

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Peri-implantitis is an inflammatory reaction associated with loss of the supporting bone around an implant during functional processes [1]. In re-osseointegration, which is the ultimate objective in the treatment of peri-implantitis, cellular responses to the titanium surface are important. The reaction of cells to titanium depends on its surface characteristics, such as topography and the elemental composition of the implant [2].
Since loss of supporting bone around the implant occurs after bacterial infection, complete surface decontamination must be performed as the primary step [3]. However, decontamination affects the surface of the implant. The surface roughness of instrumented titanium is affected by the instrument materials and material hardness [4]. Remnants of the plastic scaler might disturb cell attachment and proliferation [56], and chemical agents might affect the elemental composition of the titanium surface [7]. Therefore, the decontamination procedure may adversely affect the biocompatibility of the titanium surface of the implant in comparison to the pristine titanium of newly purchased commercial implants.
However, very few studies have sought to characterize changes in the biocompatibility of titanium after decontamination. Most such studies have reported reduced biocompatibility of decontaminated titanium surfaces [2], whereas other studies failed to find any significant change in the biocompatibility of titanium after decontamination using an air-powder abrasive system [89]. These conflicting results may be attributable to differences in experimental conditions, including the decontamination methods, titanium surface, and the cell types used in those studies.
Therefore, the aim of this study was to comprehensively evaluate the cytocompatibility of titanium surfaces decontaminated by various methods. To test biocompatibility, salivary bacterial contamination with dental pellicle formation was used to reproduce the clinical situation in vitro.
MATERIALS AND METHODS
This study was approved by the Institutional Review Board of Seoul St. Mary's Hospital, College of Medicine, the Catholic University of Korea, Seoul, Republic of Korea (KC16TNSI0644).
Preparation of samples and chemical analysis
Grouping
Table 1 shows the groups categorized according to the surface treatment. Three control groups were used in this study. Pristine sand-blasted and acid-etched (SA) titanium disks were completely untreated in the SA group. The pellicle group was treated with only a salivary pellicle coating. The third (biofilm-coated, untreated SA disks [NT]) group was not decontaminated after salivary pellicle formation and bacteria growth. The 14 treatment groups were decontaminated with ultrasonic and rotating devices, an air-powder abrasive system, a laser, and chemical agents.
Table 1
Details of the decontamination treatments used in this study

EM: EMS metal, EP: EMS plastic, SM: Satelec metal, SP: Satelec plastic, ST: Satelec titanium, iB: iBrush, Ti: Tigran brush, GB: GingiBrush, Pf: Perioflow, CA: citric acid, Tc: tetracycline, NT: no treatment, SA: sand-blasted and acid-etched, Er,Cr:YSGG: erbium, chromium: yttrium-scandium-gallium-garnet, EDTA: ethylenediaminetetraacetic acid.
Titanium disks
In this study, SA titanium disks (Osstem, Busan, Korea) were used. The disk diameter was 12 mm and the thickness was 1 mm. The disks were initially sterilized by gamma irradiation before use in the experiments.
Salivary pellicle preparation
Saliva was obtained from a healthy volunteer. The saliva was diluted 2-fold with phosphate-buffered saline (Welgene, Daegu, Korea) and filtered through a 0.2 µm filter (Sartorius, Gottingen, Germany). Except for those in the SA group, all disks (4 disks per group) were coated with filtered saliva solution and dried in a desiccator for 24 hours. All disks were then sterilized with 24 hours of ultraviolet (UV) irradiation.
Biofilm formation
Biofilm formation was initiated on the disks of all groups, except those in the SA and pellicle groups. Saliva from the same healthy volunteer was diluted 4-fold in brain heart infusion (BHI) broth (BD Biosciences, San Jose, CA, USA) containing 2% sucrose and 2% mannose, and then vortexed for 20 seconds. The saliva and BHI mixture was centrifuged at 1,000×g at room temperature for 5 minutes to remove debris. The supernatant was used for biofilm formation. The pellicle-coated titanium disks (except those in the SA and pellicle groups) were incubated with the supernatant in an anaerobic CO2 incubator for 48 hours.
