

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Age-related macular degeneration (AMD) is a progressive disease of the macula that affects central vision. In industrialized countries, it is the leading cause of irreversible blindness in people aged 65 years or older.1 The prevalence of AMD is likely to increase due to the exponential increase in aging populations.2 The etiology of AMD is not clearly understood; however, several studies have suggested that immunologic and inflammatory processes34 and atherosclerosis5 are involved in its pathogenesis. In contrast, dietary intake of antioxidants has been associated with a decreased risk of exudative AMD.6 In Korea, the prevalence and incidence of wet AMD in a subset of the population aged 40 years or older were 36.43 (per 10000 people) and 3.02 (per 10000 person-years).7
Statins,8 metformin,9 angiotensin-converting enzyme (ACE) inhibitors,10 and angiotensin II receptor blockers (ARBs)11 are well-known medications that exert pleiotropic effects, such as anti-inflammatory and antioxidant effects, endothelium-protective actions, antiaggregatory and profibrinolytic effects, and atherosclerosis attenuation. Observational studies have examined the association of AMD with statins and ACE inhibitors. A systematic review reported that statin users experienced no preventive effect for AMD compared to non-users [relative risk (RR)=0.95, 95% confidence interval (CI)=0.74–1.15].12 Additionally, a nested case-control study found no decrease in the risk of AMD associated with ACE inhibitor use [odds ratio (OR)=1.19, 95% CI=1.07–1.33] compared with non-use.13 Thus far, no previous studies have examined the association of metformin and ARBs with AMD incidence.
Using a cohort of elderly patients from the Korean National Health Insurance Service database, this nested case-control study aimed to determine whether users of statins, metformin, ACE inhibitors, or ARBs had a reduced risk of AMD compared to that in non-users.
MATERIALS AND METHODS
Data sources
We used the National Health Insurance Service-National Elderly Cohort (NHIS-NEC) database from South Korea. South Korea introduced the National Health Insurance program in 1977, and gradually expanded its coverage until it achieved universal healthcare in 1989.14 NHIS collects the healthcare utilization records of the entire Korean population through claim data, which is generated by medical institutions for the reimbursement of costs covered by national insurance.15 Using the claim data, NHIS established a sample cohort database of elderly patients aged ≥60 years. Through simple random sampling, NHIS-NEC consists of 10% of the total population aged ≥60 years and eligible for health insurance or medical aid.16 This database includes demographic information and details on the healthcare services provided. Personal identification numbers were anonymized before providing information to researchers, and all diagnoses were coded according to the International Classification of Diseases, Tenth Revision (ICD-10).
Cohort construction
NHIS-NEC database was established from claim data from 2002–2015. Our study cohort included patients aged 65 years or older who were diagnosed with diabetes mellitus, including types 1 and 2 (ICD-10: E10–E14), or cardiovascular diseases (ICD-10: I05–I15, I20–I28, I30–I52, I60–I89) in 2002. This population was considered to contain patients with the aforementioned diseases, and cohort entry date was defined as the first date of diagnosis.
Case definition and control selection
We identified all incident patients with AMD between January 2012 and December 2015. Incident patients were defined as patients without a diagnostic history of degeneration of the macula and posterior pole (ICD-10: H35.3) before 2012, as diagnosis related to the disease of interest was specified by four digits in ICD code, which were introduced in 2011. Therefore, we excluded the patients who were diagnosed in 2011 or earlier from the study cohort. Cases were defined as all patients with incident AMD diagnosed with non-exudative (ICD-10: H35.30) or exudative (ICD-10: H35.31) AMD after the cohort entry date. To differentiate the cases from other cases with diseases related to the degeneration of the macula and posterior pole (ICD-10: H35.32–H35.39), we defined cases as patients with non-exudative or exudative AMD and not as those with other disease types. The first date of AMD diagnosis was defined as the index date. For each case, 10 controls were randomly selected by risk set sampling, and the controls were matched for sex, age, cohort entry date (±60 days), and follow-up duration.
Exposure definition
Statins, metformin, ACE inhibitors, and ARBs were the main exposures in this study. Therefore, we collected patient medication history until one year prior to index data collection. We defined exposure as a prescription history for single or combination administration of the aforementioned medications. Patients who were prescribed more than two types of these medications were defined as combination users, whereas the remaining patients were considered non-users. For subgroup analysis, we classified exposure more specifically according to the cumulative duration and timing of medication use. Cumulative duration was calculated as total days of medication prescription without duplicated days, and it was classified into three categories as follows: 1) fewer than 90 days, 2) fewer than 300 days, and 3) greater than 300 days. Additionally, the timing of medication use was classified into three categories as follows: 1) recent use, 2) current use, and 3) past use. We defined recent use as when the latest administration duration of the study medications overlapped with the index date. Current use was defined as cases in which the latest administration duration of the study medications occurred within 30 days from the index date, whereas the remaining cases were defined as past use.
