead1 discovered that the pathophysiology of neonatal respiratory distress syndrome (RDS) involved the insufficient production of pulmonary surfactant (PS) in premature infants, “hyaline membrane disease”—the former name of the disease—was replaced by RDS.
Since the description of the pathophysiology of RDS, studies investigating remedies that supplement PS deficiencies in animal models of RDS have been conducted. In 1980, Fujiwara et al.2 performed treatment via the respiratory tract in 10 pediatric patients with RDS, using Surfactant-TA (Surfacten®; Mitsubishi Tanabe Pharma Corporation, Tokyo, Japan), an artificial PS preparation that was reconstituted by adding phospholipids (PLs) to PS extracted from bovine lung. This was the first successful treatment using artificial PS supplementation in humans, and has since resulted in improvement in oxygenation, treatment progress, and prognosis. This therapy has been further developed in the treatment of RDS, which was previously limited to conventional oxygen therapy, artificial ventilation therapy, and other symptomatic therapies. It was the first time that a treatment method of complementing PS with artificial preparations was used, which was a milestone in this field. Since then, this therapy has become the most important and definitive method of neonatal RDS therapy. In fact, it has contributed significantly to the reduction in RDS mortality in the past 30 years, and to the improvement of neonatal, perinatal, and infant mortality rates.34
Surfacten® was first marketed in Japan in 1986 as the world's first artificial PS replacement therapy for neonatal RDS and, since then, many other similar products have been developed, sold, imported and/or used in Korea. These include Surfacten® since 1991, Exosurf® (generic names as colfosceril palmitate, hexadecanol, and tyloxapol, Wellcome Foundation Ltd., London, UK) since 1991, Curosurf® (generic name as poractant alfa, Chiesi Farmaceutici, Parma, Italy) since 2003, and Infasurf® (generic name as calfactant, Onybiotech, New York, NY, USA) since 2007. The domestic product Newfactan® (Yuhan Corporation, Seoul, Korea) was developed in Korea and has been used since 1996.5
In Korea, PS replacement therapy for neonatal RDS has been available for 30 years. During this time, the survival rates of very low birth weight infants (VLBWI) and extremely low birth weight infants (ELBWI) have been significantly improved and described in various publications.56789 Moreover, the contemporary survival rate is very encouraging, and has reached a level similar to that of advanced countries in Europe and North America.9
The history of PS research and replacement therapy in foreign countries (as a basic background) and the history of PS replacement therapy in Korea are reviewed from the perspective of the history of its use in Korea, results of treatment, and improvements in prognosis. These narratives are summarized to illustrate the history of RDS, inarguably the most important disease in neonatal care.
HISTORY OF PS AROUND THE WORLD
The history of PS research in the age of pre-clinical trials
Laplace was the first to formulate that the external and internal pressures applied to an air bag are inversely proportional to the radius of the air bag and proportional to twice the surface tension (ST). The excess pressure inside a liquid surface is determined by its curvature and tension according to Laplace's equation. A major function of PS is to reduce ST at the air-water interface of the terminal airways, thereby decreasing the tendency for alveolar collapse by Laplace's law.10 In 1929, Von Neergaard11 studied PS function in the porcine lung and demonstrated that a lower ST would be useful for the respiratory mechanism. In 1946, Thannhauser et al.12 showed that the lung contains unusually large amounts of dipalmitoylphosphatidylcholine (DPPC); however, at the time, the association between DPPC and the surface-active properties of the alveolar wall was not known. In 1947, Gruenwald13 reported that resistance to aeration is caused by ST interfering with the entrance of the air, and surface-active substances were shown to reduce the pressure required for lung aeration. In the 1950s, Clements14 and Macklin15 experimentally demonstrated that PS influences the ST in lung volume.
