

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Parathyroid cancer (PC) is an exceptionally rare malignancy. It constitutes only 0.005% of all malignancies and 1%–5% of cases of primary hyperparathyroidism (1). In Korea, 21 cases of PC (7 male and 14 female patients) were found among 214,701 malignancies treated in 2015 (2).
The clinical presentation of PC is hypercalcemia accompanied with a high serum level of parathyroid hormone, which is like that of benign primary hyperparathyroidism. Both diseases can present with nephrolithiasis, osteopenia, or general weakness. The definitive diagnosis of PC is made by pathologic examination for lesions displaying vascular invasion, perineural space invasion, capsular penetration with growth into adjacent tissues, and/or metastasis. Therefore, preoperative fine needle aspiration cytology is not suitable for differentiating between benign and malignant tumors (3), and thus, it is nearly impossible to diagnose PC preoperatively. For that reason, most patients undergo operation under the presumption of parathyroid adenoma and suspicion of PC is only raised during surgery.
Likewise, differentiating PC from benign primary hyperparathyroidism intraoperatively is also challenging. PCs are firm, densely scarred, obliterate normal tissue planes and often adhere to the thyroid glands. Although atypical adenomas may similarly be large and exhibit considerable adherence to surrounding structures, they do not direct invade surrounding tissues such as in cases of malignancies (1).
The treatment of choice for PC is complete surgical resection — en bloc resection including the tumor along and any involved adjacent structure (45). Resection of the ipsilateral thyroid gland and the central compartment lymph node is important for disease-free survival (67).
Because it is difficult to determine whether a parathyroid lesion is malignant or not, many surgeons are perplexed with a postoperative pathologic confirmation of PC. Therefore, we analyzed the clinicopathologic characteristics of the patients of PC to identify diagnostically useful differences between PC and benign primary hyperparathyroidism.
MATERIALS AND METHODS
A total of 157 parathyroid operations were performed at our institute between 2001 and 2017, and 83 of these were conducted in primary hyperparathyroidism patients (the other 74 were 65 secondary hyperparathyroidism and 9 parathyroid cysts). These 83 patients were diagnosed as having primary hyperparathyroidism. In addition, 2 patients with secondary hyperparathyroidism diagnosed postoperatively to have PC were also enrolled in the study.
Medical records were reviewed retrospectively for clinical information including age, sex, symptoms, physical findings, major cause of hyperparathyroidism diagnosis, and preoperative biochemical test results. Symptoms or signs including nephrolithiasis, palpable neck mass, osteopenia/osteoporosis, and more were reviewed. Biochemical tests included serum calcium, phosphorus, alkaline phosphatase (ALP), and intact parathyroid hormone (iPTH). Preoperative imaging studies, operative records, and pathologic results were also analyzed. Preoperative imaging study included neck ultrasonography (USG) and a 99mTc-myocardial perfusion (MIBI) parathyroid scan, and if needed, neck computed tomography (CT) or magnetic resonance imaging (MRI). Medical records of USG findings were evaluated when images were unavailable. Operative records were searched for mention of parathyroid tumor adhesion to surrounding thyroid/soft tissue.
PC was diagnosed pathologically based on the presence of vascular invasion, perineural space invasion, capsular invasion with growth into adjacent tissue, and/or metastasis, in accordance to the criteria detailed in the fourth edition of the World Health Organization classification of endocrine tumors (3). Vascular invasion was described as tumor cells invading through vessel walls and endothelium and/or thrombus adherent to an intravascular tumor. Extra-parathyroidal invasion was defined as having features of cancer extending into surrounding structures, including extension into soft tissue, muscle and/or thyroid. Mitotic counts per 50 high power fields (HPFs) were evaluated by microscopy of tumor sections.
