

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Immediate implant placement after tooth extraction has been shown to yield implant survival rates similar to those of delayed implant placement [12], and immediate replacement has been reported to be convenient for the patient because it shortens the treatment time [3]. Although the timing of implant placement does not itself necessarily affect the implant survival rate, other parameters appear to be more clinically relevant in the decision-making process regarding the choice of a specific time-point for implant placement. Among those factors, the preservation of hard and soft tissues—with implications for esthetic outcomes—can be affected by the timing of implant placement [45].
Contour changes, as a consequence of resorption and remodeling processes at the extraction site following tooth extraction and immediate implant placement, predominantly result in (partial) loss of the buccal bone wall [67] and the frequent development of buccal mucosal dehiscence [8].
Various therapeutic concepts have been developed to minimize the above-mentioned changes following immediate implant placement, including hard tissue grafting, soft tissue grafting, and immediate provisionalization [9].
Most commonly, the gap between the facial bone wall and the implant is grafted with a bone substitute material. This approach has been demonstrated to decrease the buccolingual resorption rate of the bone [1011], thereby providing tissue stability. The use of a connective tissue graft in conjunction with an immediately placed implant can further support tissue stability, leading to a more stable marginal mucosal level and less recession [121314]. It has also been speculated (and, to some extent, proven) that immediate provisionalization supports the peri-implant soft tissues in a beneficial way by yielding higher soft tissue thickness and height, as well as stable papillae levels [151617].
Limited data are currently available on the additional benefits of hard tissue grafting, soft tissue grafting, and/or immediate provisionalization for peri-implant tissue stability at immediate implant sites.
The aim of the present study was therefore to evaluate the effects of intra-alveolar socket grafting, subepithelial connective tissue grafting, and individualized abutments on peri-implant hard and soft tissue outcomes following immediate implant placement.
MATERIALS AND METHODS
This study was designed as a randomized experimental study employing 5 mongrel dogs, and was approved by the local ethics committee (2017-0332). The study was performed at Yonsei University, Seoul, Korea, according to the local guidelines of animal keeping. The data analysis was performed at the Clinic for Fixed and Removable Prosthodontics and Dental Material Science at the University of Zurich. Prior to the beginning of the study, the experimental protocol (performed according to the ARRIVE—Animal research: reporting in vivo experiments—guidelines [18]) was approved by the local ethics committee.
Surgical procedures
All surgical procedures were performed under local anesthesia in an operating room. On the day of surgery, the dogs were premedicated with cefazolin (20 mg/kg, intravenous) and meloxicam (1 mg/kg, subcutaneous). Subsequently, general anesthesia was induced by injection of Zoletil (5 mg/kg, intravenous) and Rompun (2 mg/kg, intravenous). Isoflurane (1.5%–2%) and O2 (100%) were used as inhaled anesthetics. The animals were routinely monitored and further analgesia was given if necessary within the first days following all surgical procedures.
Extractions
After disinfection of the surgical site with 0.2% chlorhexidine solution (Hexamedine; Bukwang Pharmaceutical, Seoul, Korea), local anesthetics (lidocaine HCl [2%] with epinephrine [1:100,000]; Huons, Seongnam, Korea) were administered by infiltration at the respective buccal and lingual sites. On both sides of the mandible, the mesial roots of P3 and P4 were extracted. Root canal treatment was performed for the distal roots of P3 and P4.
