

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Intraoperative neural monitoring (IONM) is routinely used nowadays in thyroidectomies and parathyroidectomies, in order to identify and protect the anatomical and functional integrity of recurrent laryngeal nerve (RLN). The protocol of the proper use of IONM suggests the necessity of the stimulation of the vagus nerve as well, a procedure which is generally considered as a safe one in the general population (1). However, as the vagus nerve correlates with the heart rate, some concerns might be raised in certain heart diseases. As such case is considered the long QT syndrome (LQTS), which is a life threating arrhythmia caused by a disorder of myocardial electrical conduction (2). In the current study, we report the case of a 51-year-old female patient with a history of LQTS who underwent thyroidectomy and parathyroidectomy with the use of IONM. The Institution's Scientific Board approved this study (SB 001/2017) and the patient has signed the informed consent form.
CASE REPORT
The 51-year-old female patient referred to our department with ultrasound images of a large thyroid nodule, with a major diameter of 3.66 cm, which had excessive vascularity, occupied the left lobe and descended to the upper mediastinum. Additionally, the blood tests revealed high levels of calcium, low levels of phosphorus and parathormone levels in the normal range. Because of the patient's history of nephrocalcinosis, the presence of primary hyperparathyroidism with normal levels of parathyroid hormone could not be excluded. The additional ultrasound mapping by an experienced radiologist in parathyroid glands imaging, was negative for abnormal parathyroid tissue. Therefore, there was an absolute indication for surgery including, not only thyroidectomy but bilateral neck exploration to reveal parathyroid hyperplasia or adenoma, as well. The family history of the patient included LQTS, which affected 3 generations. The mutant was located at long QT syndrome type 1 (LQT1). The investigation of the family started from the late 90's when the nephew of the patient had several episodes of loss of consciousness. Both the patient and her sister mentioned similar events in the past. Moreover, there was a third sister who suddenly passed away at the age of 15 during swimming. The patient's children and her parents were asymptomatic. After a thorough family examination, the conclusion was that they had a mutant at LQT1, as mentioned above, and according to Schwartz criteria, 3 members had the clinical diagnosis of the syndrome, including our patient. More specific, the latter's electrocardiogram (ECG) revealed sinus rhythm and corrected QT=461 msec. All the family members were administered of b-blockers for life.
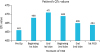
Because of the above history, there was a very thorough preoperative evaluation of the patient. All the potential intraoperative and postoperative risks were explained in detail to the patient, before she gave her signed informed consent form. The patient was led to the operative theater, while a special cardiologist was standing by and a defibrillator was ready for use. Since continuous intraoperative ECG recording was not available, the attending cardiologist performed manually ECGs at specific time intervals, according to surgeon's vagus nerve stimulation activity (Fig. 1). Moreover, ECG recording was performed at the induction to anesthesia and after patient's extubation, according to anesthesiologist's instructions. Patient underwent a total thyroidectomy and dissection of hyperplastic left upper parathyroid gland of a major diameter of 1.3 cm. Intraoperatively, after the mobilization of the left lobe, the vagus nerve was identified and stimulated with 1.5 mA, in order to exclude equipment failure or misplacement of the endotracheal tube, and to set an initial signal which would be used as a baseline. Afterwards, before its exposure, the RLN was localized by stimulating nearby and parallel to the trachea. Then, dissection and full exposure of the RLN by taking signals at all its revealed course followed. During the dissection, the vagus nerve was frequently stimulated, in order to exclude any proximal injury of the RLN. At the end of the lobectomy, the vagus nerve was stimulated as well as the RLN, and its signal remained similar to the initial one, which confirmed the anatomical and functional integrity of the RLN. An upper left hyperplastic parathyroid gland was also identified and was excised. The same procedure was followed during the right lobectomy. After thyroidectomy and parathyroidectomy completed and at the end of the hemostasis, laryngeal and vagus nerves were stimulated bilaterally, before the closure of the incision. Also, parathyroid hormone levels were measured intraoperatively 10 and 20 minutes after the excision of the abnormal gland, showing a decrease more than 50%, confirming the biochemical cure of the patient. Postoperatively, the patient was admitted to the intensive care unit and was put on monitoring for preventative reasons for 24 hours. Her postoperative course was uneventful and she was discharged after 48 hours.