During follow-up, serum calcium, phosphorus, and iPTH were examined every 3 months. When hypercalcemia (>10.8 mg/dL) and elevated iPTH (>65 pg/mL) were confirmed biochemically, neck USG, 99mTc-MIBI parathyroid scan, neck CT or MRI, chest CT, and positron emission tomography (PET)-CT were conducted to locate and evaluate distant metastasis. Disease recurrence and survival were evaluated in the PC patients. Persistent PC was defined as biochemically confirmed hypercalcemia (>10.8 mg/dL) within 6 months of initial surgical intervention, and recurrent PC was defined as normocalcemia persisting longer than 6 months after initial surgery by eventually followed by recurring hypercalcemia.
Our Institutional Review Board of Gil Medical Center approved this retrospective study before the patient list was retrieved from the hospital database (GCIRB 2017-379).
1. Statistical analysis
Statistical analysis was performed using IBM SPSS version 23.0 (SPSS Inc., Chicago, IL, USA). Pearson's χ2 test and independent t-test were used to evaluate the significances of differences between PC and benign primary hyperparathyroidism. Fisher's exact test, McNemar's test and the Mann-Whitney U test were used for nonparametric analysis. Statistical significance was accepted for P values <0.05.
RESULTS
The clinicopathologic characteristics of the 85 study subjects are summarized in Table 1. Eighty-three patients were diagnosed as primary hyperparathyroidism and 2 patients were initially diagnosed as secondary hyperparathyroidism but were revealed as PC after operation. PC was diagnosed in 7 patients (8.2%). Incidence of PC among primary hyperparathyroidism in our institution was 6.02% (5/83). Follow-up duration was 52.9±44.4 months (range: 0–154).
Table 1
Clinicopathologic characteristics of 85 hyperparathyroidism patients

Symptoms and signs accompanying hyperparathyroidism varied in 85 patients. The mean number of symptoms and signs was 2.9±1.7 (range: 1–11). Osteopenia/osteoporosis was present in 54 patients (63.5%), hypertension in 26 (30.6%), nephrolithiasis in 21 (24.7%), general weakness/fatigue in 13 (15.3%), gall bladder stone in 8 (9.4%), weight loss, abdominal pain, and vomiting in 6 each (7.1%), bone pain, nausea, and polydipsia/polyuria in 5 each (5.9%), anorexia, palpable neck mass, neck discomfort, and headache in 4 each (4.7%), tingling sensation, dizziness, and depression in 3 each (3.5%), hypoglycemia, chest pain, lethargy, and syncope in 2 each (2.6%), and bone fracture, and recurrent pancreatitis in one each (1.2%) were noted. Incidental hypercalcemia was observed in 20 patients (23.5%), incidental neck mass by USG in 16 (18.8%), incidental findings during thyroid surgery in 11 (12.9%), and incidental ALP elevation was found in one (1.2%). The most common chief complaint to make patient to be treated was an incidental finding of hypercalcemia (18/85, 21.2%), and the second was incidental finding of neck mass by USG (15/85, 17.6%).
Differences between PC and benign primary hyperparathyroidism are summarized in Table 2. Tumors were larger in cancer patients than in patients with benign disease (P=0.002). Preoperative serum iPTH (P=0.002) and ALP (P=0.01) were higher, and adhesion to surrounding soft tissue or the thyroid gland (P<0.001) (Fig. 1) was observed more frequently in cancer patients compared to the benign counterpart. No study subject showed calcification in USG. Tumors of one cancer patients (14.3%, case 1; Table 3) and two parathyroid adenoma patient (2.6%) infiltrated thyroid tissue (P=0.230) in USG. In these 3 patients, adhesion to thyroid was recognized during surgery. One (14.3%) PC and three (3.8%) benign disease cases presented with a palpable neck mass (P=0.296). Nephrolithiasis was present in 1 (14.3%) cancer and 21 (26.9%) benign cases (P=0.671), while osteopenia/osteoporosis was observed in 4 (57.1%) in cancer and 52 (66.7%) benign patients (P=0.686).