Implant placement
Immediate 2-piece dental implants (Neobiotech, Seoul, Korea) were placed slightly lingually of the center of the extraction socket, without raising a flap and with the implant shoulder (IS) placed flush with the lingual bone crest (lBC). The horizontal and vertical position of the implant was recorded. Subsequently, the following 4 treatment modalities were randomly applied to the 4 sites in the lower jaw (mesial roots of P3 and P4 on both sides):
• Standardized healing abutment: control group
• Alloplastic bone substitute material (BSS) + standardized healing abutment: SA group
• BSS + individualized healing abutment: IA group
• BSS + subepithelial connective tissue graft (SCTG) + individualized healing abutment: IAG group
In the control group, a standardized healing abutment was connected to the implant. In the SA, IA, and IAG groups, an alloplastic bone substitute material (polylactic-co-glycolic acid–coated biphasic calcium phosphate particles consisting of 60% hydroxyapatite [HA] and 40% beta-tricalcium phosphate [β-TCP]) (GUIDOR easy-graft CRYSTAL; Sunstar Suisse SA, Etoy, Switzerland), was applied to fill the intra-alveolar bone defect between the walls of the extraction site and the implant. In the SA group, a standardized healing abutment was placed. In the IA and IAG groups, an individualized healing abutment was positioned. The healing abutment was modified to create an optimal emergence profile mimicking that of a natural tooth using flowable composite. The buccal height of the individualized healing abutment was slightly higher than the margo mucosae (MM). In the IAG group, an SCTG was harvested from the palate and placed on the buccal side of the implant site. For that purpose, a split-thickness flap was prepared on the buccal side of the extraction socket. Sutures were used to stabilize the graft. In all groups, the implants were left to heal transmucosally. Sutures were removed 7–10 days later.
Sacrifice
Following a healing period of 4 months, all dogs were painlessly sacrificed using an overdose of pentobarbital. The implants and surrounding soft tissues were macroscopically inspected. Local inflammation, necrosis, hemorrhage, dehiscence, or the presence of any other lesion was recorded. Following dissection, the 2 hemimandibles were block-resected and fixed by immersion in 10% formaldehyde in phosphate buffer at pH 7.
Clinical measurements
Clinical measurements were recorded in millimeters with a caliper after immediate implant placement and after sacrifice. These measurements included the distance from the top of the healing abutment to the buccal and lingual MM post-implant placement and at sacrifice. Moreover, the change in the distance between those 2 time-points was calculated and recorded as the primary outcome (Figure 1).
Figure 1
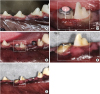
Clinical case from the IA and SA treatment groups at (A) baseline (before tooth extraction), (B) post-implant placement, and at (C) sacrifice. The dashed-line rectangle shows the P3 site corresponding to group IA at (D) post-implant placement and (E) sacrifice. The line with arrows shows the distance from the top of the healing abutment to the margo mucosae on the buccal side of the implant.
Histological preparation
X-rays were taken of each site in order to accurately determine the cutting planes. The 20 sites (4 per animal) were fixed in buffered 4% formaldehyde solution, followed by dehydration, and embedded in a methyl methacrylate solution (Sigma-Aldrich M55909-1L).
The tissue blocks were cut into 200-µm-thick sections using a diamond band saw (Exakt Apparatebau, Norderstedt, Germany). The sections were ground and polished to a thickness of 60–80 µm. All the sections were stained with Van Gieson Elastica (VG-El).
Histomorphometric analyses
For the histomorphometric analyses, digital images were evaluated using Leica Application Suite (LAS) version 4.3 (Leica Mikrosysteme, Wetzlar, Germany) and for the first round of image processing, Photoshop CS6 was used (Adobe Inc., San Jose, CA, USA). All images were photographed with a Leica DM6000 B microscope (Leica Mikrosysteme, Wetzlar, Germany) and a Leica DFC 450 digital camera (Leica Mikrosysteme, Wetzlar, Germany). The digital software used to make the histological linear measurements was the LAS version 4.3 Interactive Measurement Module (Leica Mikrosysteme). All measurements were performed by 2 blinded examiners, and thereafter compared and discussed to establish a consensus.
The following histomorphometric landmarks were identified at sacrifice (Figure 2):
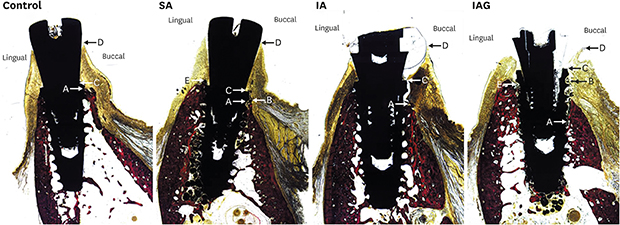
Figure 2
Histological slides of all 4 groups (control, SA, IA, and IAG) at sacrifice. (A) The first bone-to-implant contact on the buccal side. (B) The buccal bone crest or the most coronal location of bone substitute particles. (C) The implant shoulder on the buccal side. (D) The most coronal level of the margo mucosae on the buccal side. (E) The lingual bone crest.