Titanium disk preparation
All decontamination treatments were performed by a single researcher (YK). Table 1 shows the grouping of the disks according to the decontamination methods. The disks treated with an ultrasonic instrument were divided into 5 groups based on the use of 2 metal tips (EM; EMS Piezon System, EMS, Nyon, Switzerland/SM; Satelec, Mérignac, France), 2 plastic tips (EP; polyetherether-ketone tip, EMS Piezon Systems/SP; Satelec), or 1 titanium tip (ST; Satelec). Ultrasonic instrumentation was performed as described in a previous study [10]. The tip was angulated tangentially and placed with minimal lateral pressure on the disk. A power setting of 1 was applied at 25–32 kHz in the EM and EP groups, and a power setting of 2 was used at 28–33 kHz in the SM, SP, and ST groups on P5 Newtron (Satelec) unit [10].
Disks treated with a rotating instrument were divided into 3 groups based on the use of stainless steel (iB; iBrush, Neobiotech, Seoul, Korea), titanium (Ti; Tigran PeriBrush, Tigran Technologies AB, Malmö, Sweden), or nylon (GB; GingiBrush, Neobiotech). Rotating instrumentation was performed for 40 seconds as previously described [11], at rpm settings recommended by the manufacturer. The titanium brush was used at 300 rpm and the stainless steel brush at 1,000 rpm under irrigation. The operator took care to apply the minimum possible lateral pressure during instrumentation. An air-abrasive system (Pf; Air-Flow® PERIO, EMS) with glycine powder (Air-Flow® PERIO powder) was applied with a plastic nozzle for 10 seconds.
For the laser treatment, the disks were treated with an erbium, chromium: yttrium-scandium-gallium-garnet (Er,Cr:YSGG) laser (Waterlase iPlus, Biolase, Irvine, CA, USA). The power was set at 2.50 W in the 25 Hz mode (S). The operation mode was the pocket therapy open setting with 50% air and 50% water. Disk treatment was performed for 40 seconds.
The disks subjected to chemical decontamination were divided into 4 groups based on whether they were treated with 3% H2O2 (H2O2; Green Pharmaceutical Co., Jincheon, Korea), 50% citric acid (CA; pH 1.0, Sigma-Aldrich Co., St. Louis, MO, USA), 24% ethylenediaminetetraacetic acid (EDTA; pH 7.1, Biosesang, Seongnam, Korea), or tetracycline HCl (Tc; 50 mg/mL, Sigma-Aldrich Co.). Disks were treated by 20 back-and-forth strokes using cotton pellets soaked in the respective chemical agent.
Cell culture
The human osteoblast-like MG63 cell line (MG63; ATCC® CRL-1427™, ATCC, Manassas, VA, USA) was used in all cell culture experiments. The treated titanium disks were sterilized in UV light for 72 hours. The MG63 cells were seeded in 24-well cell culture plates (Corning, Tewksbury, MA, USA) with a titanium disk at a density of 2×104 cells/well and incubated for 24 hours at 37°C in a humidified incubator with 5% CO2 and 95% air. The next day, the 24-well culture plate was replaced with a new 24-well culture plate. The cells were incubated for 5 days. Dulbecco's Modified Eagle Medium (Hyclone, Logan, UT, USA) containing 10% fetal bovine serum (Gibco, Grand Island, NY, USA), penicillin (100 U/mL, Sigma-Aldrich Co.) and streptomycin (100 µg/mL, Sigma-Aldrich Co.) was used as the culture medium. Three disks per instrumentation type or control were used for the experiment after the use of 1 disk per group for EDS.
Cell proliferation assay
The cell proliferation analysis was performed using the Cell Counting Kit-8 (CCK-8; Dojindo Molecular Technologies Inc., Gaithersburg, MD, USA). The analysis was performed on days 2 and 5 of cell culture, according to the manufacturer's protocol.
Cell morphology analyses
The MG63 cells were seeded in 24-well plates with a titanium disk at a density of 2×104 cells/well. The next day (after 24 hours), the 24-well culture plate was replaced with a new 24-well culture plate and the cells were incubated for 5 days.
Immunofluorescence
All samples were fixed with 4% paraformaldehyde (Sigma-Aldrich Co.) and stained with rhodamine-phalloidin (Molecular Probes, Eugene, OR, USA) and 4′,6-diamidino-2-phenylindole (DAPI; Sigma-Aldrich Co.). The samples were observed under a fluorescence microscope (Axiovert 200, Zeiss, Oberkochen, Germany).