Table 2
Differences between parathyroid cancer and benign primary hyperparathyroidism

Values are presented as mean±standard deviation or number (%). Normal range: Calcium, 8.2–10.8 mg/dL; Phosphorus, 2.5–4.7 mg/dL; iPTH, 10–65 pg/mL; ALP, 35–123 U/L; Creatinine: 0.6–1.2 mg/dL.
iPTH = intact parathyroid hormone; ALP = alkaline phosphatase.
*Analysis excluding patients under hemodialysis.
Fig. 1
Left lower parathyroid gland was adherent to lower pole of left thyroid gland (thick arrow) and surrounding soft tissue (thin arrow) (case 6).

Table 3
Seven cases of parathyroid cancer
According to histopathologic results, the cut surface margin of the PC had an infiltrative margin (Fig. 2). All PCs exhibited capsular invasion, 6 (85.7%) exhibited vascular invasion, and 6 (85.7%) exhibited capsular penetration with growth into adjacent tissues (Fig. 3). The mean number of capsular invasion foci was 4.1±3.3 (range: 1–11) and the mean number of vascular invasion foci was 1.6±0.8 (range: 0–2). Three patients had thyroid parenchyma invasion pathologically (cases 2, 5, and 6). Mean mitotic count (1.0±1.8 vs. 0.8±4.3, P=0.046) were significantly higher in PC than in benign cases.
Fig. 2
The parathyroid cancer shows whitish firm fibrotic cut surface with infiltrative margin (case 6).
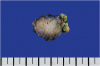
Fig. 3
The parathyroid cancer has a thick fibrous tumor capsule and the peritumoral soft tissue invasion is extensive (astrix) (case 6). (hematoxylin and eosin, ×12).

Tumor adhesion to surrounding soft tissue or the thyroid gland was observed in 10 (12.8%) of the 78 benign cases, among which all were parathyroid adenomas. Their tumor size was larger (3.20±0.95 cm vs. 1.94±0.69 cm, P<0.001), and their serum calcium (14.0±3.5 mg/dL vs. 11.8±1.6 mg/dL, P=0.009) and iPTH (1,291.6±713.7 pg/mL vs. 367.5±394.7 pg/mL, P<0.001) levels were higher than the non-adherent cases in 78 benign patients. Furthermore, their serum ALP level (309.3±255.7 U/L vs. 145.7±159.5 U/L, P<0.001) and mean mitotic count (4.90±11.56 vs. 0.15±0.68, P=0.003) were significantly higher.
Details of the 7 cases are provided in Table 3. We had begun operation with suspicion of parathyroid adenoma in most patients. When the adhesion to the thyroid gland or surrounding soft tissue was detected intraoperatively, however, en bloc resection including the ipsilateral thyroid lobe and central lymphadenectomy was performed under suspicion of PC. Three patients had obvious symptom to make them to be treated (42.9%, cases 4–6). One patient (case 7) were diagnosed as PC after having medical check-up. Case 1 of female patient was diagnosed as PC after thyroid operation for papillary thyroid cancer. There was no symptom and sign related to hyperparathyroidism. Her preoperative thyroid USG showed a heterogeneous solid nodule with an unclear border at the posterior side of the thyroid. It looked to be a thyroid mass unrelated to thyroid cancer. However, the mass was adhesive to the right thyroid, which led to en bloc resection with total thyroidectomy. Cases 2 and 3 patients in their forties had been under hemodialysis for 15 and 14 years respectively, during which secondary hyperparathyroidism occurred. Osteoporosis was detected in these patients. Preoperative neck USG in case 2 revealed a 1.0 cm sized, smooth, oval, hypoechoic nodule in the posterior portion of the right mid pole, and 0.9 cm and 0.7 cm lesions at left gland with similar characteristics. Intraoperatively, the left lower parathyroid gland resembled a 2 cm sized kidney-shaped mass. Despite conducting central neck dissection to identify remaining parathyroid tissue, the right lower parathyroid gland could not be found. Pathology report revealed the left lower gland to be a PC. In case 3, preoperative neck USG displayed a 2.0 cm sized hypoechoic lesion in the upper area of the left thyroid lobe suggestive of a parathyroid tumor. As the adhesion to the left