SA: alloplastic bone substitute material + standardized healing abutment, IA: alloplastic bone substitute material + individualized healing abutment, IAG: alloplastic bone substitute material + individualized healing abutment + a subepithelial connective tissue graft.

• First bone-to-implant contact (fBIC) on the buccal side (Figure 2A)
• Buccal bone crest (bBC) or the most coronal location of bone substitute particles on the buccal side (Figure 2B)
• IS on the buccal side (Figure 2C)
• Most coronal level of the MM on the buccal side (Figure 2D)
• lBC (Figure 2E)
The following distances were calculated on the buccal side of the implant at sacrifice: height from the margo mucosae to the implant shoulder (MM-IS), height from the margo mucosae to the first bone-to-implant contact (MM-fBIC), height from the margo mucosae to the buccal bone crest (MM-bBC) or the most coronal location of bone substitute particles on the buccal side, and height from the margo mucosae to the lingual bone crest (MM-lBC). All these measurements were recorded in millimeters.
Profilometric analysis
Prior to tooth extraction, following implant placement, and at sacrifice, digital impressions of the implant sites and the 2 neighboring teeth were made. The profilometric analysis was performed by superimposing the surface scans of the 3 time-points and analyzing the volumetric and contour changes of the peri-implant tissues. This was carried out through digital software (SMOP, Swissmeda AG, Baar, Switzerland) at the University of Zurich.
The following measurements were made at the buccal aspect of the implant sites: volumetric changes from baseline (before tooth extraction; B) to post-implant placement (B-pIP), from baseline to sacrifice (B-S), and from post-implant placement to sacrifice (pIP-S). These volumetric changes were calculated by defining a rectangular region measuring 3 mm in width and 1 mm in height at the level of the soft tissue margin of the superimposed scans. The digital software was able to calculate an average of the multiple thicknesses between both scans in this rectangular area at different time-points, and recorded it in millimeters (Figure 3).
Figure 3
Digital analysis of surface scans at (A, B) baseline, (C, D) post-implant placement, and (E, F) sacrifice at an implant site from the control group. The orange rectangle corresponds to the area of interest, measuring the overall volume change defined in that region. (G) The volume of interest in a sagittal 2-dimensional cut between baseline and sacrifice.

Horizontal changes at the level of the MM, and at 1 mm and at 3 mm below the MM from baseline (prior to extraction) to sacrifice were calculated.
Statistical analysis
Continuous variables were described using mean values, standard deviations, median values, and quartiles.
Intergroup differences were analyzed by nonparametric mixed models, and in case of a significant result, multiple pairwise comparisons of the groups were made using the Bonferroni correction. However, because of the small sample size, the power of the pairwise comparisons was quite low. P values <0.05 were considered to indicate statistical significance. Intragroup differences (showing time effects) could not be statistically analyzed due to the limited number of dogs (5).
RESULTS
All animals remained healthy during the study period, and no wound healing complications or local infections were observed. Nonetheless, 1 implant failed in dog #2, and 3 implants failed in dog #5 (all during the early healing period).
Clinical outcomes
All clinical measurements are reported in Table 1 at baseline (before tooth extraction), post-implant placement, and at the time of sacrifice.
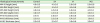
Table 1
Clinical measurements of the treatment groups

SA: alloplastic bone substitute material + standardized healing abutment, IA alloplastic bone substitute material + individualized healing abutment, IAG: alloplastic bone substitute material + individualized healing abutment + a subepithelial connective tissue graft, HA-bMM: distance from the top of the healing abutment to the buccal margo mucosae, bMM: buccal margo mucosae, pIP: post-implant placement, S: sacrifice, HA-lMM: distance from the top of the healing abutment to the lingual margin mucosae, lMM: lingual margo mucosae.