Scanning electron microscopy (SEM)
All samples were fixed with 2.5% glutaraldehyde (Sigma-Aldrich Co.). The samples were dehydrated in 50%, 60%, 70%, 90%, 95%, and 100% ethanol, dried with hexamethyldisilazane, and coated with carbon gold alloy. All samples were observed under a SEM (S-4700, Hitachi, Tokyo, Japan).
Vascular endothelial growth factor (VEGF) assay
A commercial VEGF assay kit (Quantikine ELISA, R&D Systems, Minneapolis, MN, USA) was used. The MG63 cells were seeded in 24-well plates with a titanium disk at a density of 2×104 cells/well. The next day (after 24 hours), the 24-well culture plate was replaced with a new 24-well culture plate and the cells were incubated for 5 days. The supernatant medium from the cell culture was used for the VEGF assay according to the manufacturer's protocol.
Statistical analyses
Data from EDS were expressed as the weight percent and the atomic percent. All data in this study, except EDS, were expressed as the mean±standard deviation. The measurements were taken in duplicate. The Tukey multiple comparison test following 1-way analysis of variance was used to analyze the cell proliferation and VEGF data. Commercially available statistical software (GraphPad Prism 7, GraphPad Software, San Diego, CA, USA) was used in this study. The level of statistical significance was set at P<0.05.
RESULTS
Chemical composition of the disk surfaces
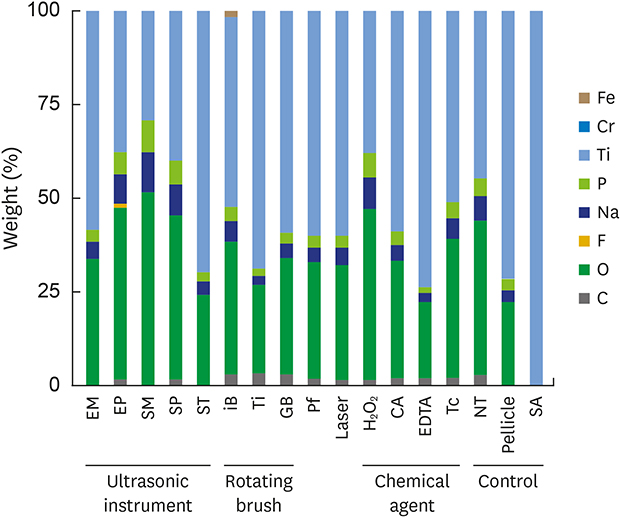
Figure 1 shows the results of the EDS analysis of the disk surfaces. As expected, the SA group was composed of only titanium on the surface. Unlike the SA group, the surfaces of the treated samples showed changes in the chemical composition. Oxygen was most abundant on the instrumented surfaces (weight percent: 20.36%–51.58%; atomic percent: 40.63%–70.4%). Carbon was detected in the majority of the instrumented and NT groups (weight percent: 1.4%–3.34%; atomic percent: 2.68%–8.29%). However, carbon was not detected in the metal- and titanium-instrumented groups (EM, SM, and ST groups). An iron component was found only in the iB group (weight percent: 1.52%; atomic percent: 0.69%).
Figure 1
EDS of the treated titanium disks. (A) Chemical composition (weight percent) of the prepared disks. (B) Chemical composition (atomic percent) of the prepared disks.
EM: EMS metal, EP: EMS plastic, SM: Satelec metal, SP: Satelec plastic, ST: Satelec titanium, iB: iBrush, Ti: Tigran brush, GB: GingiBrush, Pf: Perioflow, CA: citric acid, Tc: tetracycline, NT: no treatment, SA: sand-blasted and acid-etched, EDS: energy-dispersive X-ray spectroscopy, EDTA: ethylenediaminetetraacetic acid.

Cell proliferation
Figure 2 shows the results of the CCK-8 assay on days 2 and 5. Cell proliferation was significantly higher in the Ti (1.27±0.14), GB (1.1±0.16), and laser (1.23±0.14) groups than in the SA group (0.74±0.04) on day 2 (Figure 2A). The cell proliferation in the Ti (1.27±0.14) and laser (1.23±0.14) groups was significantly higher than in the NT group (0.82±0.14) and was significantly lower in the Tc group (0.44±0.05) than in the NT group (0.82±0.14) on day 2 (Figure 2A). On day 5, cell proliferation was significantly lower in all the decontaminated disks (mean, 1.14±0.31), except for the 2 groups treated using a plastic tip, than in the SA group (2.08±0.07; Figure 2B). In addition, on day 5, the EP (1.51±0.33), SP (1.41±0.17), Tc (1.31±0.03), H2O2 (1.35±0.07), and CA (1.57±0.03) groups showed higher cell proliferation than did the NT group (0.57±0.08; Figure 2B).