thyroid was noted intraoperatively, en bloc resection was performed with excision of right upper and left lower parathyroid glands. Despite through central neck dissection, we could not find the right lower parathyroid gland. The left upper parathyroid gland was diagnosed to contain PC postoperatively. These patients were alive with a low-normal calcium level and mild iPTH elevation at 18 and 11 months after operation, respectively. Case 4 patient had suffered from fatigue and bone pain. Gall bladder stone and osteoporosis were discovered during evaluation. She showed serum iPTH elevation with a normal calcium level after the operation, a whole body 99mTc-MIBI scan and PET-CT were performed. Pelvic MRI depicted multiple brown tumors, which were later pathologically confirmed. Serum iPTH was normalized after neck radiotherapy (30 fractions at 5,400 cGy). Case 5 patient visited with palpable neck mass and neck discomfort accompanied with weight loss and nephrolithiasis. Case 6 patient complained poor oral intake, weight loss, fatigue, and tingling sense. She showed gall bladder stone and osteoporosis. Case 4–7 patients underwent en bloc resection with the ipsilateral lobe and central lymph node under suspicion of PC due to detection of adherence to surrounding soft tissue and thyroid gland.
There was no persistent PC in 7 patients. However, two patients (Cases 5 and 6) suffered from disease recurrence. Case 5 patient was followed-up irregularly and experienced recurrence three times; in operative bed soft tissue at 27 months postoperatively, in the operative bed and mediastinum at 39 months, and in mediastinum at 54 months. Serum iPTH and calcium levels were normal after reoperations. At 77 months, hypercalcemia was aggravated, and lung metastasis was detected on CT. However, he did not visit out-patient clinic regularly and bone metastasis was detected at 131 months, and he died of hypercalcemia associated cardiac arrest at 139 months postoperatively. In case 6 patient, local recurrences occurred in operative bed soft tissue at 15 and 20 months postoperatively.
DISCUSSION
In this study, we analyzed the characteristics of PC patients and evaluated differences between PC and benign primary hyperparathyroidism. Tumor size was larger, and preoperative serum iPTH and ALP were significantly higher in cancer patients than in those with benign disease. Intraoperative findings of the severe adhesion between parathyroid lesion and surrounding thyroid gland or soft tissue were observed in cancer patients.
Several clinical, laboratory, and radiologic findings raised suspicion of PC. In general, PC was more common in younger patients and in men. Average age at presentation was 48 for cancer and 55 for those with benign disease. In cancer patients, the male/female ratio was around 1:1 but 3–4 times more women than men had benign disease (8). In a report conducted in Korea in 2015, 7 males and 14 females of PC patients were found and the disease was most common in the sixth decade of life regardless of sex (42.9%) (2).
In previous reports, severe hypercalcemia (>14 mg/dL), iPTH elevation to 3–15 times the normal upper limit, serious renal and skeletal disease, and the presence of a palpable neck mass were found to be features of PC (4910). Furthermore, some patients with PC exhibit ALP elevation than in those with primary hyperparathyroidism, in whom levels were generally near the upper limit of normal (411). Ultrasonographic evidence of infiltration, calcification, suspicious vascularity, and the presence of a thick capsule have also been reported to be strongly associated with parathyroid malignancy (412).
Intraoperative suspicion of local invasion or regional metastasis was critical (912), and findings of a lobulated firm mass, surrounded by a fibrous grayish-white capsule that adheres persistently to the ipsilateral thyroid lobe or adjacent cervical tissues raised suspicion of PC.