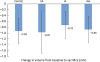
The primary outcome was the mean change of the level of the buccal MM in relation to the healing abutment from post-implant placement to sacrifice. The level of the buccal MM in the control group showed a coronal shift of 0.88±0.48 mm. This was followed by the SA group, with a coronal shift of 0.37±1.11 mm. The IA group exhibited an apical shift of the mucosa of −0.7±1.15 mm, whereas the IAG group had the greatest apical shift, amounting to −1.1±0.96 mm. The intergroup differences were not significant (P=0.213) (Figure 4).
Figure 4
Mean clinical changes of the level of the buccal MM in relation to the healing abutment from pIP to sacrifice in all 4 treatment groups.
SA: alloplastic bone substitute material + standardized healing abutment, IA: alloplastic bone substitute material + individualized healing abutment, IAG: alloplastic bone substitute material + individualized healing abutment + a subepithelial connective tissue graft, MM: margo mucosae, pIP: post-implant placement.

Histomorphometric outcomes
All histomorphometric data were obtained at sacrifice and are displayed in Table 2. An illustrative image of the histological analysis is presented in Figure 5.
Table 2
Histological measurements in the different treatment groups
SA: alloplastic bone substitute material + standardized healing abutment, IA: alloplastic bone substitute material + individualized healing abutment, IAG: alloplastic bone substitute material + individualized healing abutment + a subepithelial connective tissue graft, MM-IS: height from the margo mucosae to the implant shoulder, MM-fBIC: height from the margo mucosae to the first bone-to-implant contact, MM-bBC: height from the margo mucosae to the buccal bone crest or the most coronal location of bone substitute particles on the buccal side, MM-lBC: height from the margo mucosae to the lingual bone crest, M-IS: thickness of the mucosa at the level of the implant shoulder, M-1IS: thickness of the mucosa at 1 mm below the implant shoulder, M-lBC: thickness of the mucosa at the level of the lingual bone crest.
Figure 5
Histological slide with vertical measurements.
MM: margo mucosae, IS: implant shoulder, BC lingual: bone crest lingual, fBIC: first bone-to-implant contact, D1: distance from MM to IS, D2: distance from MM to BC lingual, D3: distance from MM to fBIC.

The mean distance from the MM-bBC or the most coronal location of bone substitute particles (MM-bBC) was greatest in the SA group (4.2±0.58 mm), followed by the IAG (4.2±0.96 mm) and IA (4.0±0.37 mm) groups. The control group had the least distance (4.0±0.37 mm). The intergroup differences were not significant (P=0.787) (Figure 6).
Figure 6
Mean histological distance from the MM to the bBCor the most coronal location of bone substitute particles at sacrifice in all 4 treatment groups.
SA: alloplastic bone substitute material + standardized healing abutment, IA: alloplastic bone substitute material + individualized healing abutment, IAG: alloplastic bone substitute material + individualized healing abutment + a subepithelial connective tissue graft, MM: margo mucosae, bBC: buccal bone crest.

The mean distance from the margo mucosae to the implant shoulder (MM-IS) on the buccal side was greatest in the SA group (4.1±0.28 mm), followed by the control group (4.0±0.50 mm) and the IA group (2.6±0.04 mm). The IAG group had the least height (2.6±0.62 mm). The intergroup differences were statistically significant (P<0.001).
The mean distance from the margo mucosae to the first bone-to-implant contact (MM-fBIC) on the buccal side was greatest in the SA group (5.1±0.30mm), followed by the IAG (4.9±0.92 mm) and IA (4.3±0.79 mm) groups. The shortest distance was measured in the control group (4.1±0.67 mm). The intergroup differences were not significant (P=0.166).
Profilometric measurements
All profilometric data are shown in Table 3. The mean volume change from baseline (prior to tooth extraction) to post-implant placement was greatest in the IAG group, with a gain of 0.40±0.51 mm. The remaining groups demonstrated a decrease in volume of −0.03±0.26 mm (IA group), −0.21±0.22 mm (SA group) and −0.28±0.17 mm (control group). The intergroup differences were not significant (P=0.209).