Figure 2
Cell proliferation analysis. The Cell Counting Kit-8 assay was performed on days 2 and 5. (A) Cell proliferation on day 2. Cell viability in the Ti, GB, and laser groups was significantly higher than in the SA group. (B) Cell proliferation on day 5. Cell viability in 14 groups (EM, SM, ST, iB, Ti, GB, Pf, laser, H2O2, CA, EDTA, Tc, NT, and pellicle) was significantly lower than in the SA group.
EM: EMS metal, EP: EMS plastic, SM: Satelec metal, SP: Satelec plastic, ST: Satelec titanium, iB: iBrush, Ti: Tigran brush, GB: GingiBrush, Pf: Perioflow, CA: citric acid, Tc: tetracycline, NT: no treatment, SA: sand-blasted and acid-etched, OD: optical density, EDTA: ethylenediaminetetraacetic acid.
a)Significantly different from the SA group (P<0.05); b)Significantly different from the NT group (P<0.05).

Cell morphology
Immunofluorescence
Figure 3 shows the immunofluorescence images of cell morphology, as indicated by F-actin and nuclear staining, on day 5. Cell density was observed to be lower in the Ti, NT, and pellicle groups than in the other groups. This result was consistent with the CCK-8 assay (Figure 2B).
Figure 3
Morphology of the cells under immunofluorescence microscopy. The F-actin in cells was stained by rhodamine-phalloidin. Nuclei were stained with DAPI.
EM: EMS metal, EP: EMS plastic, SM: Satelec metal, SP: Satelec plastic, ST: Satelec titanium, iB: iBrush, Ti: Tigran brush, GB: GingiBrush, Pf: Perioflow, CA: citric acid, Tc: tetracycline, NT: no treatment, SA: sand-blasted and acid-etched, DAPI: 4′,6-diamidino-2-phenylindole, EDTA: ethylenediaminetetraacetic acid.

Scanning electron microscope
Figure 4 shows the SEM images of cell morphology on day 5. All groups showed well-attached cells, except the NT group. Cells were not observed in the NT group, and extensive bacterial residue was observed.
Figure 4
Morphology of the cells under scanning electron microscopy. The scale bar in the figures indicates 40 μm and 20 μm.
EM: EMS metal, EP: EMS plastic, SM: Satelec metal, SP: Satelec plastic, ST: Satelec titanium, iB: iBrush, Ti: Tigran brush, GB: GingiBrush, Pf: Perioflow, CA: citric acid, Tc: tetracycline, NT: no treatment, SA: sand-blasted and acid-etched, EDTA: ethylenediaminetetraacetic acid.

VEGF assay
Figure 5 shows the results of the VEGF assay. Cells grown in the presence of the Tc (1.97±0.16) and NT (1.79±1.39) disks showed significantly lower VEGF production than those grown with the disks from the SA group (4.73±0.69).
Figure 5
VEGF assay at day 5. The VEGF level in the Tc and NT groups was significantly different from that in the SA group.
VEGF: vascular endothelial growth factor, EM: EMS metal, EP: EMS plastic, SM: Satelec metal, SP: Satelec plastic, ST: Satelec titanium, iB: iBrush, Ti: Tigran brush, GB: GingiBrush, Pf: Perioflow, CA: citric acid, Tc: tetracycline, NT: no treatment, SA: sand-blasted and acid-etched, EDTA: ethylenediaminetetraacetic acid.
a)Significant difference (P<0.05).

