

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Antegrade dissection and re-entry (ADR) refers to an attempt to cross a coronary chronic total occlusion (CTO) lesion that leads to wire and/or equipment passage in the sub-intimal space (SIS) followed by re-entry to the distal true lumen. The re-entry point can occur at different sites and is dependant on the specific ADR technique that is employed. In reality, many wire-based CTO percutaneous coronary intervention (PCI) approaches lead to sub-intimal wire passage, particularly as the lesions become longer and more complex.1)2)3) Whilst blunt dissection is not employed as part of this wire based recanalization, the end result is of a deployed stent that passes from the proximal true lumen, via a segment in the SIS to the distal true lumen. This is often an unrecognized occurrence, especially if intravascular ultrasound (IVUS) or optical coherence tomography is not performed prior to stent deployment, but is not known to be associated with adverse outcomes.
ADR as a dedicated technique was initially adapted from peripheral intervention and was first described in the coronaries as the sub-intimal tracking and re-entry (STAR) technique.4) This involved pushing a looped or ‘knuckled’ guidewire (usually polymer jacketed) from within the CTO body until it re-entered the distal true lumen. The technique was adapted to involve the use of intra-lesion contrast injection5) as well as for bail-out when some of the CTO lesion was wired as an initial strategy (mini-STAR).6) However, this approach was associated with uncontrolled re-entry that was typically distal, often at a bifurcation and that could lead to run-off into 1 terminal branch. Unsurprisingly, the long-term results were poor with high rates of repeat revascularization and target vessel occlusion.7)8)9) Today, STAR or mini-STAR do still represent a small proportion of successful ADR cases, being accepted as an inadvertently successful technique when knuckle wires re-enter the vessel at or close to the distal cap.
Further adaptations of practice occurred over time as it was realized that STAR and its variations were sub-optimal approaches. One early evolution without dedicated equipment was limited antegrade sub-intimal tracking (LAST). This approach involved an initial wire-based approach to cross the CTO lesion. Once it was recognized that the wire was in a sub-intimal position, the guidewire was swapped out via a micro-catheter and a tapered tip, high penetration force guidewire was shaped with significantly angled primary and secondary bends in an effort to puncture back into the true lumen. However, re-entry was relatively unreliable, also unpredictable in terms of its location relative to the distal cap and this technique was also associated with less favorable outcomes.10) LAST as a concept may still be applied in some geographies where dedicated ADR devices are either unavailable or prohibitively expensive. The use of standard dual lumen catheters is also sometimes applied to try to assist re-entry. However, the overall reliability of this technique and systematic examination of outcomes are poorly understood.
The CrossBoss and Stingray system (Figure 1; Boston Scientific, Marlborough, MA, USA) have been developed as a combination of devices that can create a controlled antegrade dissection plane to facilitate targeted distal vessel re-entry.11) The CrossBoss catheter is a blunt dissection tool with a 1 mm rounded tip that will either track through intimal plaque and re-enter the distal true lumen itself (<10% of cases) or alternatively create a controlled dissection plane in the SIS that allows the Stingray balloon to be delivered just beyond the distal cap of the occlusion. This allows a focused puncture back into the vital vessel at a precisely controlled site and thus revascularization of all the distal branches. Application of this technique promotes reproducibility as well as predictability of the re-entry site. In many geographies this has become the dominant mode of ADR in contemporary practice.

Newer technologies are in development with adaptations of re-entry devices from dual lumen catheters. One such device in early clinical development is the Recross (IMDS, Drenthe, Netherlands), although others are also approaching clinical use. Where these devices will fit in future clinical practice of ADR remains to be seen.
A FOCUS ON UPDATED TECHNICAL APPROACHES USING THE CROSSBOSS/STINGRAY SYSTEM
Algorithmic approaches to CTO lesions have been recommended for several years.12)13) Whilst many lesions are amenable to multiple strategies, the most complex CTOs will often require an ADR or retrograde dissection and re-entry (RDR) based approach. Nevertheless, the majority of lesions that are attempted in global practice usually begin with an antegrade wire (AW) approach. It is not uncommon, especially in increasingly long lesions for the wire to pass beyond the distal cap of the CTO in the SIS. On occasion this can be resolved by redirection of the wire within the CTO body. Some would also advocate parallel wiring to try to resolve this issue. Nevertheless, it is not uncommon for the distal true lumen to be inaccessible. Under these circumstances, we would advocate consideration of an early switch to a controlled ADR technique, provided that there is no major distal side-branch at the landing zone. One evolution from historical practice when ADR is performed as a bail out for unsuccessful AW is that blunt dissection with knuckle wires or a CrossBoss device is often unnecessary.
