

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Kyungjoong Kim, Myungkwan Ko, Ho Chan Sim, Chang Lae Kim, Yeo Jin Jung, Tae Oh Kim
Abstract
Intussusception is a common in pediatric age group. But it is rare in adults. And intussusception caused by tumor account for 1% of bowel obstructions in adult. Intussusception is an extremely rare cause of abdominal pain in pregnancy. In particular, cases of Intussusception due to colorectal cancer during pregnancy have never been reported in Korea. Our patient is a 34 years old woman who presented at 14 weeks of her second pregnancy. She presented with right lower abdominal discomfort and intermittent palpable mass which was usually spontaneously resolved. In the MRI study, pathologic asymmetric wall thickening was still noted and ileocolic intussusception was noted, and in colonoscopy, there was ulcerofungating mass around ileocecal valve which may be a leading point of intussusception. Biopsy was done. Pathologic finding was poorly differentiated adenocarcinoma. Under the patient agreement, we performed dilatation and curettage and laparoscopic right hemicolectomy and lymph node dissection. Now she is receiving a FOLFOX chemotherapy.
Figures and Tables
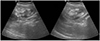
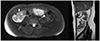
 | Fig. 2Diffuse wall edema on the ascending colon, but no definite intussusception or mass like lesion were noted. Ileocecal valve (arrow).
|
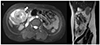
 | Fig. 3Pathologic asymmetric colon wall thickening (arrow) was observed but there was no definite intussusception in the first magnetic resonance imaging.
|

References
1. Sreenivas KS, Vinayachandran S. Intussusception in pregnancy: a rare case report. IJSS. 2014; 1:8–9.
2. Tan KY, Tan SM, Tan AG, Chen CY, Chng HC, Hoe MN. Adult intussusception: experience in Singapore. ANZ J Surg. 2003; 73:1044–1047.

3. Gurbulak B, Kabul E, Dural C, et al. Heterotopic pancreas as a leading point for small-bowel intussusception in a pregnant woman. JOP. 2007; 8:584–587.
4. Grzelak K, Bil M, Czerwińska M, Cencelewicz-Lesikow A, Bieniasz M. Colorectal cancer during pregnancy – case report and brief review of the literature. MEDtube Sci. 2017; (1):16–20.
5. Osime OC, Onakewhor J, Irowa OO. Intussusception in pregnancy--a rarely considered diagnosis. Afr J Reprod Health. 2010; 14:145–148.
6. Perdue PW, Johnson HW Jr, Stafford PW. Intestinal obstruction complicating pregnancy. Am J Surg. 1992; 164:384–388.
7. Özyapi AG, Kars B, Ergen B, et al. Primary jejunal intussusception in pregnancy: a rare case report. J Turkish-German Gynecol Assoc. 2009; 10:120–121.
8. Kang HJ, Kim SH, Ryu JH, Choi SJ, Roh CR. A case of intussusception managed conservatively in pregnancy. J Womens Med. 2011; 4:15–18.
9. Mahungu P, Galerneau F, Pugash D, Williams K. Intussusception during pregnancy: a case report and review of the literature. J SOGC. 1996; 18:77–80.
10. Long SS, Long C, Lai H, Macura KJ. Imaging strategies for right lower quadrant pain in pregnancy. AJR Am J Roentgenol. 2011; 196:4–12.
11. Gould CH, Maybee GJ, Leininger B, Winter WE 3rd. Primary intussusception in pregnancy: a case report. J Reprod Med. 2008; 53:703–707.
12. American College of Obstetricians and Gynecologists' Committee on Obstetric Practice. Committee opinion no. 656: guidelines for diagnostic imaging during pregnancy and lactation. Obstet Gynecol. 2016; 127:e75–e80.
 XML Download
XML Download