As the pathophysiological mechanism in RDS, the lack of PS in actual clinical practice was first described by Avery and Mead1 in 1959. They found that the lungs of a neonate who died of RDS had a higher ST than those of neonates who died of non-RDS causes, and it was related to the absence or late emergence of some substances that render the internal surface capable of obtaining a low ST when the lung volume decreases in normal subjects. This was the first research to identify the cause of RDS. In 1963, Patrick Bouvier Kennedy, son of John F. Kennedy, former President of the United States, was born with RDS and a birth weight of only 1,860 g at 34 weeks of gestation; he died on the third day of life. The case was highlighted by the media, ultimately leading to the establishment of a large research support system in the United States for RDS research and therapeutic drug development. In fact, this provided significant momentum to the development of artificial therapeutic PS drugs in the 1980s.16
In a clinical study in 1965, Chu17 used nebulized DPPC as a spray method for the first time, but aerosolized DPPC was not effective and might worsen the clinical course of RDS. Due to the failure of this experiment, studies investigating artificial PS supplementation fell dormant for a while. In the 1970s, however, Enhörning and Robertson18 and Adams et al.19 reported that a natural PS formulation was effective in animal models of RDS. This had a significant impact on the basis for future preparations of PS. In the meantime, as PS studies continued, in 1973, King et al.20 described surfactant proteins (SPs), in addition to PLs, as structural components of PS, which play key roles in physical surface properties. In the 1980s, Hallman et al.21 described the administration of PS preparations isolated from human amniotic fluid.
Based on these studies, Fujiwara et al.,2 who were studying PS in the United States with the Adams team, returned to Japan and extracted PS from bovine lungs in 1980. They administered artificial PS in a formulation called surfactant-TA, a reconstituted PS supplement containing PLs, to 10 neonates with RDS (mean gestational age, 30 weeks; mean birth weight, 1,500 g). This was the first report to describe the successful use of an artificial PS preparation in the clinic and was a landmark contribution to the field.2 Fujiwara then won the Virginia Apgar Award, a neonatal research award from the American Academy of Pediatrics, and the King Faizal Medical Prize in Saudi Arabia for his work. Meanwhile, in Stockholm (Sweden), Bengt Robertson teamed up with Tore Curstedt to produce a porcine surfactant that they named after themselves: Curstedt–Robertson surfactant or “Curosurf.” This surfactant was isolated and produced from porcine lungs and underwent an additional preparation and purification step involving liquid gel chromatography.22
Artificial PS preparations currently in use worldwide
PS preparations are roughly categorized as natural PS preparations extracted from animals, such as cows or pigs, and synthetic preparations combining PLs alone or PLs with synthetic PS proteins. Natural products include Surfacten®, Survanta® (generic name as Beractant, AbbVie Inc., North Chicago, IL, USA), BLES® (generic name as CLSE, BLES Biochemicals Inc., London, Canada), Infasurf®, Alveofact® (generic name as Bovactant, Boehringer-Ingelheim Pharma, Ingelheim, Germany), and Curosurf®. Surfacten® and Survanta® are derived from modified bovine minced lung surfactant extracts with added DPPC, tripalmitoylglycerol, and palmitic acid. BLES®, Infasurf®, and Alveofact® are bovine lung lavage surfactant extracts obtained using chloroform–methanol extraction. Curosurf® is a porcine minced lung surfactant extract obtained using chloroform–methanol extraction and liquid-gel chromatography.2223 All natural PS preparations contain SP-B and CP-C, but the minced lung surfactants extracts (Survanta® and Curosurf®) contain less than 10% of the SP-B found in the lung lavage surfactant extracts (Infasurf®, Alveofact®, and BLES®).24
Current synthetic products without SPs are mixtures of various surface-active PLs and spreading agents.25 These products include ALEC® (generic name, Pumactant; Britannia Pharmaceuticals Ltd., Berkshire, UK) and Exosurf®, which have been used in the past and are no longer manufactured due to lack of natural surfactant components, particularly the hydrophobic SP-B and C.25 Synthetic products containing SPs generated through peptide synthesis and recombination technology function similar to the SP-B and C of native human surfactant.26 These products include Surfaxin® (generic name as Lucinactant, Discovery Laboratories, Warrington Township, PA, USA), which contains a chemically synthesized SP-B peptide called sinapultide (also known as KL4 peptide) combined with PLs and palmitic acid, and Venticure® (generic name as rSP-C Surfactant, Byk Gulden, Konstanz, Germany), which contains a recombinant SP-C combined with PLs and palmitic acid. However, clinical trials with these products were discontinued.2728
THE HISTORY OF PS IN KOREA
PS preparations used in Korea
In Korea, foreign PS preparations have been imported and used since 1991. The composition and characteristics of these preparations are summarized in Table 1. Since 1991, Surfacten® has been a component of readjusted natural PS from minced bovine lung extract with DPPC, tripalmitoylglycerol and palmitic acid, and contains SP-B, and -C. Imports have been discontinued since 2018, and are no longer available. Exosurf®, used from 1991 to 2008, was a synthetic PS of DPPC with 9% hexadecanol and 6% tyloxapol, which was not effective due to lack of SPs, and its production was discontinued in 2008. Curosurf®, imported from 2003, is a natural PS from minced porcine lung DPPC, subjected to chloroform–methanol extraction, purified by liquid-gel chromatography, and contains SP-B and -C, and is currently in use. Infasurf®, imported from 2007, had a short period of interruption and was imported again from 2017, is a natural PS from bovine lung lavage extract subjected to chloroform methanol extraction and contains SP-B, and -C. Newfactan®, a domestic product developed in Korea and used since 1996, has the same components as Surfacten®.