DISCUSSION
The surface characteristics of implants, particularly variations in their micro- and nano-structures, affect the extent and quality of osseointegration, as reflected by parameters such as bone-to-implant contact [12]. Unfortunately, in cases of peri-implantitis, contamination by bacteria and their secretions has deleterious effects on the biocompatibility of the implant. Many decontamination methods have been used to restore biocompatibility, such as ultrasonic devices, rotating instruments, air-powder abrasive systems, lasers, and chemical agents. However, none have shown particularly superior results [3111314]. Recently, metal and non-metal curettes were shown to be ineffective in removing bacteria from machined and sandblasted, large grit, acid-etched surfaces [15]. Thus, metal and non-metal curettes were excluded from the present study; we found that most decontamination methods failed to restore the biocompatibility of titanium surfaces to a level comparable to that of the pristine SA titanium surface (Figure 2B). This result is consistent with most previous studies using osteoblast-like cells [5161718].
Although the results vary depending on the instrument, many studies have investigated topographical changes of titanium surfaces after instrumentation [1920]. Altered surface topography may adversely affect cell proliferation and cell response. In particular, osteoblast-like cells exhibit roughness-dependent phenotypic characteristics [21]. They tend to attach more easily to surfaces with rougher microtopography and show better characteristics on rougher surfaces in terms of morphology, extracellular matrix synthesis, and alkaline phosphatase activity [21].
Altered chemical composition may also adversely affect cell proliferation. In our study, EDS analysis revealed that decontamination procedures changed the chemical composition of the titanium surface (Figure 1). Although the mechanism is not clear, previous studies have suggested that the biocompatibility of implants is related to the surface chemical composition [212223]. The chemical composition is believed to be important because most cells establish a chemical attachment between the titanium oxide layer and the cell surface glycoproteins [24]. The altered chemical composition may have been due to debris from the instrument deposited on the surface. In the present study, iron was identified on the surface of the iB group, which may have been debris from the stainless steel bristles of the iBrush (Figure 1).
The results of our study, most decontamination methods have shown a tendency to restore the biocompatibility of decontaminated surfaces compared to untreated, contaminated surfaces (Figure 2B). In our experiments, all disk samples were sterilized by UV radiation. Thus, the decreased biocompatibility compared to pristine surface observed in our study might have been due to changes in the characteristics of the titanium surface, rather than the toxic effects of bacteria.
The pellicle-coated surfaces showed less cell proliferation than the SA group (Figure 2B). The MG63 cells showed less cell density and oval-shaped morphology in the pellicle group (Figure 3). The decrease in cell spreading on the pellicle-coated disks might have been due to multiple causes. On the one hand, the pellicle coating is likely to have affected the topography of the disk surface. The saliva solution was dried on the disk surface for 24 hours during the coating procedure. The dried pellicle might have affected the topography of the titanium disk. On the other hand, the pellicle allows selective attachment of cells or bacteria. The dental pellicle contains a variety of receptors, such as salivary glycoproteins and antibodies [25]. Some bacteria possess adhesins complementary to the pellicle receptors, which enable them to attach rapidly upon contact [25]. Other bacteria require prolonged exposure to adhere firmly [25]. Likewise, cells without adhesins might also require more time to attach to the dental pellicle than to pristine titanium.
VEGF production by the cells was lower in the Tc and NT groups than in the other groups (Figure 5). This result is consistent with previous studies reporting that tetracycline exhibited anti-angiogenic activity and could downregulate VEGF [2627]. Tetracycline has non-antimicrobial properties, of which inhibition of matrix metalloproteinases (MMPs) has been most widely documented [27]. MMPs are upregulated in angiogenesis, and MMP-9 may activate VEGF in vivo and in vitro [28]. Thus, tetracycline may have the effect of inhibiting angiogenesis and VEGF formation via inhibition of MMPs.
In summary, no decontamination method was found to be clearly superior in terms of restoring the biocompatibility of the treated titanium surfaces, and the biocompatibility of the pristine SA titanium surface could not be regained. This suggests that prevention of peri-implantitis is crucial, and that the original biocompatibility of implants deteriorates irreversibly in peri-implantitis. However, most of the methods improved the biocompatibility of the titanium surfaces when compared to the untreated surfaces. This suggests that decontamination is an indispensable element of peri-implantitis treatment, even if the original biocompatibility cannot be entirely restored. In this study, tetracycline showed negative effects on VEGF production by MD-63 cells. VEGF is an essential factor in the early healing process. Thus, caution is needed when using tetracycline in the decontamination process. In addition, it is recommended that saliva be eliminated from the fixture surface during decontamination. Alterations of disk topography were not evaluated in this study. Further research on topographical changes is needed to clarify the cause of the decrease in biocompatibility.
 XML Download
XML Download