In the present study, no difference was detected between the gender ratios or ages between the malignant and benign patient groups at diagnosis. The presence of a palpable neck mass at presentation and co-existing renal or skeletal disease were no different between the two groups. Preoperative imaging studies revealed no calcification in any malignant lesions, though one patient showed infiltration into the thyroid lobe. Analyzing preoperative USG was difficult because ultrasonographic images were not available in some cases due to the retrospective nature of the study. In these cases, we evaluated medical records of USG findings, but these were inadequate for evaluating the presence of infiltration, calcification, suspicious vascularity, or a thick capsule.
Interestingly, two patients with a diagnosis of secondary hyperparathyroidism were found to have PC. The etiology of PC has not been determined, and no established predisposing factors have been identified. However, several etiologic factors are associated with PC including history of neck radiation, a hyperplastic parathyroid gland, and secondary/tertiary hyperparathyroidism caused by chronic kidney disease (despite no evidence that PC arises from malignant transformation of preexisting parathyroid lesions) (411). Several case reports have described PC occurring in secondary/tertiary hyperparathyroidism (1314151617). Our seven cases of PC did not have history of neck radiation.
Mitotic status does not distinguish PC from adenomas (318). Mitosis can be observed in 80% of parathyroid adenomas (usually at <1 per 10 HPFs), and also 80% of PC (19). However, it has been reported that mitoses of >5 per 50 HPFs in PC is a poor prognostic factor (18). Although the atypical mitotic figure is exclusively observed in PC, it was not observed in our series. Although the number of mitosis was not big, in this study, mitotic count was higher in PC patients than benign cases significantly. We did find that a high mitotic index was associated with adhesion to surrounding tissue in benign group. We suggest it is worth considering the possibility that parathyroid adenoma with severe adhesion is an atypical parathyroid adenoma entity. Atypical parathyroid adenoma is a controversial entity, which displays various atypical features (adhesion to surrounding tissues, banding fibrosis, nuclear atypia, and mitosis) without meeting the diagnostic criteria of PC (3). It is difficult to differentiate atypical parathyroid adenoma and PC in the operative field due to the adhesive feature (20). However, most atypical parathyroid adenomas are clinically benign (21), and no genetic or pathological link has been demonstrated between parathyroid adenoma, atypical parathyroid adenoma and PC (2223).
Several reports have been published on the detection of synchronous thyroid cancer and PC (242526). Some suggest coincidence, while others have proposed association based on their similarities, which include increased endogenous calcium levels, growth factors, and goitrogenic factors (24). In our series, 17 patients (20%) received combined thyroid surgery because of concomitant thyroid disease (14 thyroid cancer and 3 benign disease). Because we did not routinely evaluate preoperative iPTH for thyroid operations, the true incidence of concomitant thyroid and parathyroid lesions from our institution could not be calculated.
The incidence of PC among primary hyperparathyroidism in our institution was 6.02% (5/83), although in the literature it is reported to be around 1%–5% (1). A reason for this inconsistency is the low annual incidence of primary hyperparathyroidism in Korea (0.007%–0.014%) (27) compared to annual incidence from western countries ranging from 0.04% to 0.3% (282930).
As this series was conducted using a retrospective design, it was limited in terms of incomplete preoperative USG data and follow-up loss. Although we searched medical records meticulously, accompanying symptoms, signs, and diseases would have been analyzed more thoroughly had this been a prospective study.
In conclusion, PC patients had larger tumors and higher preoperative serum iPTH and ALP values. The intraoperative detection of adhesion to surrounding thyroid gland or soft tissue was found to be essential for raising suspicions of PC. Notably, PC also developed from secondary hyperparathyroidism patients and found on occasion to be accompanied by thyroid cancer. Surgeons who explore patients with hyperparathyroidism or perform thyroid surgery should be prepared to undertake initial, appropriate en bloc resection upon suspicion of potential PC.
 XML Download
XML Download