Potential confounders
The following baseline characteristics and clinical details for all of the study subjects were considered possible confounders of the association between medication use and AMD: income level, health insurance type, Charlson comorbidity index, number of healthcare resources used, disease history, and medications. Disease history included cerebrovascular disease, complicated diabetes, uncomplicated diabetes, hyperlipidemia, hypertension, liver disease, myocardial infarction, and peripheral vascular disease. Medication history included the use of alpha-blockers, alpha-glucosidase, aspirin, beta-blockers, calcium channel blockers, diuretics, meglitinide, sulfonylurea, and thiazolidinedione. Claim data from over one year before the index date were used to define the number of healthcare resources used and disease and medication history.
Statistical analysis
We conducted a nested case-control study to investigate the preventive effect of statins, metformin, ACE inhibitors, ARBs, and their combinations on AMD. To compare the general characteristics between the case and control groups, we described categorical data with frequencies or proportions and continuous data with means and standard deviations. Furthermore, we conducted chi-square tests for unmatched categorical variables. To overcome the multiplicity problem for variables with more than two groups, we applied Bonferroni method. The level of significance was adjusted by 0.05/k, where k was the number of groups for each variable. For primary analysis, we used conditional logistic regression to estimate the ORs and corresponding 95% CIs for AMD in patients who used the study medications and their combinations versus non-users. These ORs assume unbiased estimates of the hazard ratios due to the use of risk set sampling.17 To adjust conditional logistic regression model, we used all of the potential confounders previously defined. For secondary analysis, we repeated the primary analysis, including cumulative duration and timing of medication use. To identify statistically significant differences in variables, including age, sex, AMD type, and several comorbidities, between cases and controls, we performed an interaction test and conducted subgroup analyses for variables with interaction effects. All statistical analyses were performed using SAS 9.4 for Windows (SAS Institute, Inc., Cary, NC, USA). The present study protocol was reviewed and approved by the Institutional Review Board of Sungkyunkwan University (approval no. 2018-02-008).
RESULTS
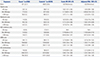
Of the 231274 patients diagnosed with diabetes mellitus or cardiovascular diseases in 2002, the study cohort included 200333 patients (Fig. 1), with 2330 incident cases and their 23278 matched controls. Matching ratio by risk set sampling was 1:9.99. There were several substantial differences in the baseline characteristics of subjects (Table 1). Cases were more likely to show greater healthcare resource use and higher Charlson comorbidity index and prevalence of comorbidities, including cerebrovascular diseases, complicated diabetes mellitus, uncomplicated diabetes mellitus, and peripheral vascular diseases. Moreover, compared with controls, cases were more likely to have a history of combined medication use, excluding aspirin, beta-blockers, and thiazolidinedione.
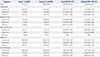
Compared to non-users, the adjusted ORs and their 95% CIs for the occurrence of AMD in users of statins, metformin, ACE inhibitors, ARBs, and all medication combinations were 1.12 (0.94–1.32), 1.15 (0.91–1.45), 0.90 (0.61–1.34), 1.21 (1.05–1.39), and 1.21 (1.06–1.38), respectively (Table 2).
In secondary analyses, there were no significant associations of AMD prevention with the long-term use and timing of medication use for any of the medications evaluated (Tables 3 and 4). This finding was supported by the results of subgroup analyses for age group, sex, and peripheral vascular disease presence. Interaction test showed a significant difference in the results according to the type of AMD and presence of cerebrovascular diseases; however, the results of subgroup analyses were statistically insignificant (Fig. 2).
DISCUSSION
We found that statin, metformin, ACE inhibitor, or ARB use did not decrease the risk of AMD in an aged population after adjusting for several potential confounders, such as socioeconomic status, healthcare resource utilization, combined medication use, and comorbidities. No significant associations were observed between AMD risk and cumulative duration or timing of medication use. Additionally, there were no considerable differences between age groups, sex, AMD types, presence of cerebrovascular or peripheral vascular diseases, and uncomplicated or complicated diabetes mellitus.