Consider the example shown in Figure 2. There is a moderate length lesion in a dominant right coronary artery. AW approaches are unsuccessful with both a low penetration force polymer jacketed wire (Fighter; Boston Scientific) and medium gram force wire (Pilot 200; Abbott Vascular, Santa Clara, USA). Once the Pilot 200 has progressed beyond the distal cap into the SIS, there is an immediate switch to an ADR approach. A CrossBoss device is not required. Rather, the coil-based micro catheter that is already in situ in the CTO is used to create a space to facilitate Stingray delivery. This minimizes the time and maneuvers that are required to progress the case to the point of puncture and re-entry. The end result is minimal hematoma formation, preservation of the landing zone and successful re-entry in a time efficient manner. All distal branches are preserved and costs have been reduced as a CrossBoss device was not required.
 | Figure 2Example of ADR as a bailout for sub-intimal wire passage in contemporary practice. (A) There is a 25–30mm CTO of the mid RCA. (B) A Pilot 200 advances into the CTO and beyond the distal cap but is in a subintimal position. (C) Blunt dissection is not required, rather the micro-catheter is advanced to the landing zone to facilitate delivery of the Stingray. (D) The Stingray is exchanged into the vessel, inflated and orientated with the target vessel on the left of the balloon. (E) Final result after successful re-entry and vessel reconstruction.ADR = antegrade dissection and re-entry; CTO = coronary chronic total occlusion; RCA = right coronary artery; RV = right ventricular; SIS = sub-intimal space.
|
Primary ADR is classically applied in the setting of defined proximal cap anatomy (by angiography or IVUS), where the CTO segment is long (and/or ambiguous) and when there is a landing zone that is proximal to a distal bifurcation at significant branches (Figure 3). Once again, practice has evolved over time. The miniaturization of equipment and in particular the advent of the Stingray LP and dedicated trapping balloons have obviated the need for the use of 8F guiding catheters. In our practice, where Caucasian patients often have larger caliber radial arteries, 7F access has become preferred for CTO PCI. This usually leads to a transradial approach. However, this may not be feasible in all geographies or patient groups. A standard step-by-step approach to a more complex lesion with primary ADR is outlined in Figures 3, 4, 5. Typically, the proximal cap is crossed. A balloon is used to introduce a guide catheter extension (most often Trapliner; Teleflex, Wayne, PA, USA). This aims to prevent any inflow of blood from the systemic circulation into the CTO segment and thus the SIS with an ultimate goal of minimizing any distal hematoma (Figure 4). The preservation of the landing zone aids the efficacy of re-entry, whilst the use of the Trapliner (if available) will facilitate efficient device exchanges. Many operators will then site a micro-catheter in the CTO segment and advance a knuckled guidewire over a proportion of the lesion. Whilst more disruptive than using a CrossBoss, this will usually lead to rapid progress, avoidance of side branches and potentially lead to safer crossing of tortuous or ambiguous segments. When the main vessel architecture is reached, the CrossBoss is used by many operators at this stage to create a smaller, less disruptive and more controlled dissection plane for the distal 2–3cm of the lesion at the landing zone. Once again, this step will help to minimize hematoma formation and enhance the efficacy of the re-entry step.
 | Figure 3Ideal anatomy for a primary ADR procedure using the CrossBoss and Stingray systemADR = antegrade dissection and re-entry; CTO = coronary chronic total occlusion; PDA = posterior descending artery; PLV = posterolateral vessel.
|
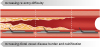
 | Figure 4Development of intramural hematoma and compression of the distal landing zone if the sub-intimal space is exposed to systemic blood flow.
|
 | Figure 5Treatment of the lesion depicted in Figure 3. (A) A resistant proximal cap is crossed with a combination of a Confienza Pro 12 (Asahi Intecc) and Turnpike Gold (Teleflex). (B) The stiff wire is removed and swapped out for a low penetration force, polymer-jacketed knuckle wire. (C) The proximal cap is dilated with a 2.5mm balloon to facilitate the introduction of a Trapliner (Teleflex). (D) A CrossBoss is then used to complete a controlled dissection to the landing zone. (E) The Trapliner facilitates efficient delivery of a Stingray balloon to allow controlled re-entry to occur. (F) Final result after stent deployment and optimization.