Table 1
Artificial PS preparations available in Korea

PS = pulmonary surfactant, SP = surfactant protein, DPPC = dipalmitoylphosphatidylcholine, PG = phosphatidyl glycerol.
![]()
Efforts and results for the development of PS replacement therapy
The Korean Society of Neonatology has hosted or sponsored numerous symposiums and seminars on PS replacement therapy (Table 2).72930 Since 1989, there have been many national and international communications on PS replacement therapy.
Table 2
Symposiums and seminars on PS replacement therapy hosted or sponsored by the Korean Society of Neonatology

S-Tx = surfactant treatment, RDS = respiratory distress syndrome, KSNR = Korean Society of Neonatal Research, KPS = Korean Pediatric Society, KSN = Korean Society of Neonatology, FAOPS = Federation of Asia and Oceania Perinatal Societies; Univ. = university.
![]()
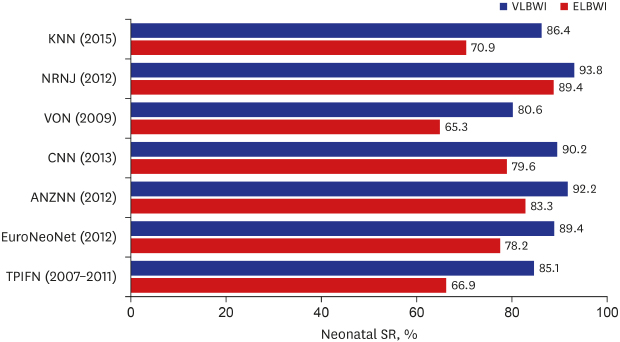
Before the formal importation of PS preparations into Korea in 1991, reports of pilot trials included those by Namgung et al.,31 in 1989, which involved eight cases, and Park et al.32 in 1991, involving six cases. After formal importation of PS preparations, the reports of outcomes of PS replacement therapy came from nationwide collective studies (total RDS patients who were admitted to the neonatal intensive care unit and who underwent PS replacement therapy without distinction according to birth weight), including those by Bae et al.33 in 1993 (60 patients in 16 hospitals), Bae et al.34 in 1997 (1,066 patients in 64 hospitals), Bae et al.35 in 2004 (1,596 patients in 62 hospitals), Bae et al.36 in 2009 (1,921 patients in 57 hospitals), and Bae et al.37 in 2011 (3,160 patients in 72 hospitals); the exception to these nationwide multicenter studies was one single-hospital study. Table 3 summarizes the results of these reports. The mortality rate for each year was 40.0% in 1990/1991, 28.7% in 1996, 18.7% in 2002, 14.3% in 2007, and 10.1% in 2010, clearly demonstrating the significant reduction in mortality. In 2014, Kim et al.38 published a report of nationwide research of early prophylactic and late selective use in RDS, showing that early prophylactic use was more effective than late selective use. Shim et al.8 reported changes in the survival rates of VLBWI and ELBWI in Korea before and after the introduction of PS. As shown in Fig. 1, the introduction of PS in 1991 contributed to improved survival rate, and the survival rates for 2010–2014 were reported to be 84.8% in VLBWI and 69.6% in ELBWI. Chung and Bae9 compared the survival rates of VLBWI and ELBWI in the KNN data in 2015 with data from western developed countries. Fig. 2 reveals that the levels were similar to those in the United States and Taiwan, which were slightly below those in Japan, Canada, Australia, New Zealand, and Europe.
Table 3
PS replacement therapy for neonatal RDS and mortality rates in Korea
Mortality rates were defined as the percentage of neonates with PS replacement therapy for RDS who died within 28 days of birth.
PS = pulmonary surfactant, RDS = respiratory distress syndrome.