Table 3
Profilometric measurements in the treatment groups

SA: alloplastic bone substitute material + standardized healing abutment, IA: alloplastic bone substitute material + individualized healing abutment, IAG: alloplastic bone substitute material + individualized healing abutment + a subepithelial connective tissue graft, volume change B-pIP: overall volume change from baseline (before tooth extraction) to post-implant placement at the buccal aspect of the implant sites, volume change pIP-S: overall volume change from post-implant placement to sacrifice at the buccal aspect of the implant sites, volume change B-S: overall volume change from baseline to sacrifice at the buccal aspect of the implant sites, thick MM B-S: thickness change at the level of the margo mucosae from baseline to sacrifice at the buccal aspect of the implant sites, thick 1MM B-S: thickness change at 1 mm below the margo mucosae from baseline to sacrifice at the buccal aspect of the implant sites, thick 3MM B-S: thickness change 3 mm below the margo mucosae from baseline to sacrifice at the buccal aspect of the implant sites.
A loss of volume from post-implant placement to sacrifice was found in all groups, and was greatest in the IAG group (−1.3±0.94 mm), followed by the SA (−0.76±0.62 mm), IA (−0.70±0.28 mm) and control (−0.65±0.46 mm) groups. The intergroup differences were not significant (P=0.089).
An overall loss of volume from baseline to sacrifice was found in all groups, with calculated mean values of −0.97±0.73 mm (SA), −0.93±0.44 mm (control), −0.88±0.45 mm (IAG), and −0.73±0.46 mm (IA). The intergroup differences were not significant (P=0.855) (Figure 7).
Figure 7
Mean volume change between baseline and sacrifice in all 4 treatment groups.
SA: alloplastic bone substitute material + standardized healing abutment, IA: alloplastic bone substitute material + individualized healing abutment, IAG: alloplastic bone substitute material + individualized healing abutment + a subepithelial connective tissue graft.
The mean horizontal change at the level of the margo mucosae from baseline to sacrifice was greatest in the IAG group, with a loss of −1.8±0.60 mm. This was followed by the control group, with a loss of −1.6±0.74 mm. The SA group had the least loss of thickness, with −1.0±1.68 mm, followed by the IA group, with −1.16±0.60 mm. The intergroup differences were not significant (P=0.516).
The mean horizontal change at 1 mm apical of the MM between baseline and sacrifice was higher in the control group, with a loss of −1.28±0.62mm, followed by the IAG group, with a loss of thickness of −1.26±0.53 mm. The least loss was observed in the IA group (−0.8±0.47 mm), followed by the SA group (−1.12±0.29 mm). The intergroup differences were not significant (P=0.446).
The mean horizontal change at 3 mm apical of the MM between baseline and sacrifice showed the highest loss in the control group (−0.86±0.48 mm), followed by the SA group (−0.33±0.57 mm). The IAG group had the least loss (−0.22±0.11 mm), followed by the IA group, with −0.26±0.31 mm of thickness loss. The intergroup differences were not significant (P=0.102).
DISCUSSION
The present study evaluated the effect of individualized healing abutments, the placement of a bone substitute material, and soft tissue grafting on clinical, volumetric, and histological outcome measures at immediate implant sites. The study demonstrated that: i) clinically, a coronal shift occurred in the buccal height of the mucosa in groups with a standardized healing abutment (control, SA), and a slight loss in mucosal height took place in groups with an individualized healing abutment with or without a soft tissue graft (IA, IAG); ii) histologically, a greater height of the mucosa was observed relative to the IS in the control and SA groups than in groups with an individualized healing abutment (IA, IAG), but a similar distance was found between the bone crest and the marginal mucosa in all groups; and iii) based on profilometric outcomes, the most favorable preservation of buccal volume occurred in the IA group.