|
After the Stingray has been successfully delivered we would recommend routinely attaching a Luer lock syringe to the central port proximally and aspirate with a large syringe on vacuum for a period of a few minutes. After inflating the Stingray balloon and finding the correct orientation for re-entry on X-ray, the puncture is performed (Figure 6). This represents another area of evolving practice. The Stingray wire is a dedicated device that has a small micro-barb at the distal tip (Figure 1). The concept behind this design was that this would ‘catch’ the intimal tissue and facilitate re-entry. Whilst this is often true where there is a closely approximated balloon to a healthy distal landing zone, this aspect of wire design can be unhelpful where there is a large burden of atheroma (often calcific) between the balloon and the lumen (Figure 7). Many operators now prefer a high penetration force, tapered tip wire to attempt re-entry (e.g. Confienza Pro 12 or Astato 8/20; Asahi Intecc, Seto, Japan or Hornet 14; Boston Scientific) under these circumstances.

 | Figure 7Examples of different disease burdens at the landing zone. The most rightward example is often amenable to re-entry with the Stingray wire, whereas many experienced operators are now using high penetration force wires for the scenario on the left.
|
Once re-entry has been successfully achieved, the same principles apply as initially described with the ADR technique. A micro-catheter should be used to exchange the stiff re-entry wire for a safer workhorse wire. This minimizes the risk of distal wire exit, distal vessel dissection and will allow a safer completion of the procedure. With a guide catheter extension already in situ, stent deployment and optimization is typically efficient.
OUTCOMES AFTER CORONARY CHRONIC TOTAL OCCLUSION PERCUTANEOUS CORONARY INTERVENTION WITH DIFFERENT STRATEGIES
ADR represents an umbrella term that covers a spectrum of different approaches. The procedural efficacy of contemporary ADR varies with the complexity of the lesion and the extent of supplementary maneuvers that are required during the case.14) In the Recharge registry,15) the use of ADR as a technique either primarily or as a bailout during switching of strategies was an important facet of achieving 89% success overall. Closer examination of the ADR sub-group14) demonstrated 81% success with CrossBoss and Stingray as a primary technique. If supplementary techniques such as wire based redirection or knuckling were used, this reduced to 74% reflecting increased lesion and technical complexity. When used as a bailout for failed AW or retrograde based procedures the success was 61%. The CrossBoss alone crossed true-to-true in 7% of the successful ADR cases. Finally, wire-based re-entry also occurred in a small percentage (10%) of successful ADR cases (either bailout LAST or inadvertent mini-STAR close to the distal cap). Failure modes of ADR are well described and this procedure is most commonly limited by the formation of a distal hematoma at the landing zone16) or failure of equipment to reach the landing zone.14)
It is important that operators recognize that there are risks inherent to any CTO procedure irrespective of approach. This is particularly pertinent when lesions are complex and potentially amenable to 2 or more strategies. Large registry data show that retrograde approaches are associated with increased jeopardy compared to AW or ADR approaches. The need for retrograde access increases the risk of perforation and peri-procedural myocardial infarction.17) Therefore, it is important that cardiologists recognize procedural jeopardy and employ a strategy and or technologies under circumstances that make the procedure as safe as possible. For example, using ADR as a strategy may confer much less jeopardy than trying to cross small caliber, high-frequency and extremely tortuous epicardial collaterals retrogradely.
As noted, there have been poorer clinical outcomes described with historical ADR approaches. However, in centers where all of these strategies were applied, more contemporary ADR (and RDR) procedures are associated with vastly superior clinical results compared to the older methods of ADR.18) This has been confirmed in large clinical registries, where outcomes with modern targeted ADR in particular, appear equivalent to wire based approaches for 1-year major adverse cardiovascular events.19)20)21) RDR approaches have been associated with a small excess of target vessel revascularization (TVR). However, this particular approach is typically reserved for the most complex cases, where there are high Japanese CTO scores, high rates of post-coronary artery bypass grafting cases and stent lengths are very long.21) The finding of increased restenosis driving more TVR under these circumstances is not unsurprising.
CONCLUSION
There is no panacea in CTO PCI, with no single strategy, technology or approach offering a solution to the broad spectrum of lesions. ADR represents an important facet of both the hybrid and Asia-Pacific algorithms and in some patients may represent a safer approach to a lesion. The ability to utilize ADR based approaches amongst the other CTO PCI strategies enhances the overall success of the procedure. Finally, when successful, ADR procedures are associated with good clinical outcomes for patients that are comparable to wire based approaches in the medium term.
 XML Download
XML Download