DISCUSSION
LQTS is a life threating arrhythmia, which is caused by a disorder of myocardial electrical conduction, resulting in impaired ventricular repolarization (2). Its characteristics are prolongation of the QT interval on the ECG, recurrent episodes of syncope, cardiac arrest, pseudo-seizures and sudden death (23). It is a very dangerous syndrome, which acquires awareness, as the mortality rate among symptomatic patients left without therapy after the initial episode of syncope can reach 21% within the first year (4). Physical activity, or even emotional stress, can trigger the severe symptoms of LQTS. The syndrome is classified as congenital or acquired, usually triggered by drugs; however, there is evidence that patients with the latter type of the syndrome may have a silent mutation in one of the genes responsible for the inherited one. Regarding the congenital LQTS, there are many different types depending the genes where the mutations are, namely LQT1, LQT2, LQT3, LQT4, LQT5, LQT6, and LQT7 (5). LQT1, which the patient of our case had, is provoked by a mutation at KCNQ1 gene, which encodes the a-subunit of the K+ channel Kv7.1, generating the ion channel Iks. When the latter is defective, the QT interval is not shortened during tachycardia, resulting in severe arrhythmia (3).
Surgical patients with LQTS need extra attention preoperatively and during their hospitalization. Before the operation, they ought to be carefully examined and evaluated by a cardiologist and an anesthesiologist. An ECG at rest is needed, in order to estimate the QT prolongation. Treatment with b-blockers should be continued until the day of the operation. All the other medication that the patients receive ought to be checked, in order to avoid drugs that may trigger QT prolongation (6). Furthermore, preoperatively they should be maintained in a quiet and calm environment to prevent stress, which may stimulate the sympathetic system. Additionally, sufficient anxiolytics should be administered for the same reason. Also, a defibrillator should be nearby for an urgent use (7). At the induction to the general anesthesia, certain drugs should be used, such as propofol, isoflurane and vecuronium, but equally important is that the patient is adequately anaesthetized before intubation, for the avoidance of triggering the sympathetic system (67).
Intraoperatively, in the current bibliography, there are not any specific measures mentioned that should be taken regarding patients with LQTS. Nevertheless, in thyroidectomy, many questions may be raised concerning the use of IONM. Over the past two decades, IONM has become a useful tool for surgeons in order to identify the RLN and to predict the postoperative function of the vocal cords (8), hence it is routinely used especially in high-risk operations. Currently, vagus nerve stimulation before and after thyroid lobectomy is recommended, according to the guidelines which are published by an international group of experts (1). In case of RNL section, the nerve might be stimulated distally of the lesion, leading to false underestimation of the damage (9). During vagus stimulation, RLN is stimulated indirectly and is completely evaluated in its all course. Therefore, vagus nerve stimulation is considered more accurate for the prediction of RLN palsy (1011). Continuous vagus IONM is also used nowadays, providing real-time evaluation of RLN.
Even though the use of IONM is generally considered as a safe procedure, including the continuous one (12), cases of cardiac arrest have been recently reported (13).
There is not any data regarding patients with certain heart diseases such as LQTS since vagus enervates heart as well. More specifically, vagus is a mixed nerve that contains 20% efferent and 80% afferent fibers. It descends to the chest and enervates the heart with parasympathetic fibers (14). It is evident that its role is crucial in the heart rhythm. Even though the symptoms of LQTS are provoked by the stimulation of the sympathetic system, concerns may be raised by the possibility of the stimulation of parasympathetic system when IONM is used, especially at the right vagus nerve, which primarily innervates the pacemaker of the heart, the sinoatrial node. With IONM, electrical current is delivered to the nerve via a probe, stimulating the vocal cords, while EMG responses are measured (15). Nowadays, devices that produce electrical current have been developed and are implanted to humans, especially at the right vagus nerve, in order to treat heart failure (16), showing that the stimulation of the vagus can potentially affect the cardiac rhythm.
In conclusion, the experience of the use of IONM during thyroidectomy and parathyroidectomy is immense nowadays. Even though it is considered as a safe procedure, some side effects are mentioned. At the patient of our case, there were some concerns about the safety of stimulation of the vagus nerve, which is a needed step during IONM. Nevertheless, the proper use of IONM, including vagal nerve stimulation, seems to be a safe procedure without complications in patients with LQTS.
 XML Download
XML Download