The purpose of providing immediate provisionalization of implants is to shape the peri-implant soft tissues into an emergence profile that matches that of natural teeth [9] and to prevent future midfacial recession of the marginal mucosa [19]. De Bruyn [15] showed that both papillae and midfacial soft tissue levels remained fairly stable over time after immediate provisionalization. The emergence profile is developed by applying pressure to the submucosal tissue. If too much pressure is applied in provisional reconstructions, however, mucosal recession might occur due to excessive tension and decreasing vascularity of the peri-implant tissues. In the present study, the individualized healing abutments were slightly over-contoured. The clinical and histological analysis, therefore, revealed that the IA and IAG groups had more midfacial mucosal recession than the groups with a standardized healing abutment. This contradicts results from previous publications [151920]. One might speculate that in groups with a standardized healing abutment, more room was available for the soft tissue to grow, thereby leading to a coronal shift of the marginal mucosa.
The histological analysis confirmed the clinical data. The effect of adding an individualized healing abutment was detrimental to the crestal bone. This was shown by a longer distance between the implant shoulder and the fBIC in groups with an individualized healing abutment than in groups with a standardized healing abutment. Apart from the possible explanation of applying too much pressure, the surface roughness of the composite material could have affected the histological and clinical outcomes. Even though the composite material of the individualized healing abutments was polished, its surface was rougher and probably more plaque-retentive than a polished titanium standard abutment. Surface roughness can affect microbial aggregation [2122]. Bacteria could therefore have adhered and colonized the resin surface more easily, resulting in a more prominent inflammatory reaction that affected the quality of the attachment between the mucosa and the implant. Moreover, it is known that the abutment material can affect the location of the mucosal margin, the presence of inflammatory cells, and the location of the crestal bone. Based on preclinical studies, when some abutment materials are used on 2-piece dental implants, they can cause a stronger inflammatory reaction and therefore subsequent bone loss, clinically visible as an apical displacement of the mucosal margin [2324].
Synthetic bone substitute materials have been utilized for various clinical indications [25]. Different ratios of HA and TCP affect the resorption rate of the material. The bone graft used in this study consisted of coated biphasic calcium phosphate with 60% HA and 40% β-TCP, which has been used successfully for bone regeneration in animal models [2627] and in humans [2829]. The material shows a very low resorption rate, thereby providing a scaffold for volume preservation [3031].
In the present study, the addition of the bone substitute material provided volumetric tissue stability at the immediate implant sites. This conclusion was made based on profilometric measurements assessing the contour changes close to the mucosal margin and horizontal changes at different heights below the mucosal margin. The effect of the bone substitute material was limited to the profilometric and horizontal measurements. This can be explained by the fact that all other measurements (clinical and histological) primarily focused on the level of the soft tissues. At such a coronal level, bone substitute material does not have any effect. More apically, close to the IS, bone substitute is thought to minimize changes in the ridge following tooth extraction, with or without immediate implant placement. This was confirmed in the present study, with a more stable tissue contour at the level of the bone (as assessed by profilometric measurements).
The use of an SCTG did not improve mucosal height, and only provided an additional benefit in thickness gain at the most apical location (3 mm from the MM). These findings contradict previous publications reporting that soft tissue augmentation around implants with an SCTG positively influenced the stability of the facial peri-implant soft tissues [121314]. A possible explanation for why the IAG group had more midfacial mucosal recession may be linked to 2 factors: the apico-coronal position of the SCTG and the fact that a flap was raised. First, the grafts were positioned very apically in relation to the mucosal margin. This might be a reason why the effect of the soft tissue graft on thickness gain was only notable at the most apical location (3 mm from the MM). Moreover, a partial-thickness flap was performed to create a pouch for the SCTG. Such split incisions can cause mucosal dehiscence when the tissue is insufficiently thick due to disruption of the blood supply of the already fragile buccal bone [32]. This finding is in line with previous research showing that flapless implant placements resulted in less recession of the midfacial mucosa [333435].
One of the limitations of the study was the limited sample size, which could explain the lack of significant differences in the results. Secondly, the effect of an individualized healing abutment alone could not be properly investigated, since another experimental group with only an abutment was missing.
CONCLUSION
The group with a standardized healing abutment and no grafting procedures demonstrated the most favorable change (coronal shift) of the MM and the largest dimensions of peri-implant soft tissues. The addition of a bone substitute material and an individualized healing abutment, however, resulted in slightly better preservation of the peri-implant soft tissue contour.
 XML Download
XML Download