Several studies have investigated the association between the risk of AMD and statins, and found no preventive effects. A case-control study suggested that statin use and AMD incidence have no association (OR=0.93, 95% CI=0.81–1.07).18 In a 5-year cohort study, statins did not prevent early age-related maculopathy (early onset: OR=1.12, 95% CI=0.47–2.67; progression: OR=1.22, 95% CI=0.54–2.76; late incidence: OR=0.41, 95% CI=0.12–1.45).19 In contrast, a nested case-control study reported a risk for AMD with statin use (OR=1.30, 95% CI=1.17–1.44).13 However, the findings of other studies conflict with our results. According to one cross sectional study,20 the relationship between statin use and AMD was negative (OR=0.14, 95% CI=0.02–0.83). Moreover, several studies have demonstrated preventive effects of statins.212223
Some studies have investigated the association between the risk of AMD and use of ACE inhibitors or ARBs. A nested casecontrol study reported that ACE inhibitor use may be associated with an increased risk of AMD (adjusted RR=1.19, 95% CI=1.07–1.33).13 A study that analyzed data pooled from three population-based cohort studies found no significant relationship between ACE inhibitor use and the incidence of early age-related maculopathy in each of the three cohort studies, as well as in the pooled cohort (OR=1.1, 95% CI=0.8–1.5).24 A case-control design study showed that ARBs have a protective effect on the development of choroidal neovascularization, which is a late form of AMD, in patients with AMD.25 However, these authors concluded that ARBs were unlikely to confer a preventive effect against choroidal neovascularization in patients with AMD.
We examined whether these medications protected against AMD using a nested case-control study design. This observational study design integrates the concept of traditional case-control studies within a constructed cohort.26 Moreover, this study design overcomes some of the disadvantages associated with case-control studies, while incorporating the advantages of cohort studies. Particularly, selection bias, which is a considerable concern in traditional case-control studies, is minimized by selecting cases and controls from populations with the same risk. Moreover, information bias is decreased. However, this study design had some disadvantages, including the fact that all pertinent risk factors were not recorded and the statistical power was low due to the small sample sizes.
Our study had several strengths. First, we used NHIS-NEC data sourced from a well-established and validated national longitudinal database, and included follow-up data from 2002–2015 for 558147 elderly subjects. Additionally, this database was constructed by collecting reimbursement data from all inpatient and outpatient claim records under a fee-for-service system, enabling researchers to collect detailed information about the utilization of healthcare resources. Second, the results of this study have high external validity and generalizability, since the database we used included data from the entire population of South Korea. Therefore, our findings reflect the realworld situation.
There were some limitations to this study. Although the claim database we used contained a large sample that was representative of the population, there are concerns regarding its validity. AMD cases were defined according to the diagnoses listed in the database, which may differ from the actual diagnoses received by the patients. Although the overall positive predictive value of diagnosis was 70%,27 validity remains an issue. Additionally, information on medication use was based solely on prescriptions, and the actual administration may have differed. Furthermore, we could not include variables related to lifestyle, family history, and cardiovascular factors (e.g., blood pressure, HbA1c, and lipid profile), which are possible risk factors of AMD, as this information was absent from the database. However, confounding by cardiovascular factors would be limited since our study design included a cohort of patients with cardiovascular diseases or diabetes mellitus and adjustments for comorbidities relevant to cardiovascular disorders. Moreover, there is a possibility of selection bias in which actual patients with AMD were misclassified as controls, since we could not confirm the use of optical coherence tomography, which was not a reimbursed procedure during the study period, for the diagnosis of AMD. However, this would not cause substantial bias in our results, since there is no conclusive evidence for differential disease misclassification rates between exposed and unexposed patients. Finally, a previous study showed that statins have protective effects against early-stage and exudative AMD. However, we could not conduct a subgroup analysis for AMD stage as specific stages could not be identified using our database. Moreover, in the database, there was no information about the number of treated eyes. Therefore, the intracorrelation between eyes could not be investigated. This limitation may have masked any preventive effects of the medications.
In conclusion, we found no evidence that statins, metformin, ACE inhibitors, or ARBs prevented the occurrence of AMD in elderly patients. We also found no significant relationships between the risk of AMD and duration-response or timing of medication use. Moreover, we found no significant differences between age groups, sex, AMD types, and presence of cerebrovascular diseases, complicated or uncomplicated diabetes mellitus, or peripheral vascular diseases.




 XML Download
XML Download