![]()
 | Fig. 1Changes of neonatal SRs for VLBWI and ELBWI in Korea (1960–2014.6). Data adapted from Shim et al.8SR = survival rate, ELBWI = extremely low birth weight infants, VLBWI = very low birth weight infants.
aP < 0.05 vs. late 1960s; bP < 0.001 vs. late 1960s; cP < 0.05 vs. late 1960s; dP < 0.001 vs. late 1960s.
|
 | Fig. 2Comparison of the neonatal SRs of VLBWI and ELBWI between Korea, Japan, US, Canada, Europe, Australia and New Zealand, and Taiwan. Data adapted from Chung et al.9SR = survival rate, VLBWI = very low birth weight infants, ELBWI = extremely low birth weight infants, KNN = Korean Neonatal Network, NRNJ = Neonatal Research Network of Japan, VON = Vermont Oxford Network; CNN = Canadian Neonatal Network, ANZNN = Australian and New Zealand Neonatal Network, EuroNeoNet = European Neonatal Network, TPIFN = Taiwan Premature Infant Follow-up Network.
|
There have been changes in the ways PS is administered. One focus of current research is the use of less invasive approaches. Tracheal intubation has been performed for PS administration in most premature babies; however, it is now known that positive pressure ventilation should be avoided as much as possible to minimize lung injury.39 The less invasive surfactant application (LISA) protocol developed by Kribs et al.40 preserves spontaneous breathing and avoids mechanical ventilation. It allows spontaneous breathing by combining PS administration and continuous positive airway pressure (CPAP). PS is delivered during CPAP via a thin catheter. In Korea, some studies have suggested that the early application of CPAP for RDS treatment is effective and can reduce the occurrence of lung injury via the Intubate-SURfactant-Extubation technique. However, there has been little research on LISA.4142
The history of insurance benefit for PS replacement therapy in Korea
In 1991, the first imported PS preparations were not initially covered by insurance in Korea. Insurance started covering single doses in February 1992 and multiple doses in October 2007.5 Since January 2011, early PS replacement therapy (early prophylactic therapy, which is administered within 2 hours of birth in very preterm infants to prevent RDS, has already been proven to improve the prognosis in other countries) started to be covered by insurance.5 The criteria for early treatment are as follows: premature babies with a birth weight < 1,250 g or a gestational age < 30 weeks, and a single administration within 2 hours after birth. Recent changes in the standard of insurance benefits for neonatal RDS in Korea are described in Table 4.
Table 4
The most recent basis for insurance benefits for PS replacement therapy in Korea (January 1, 2019)

![]()
FUTURE DIRECTIONS OF PS RESEARCH IN KOREA
The existing PS formulation is a natural formulation extracted from the lungs of animals (cows or pigs). To avoid the use of preparations of animal origin, research is underway to develop synthetic preparations that are similar to human PS. Bae et al.43 published an in vitro experiment describing a new generation of synthetic PS conjugated to DPPC and PG using a synthetic peptide of SP-C (CPVHLKRLLLLLLLLLLLLLLLL), and an effective PS formulation in in vivo experiments in a fetal rabbit model of RDS. Choi et al.44 developed further new-generation SP-C synthetic peptide and SP-B peptide (RMLPQLVCRLVLRCSMD), which had been originally developed by Bae et al.43 Additional investigations on various fields are required based on the outcome of this basic work. Evaluating the bioactivity and metabolic fate of peptide-based SP are important for understanding the clearance mechanism of synthetic PS in the lungs. This use of synthetic PS, and not an animal extract, is anticipated to result in mass production and price reduction with significant consequences in clinical application.
As new methods of minimally invasive PS administration are developing, prophylactic PS replacement therapy with LISA may have a benefit over CPAP with rescue administration of PS with LISA. Currently, the indications and methods of LISA are not established. Less invasive methods of PS administration should be studied, including type of PS, dose of PS, indication for multiple PS administrations, and less invasive catheters, in order to achieve maximum performance in patients with RDS.
SUMMARY
The present review provides information regarding the history of RDS treatment in Korea, including a formal definition of the disease, establishment of its pathophysiology, the development of various artificial PSs, the management of a registry network, and the organization of health insurance policies. PS represents the backbone of the exceptional survival of ELBWI. A generational change is occurring in the era of PS, which is anticipated to contribute to better outcomes and lower complication rates rather than merely infant survival itself. Physicians, neonatologists, nurses working at neonatal intensive care units, and scientists must persevere to overcome the remaining hurdles, such as an animal protein-free synthetic PS, new drug delivery methods, lowering treatment costs, and establishing more efficient and equitable policies for premature newborn infants.
 XML Download
XML Download