

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
With aging of the global population, the incidence of joint diseases in older adults has increased year by year. Total knee arthroplasty is one of the main methods of treating knee joint diseases.12 Although total knee arthroplasty can significantly improve the quality of life and walking ability of older adult patients, the risk of postoperative deep venous thrombosis (DVT) is high in these patients: a study has reported that the incidence of DVT after total knee arthroplasty is about 5–22%.3 In recent years, due to the increase of total knee arthroplasty surgeries in older adult patients, the incidence of DVT has also followed an increasing trend.4
The treatment of anticoagulant drugs can significantly reduce the risk of postoperative DVT.5 Low molecular weight heparin (LMWH) is a commonly used medicine for the prevention and treatment of DVT after orthopedics surgery. A study has reported that LMWH is effective and can significantly reduce the incidence of DVT within 3 months after total knee arthroplasty.6 However, LMWH also has many limitations, especially in older adult patients discharged from the hospital. For example, the subcutaneous injection method is complicated, medication compliance is poor, blood coagulation function needs to be regularly monitored, and so on.7 In recent years, new anticoagulant oral preparations have been developed. Apixaban is a new potent oral FXa inhibitor that can rapidly combine with FXa and transform prothrombin into thrombin.89 One study has shown that apixaban can significantly reduce the incidence of DVT and the associated mortality after orthopedic surgery.10 At present, there are few clinical studies comparing the efficacy of apixaban and LMWH in preventing and treating DVT after total knee arthroplasty in older adult patients. Therefore, this research sought to compare the efficacy of apixaban and LMWH in older adult patients undergoing total knee arthroplasty in order to provide an experimental and theoretical basis for the development of clinical anticoagulant strategies therein.
MATERIALS AND METHODS
General information
A total of 220 older adult patients undergoing total knee arthroplasty admitted to our hospital from January 2015 to November 2017 were selected. They were randomly divided into apixaban and LMWH groups (110 patients in each group). Patients in the apixaban group were treated with apixaban orally at 12 h after surgery, twice a day, 2.5 mg each time.11 Patients in the LMWH group were given LMWH (purchased from GlaxoSmithKline Co., Ltd., Tianjin, China) via hypodermic injection at 12 h after surgery, 4000 IU per day.12 The doses of apixaban and LMWH were not adjusted according to indicators such as activated partial thromboplastin time (APTT). The course of treatment in the two groups both lasted for 5 weeks. Alleviating analgesia and early ambulation were routinely conducted for postoperative patients. This study was approved by the Ethics Committee of Jinling Hospital (2016NZKY-020-02). All patients or their families signed informed consent.
The inclusion criteria were older adults (>60 years old), patients with total knee arthroplasty indications, patients without surgical contraindications, and patients with no history of DVT before surgery. Exclusion criteria were patients with malignant tumors; patients with liver, kidney, heart, lung, or other important organ dysfunction; patients with blood coagulation dysfunction; patients whose preoperative ultrasonography of blood vessels revealed DVT; patients who were allergic to the drugs being studied in this research; patients with a history of mental illness; patients who refused to provide informed consent; and patients who did not meet the experimental ethical standards.
Observation index
The visual analogue scale (VAS) scoring system was used to evaluate pain experienced by patients before surgery and at the end of treatment. VAS scores ranged from 0 to 10, with 0 indicating no pain and 10 indicating severe pain.
The incidence of DVT between the two groups within 3 months after surgery were compared. The clinical manifestations of symptomatic DVT were dark purple skin, elevated skin temperature, swollen lower limbs, shallow vein engorgement, and tenderness in the femoral triangle, which was confirmed by color doppler ultrasound. If there were no symptoms, color doppler ultrasound was used to examine for DVT. The patients were re-checked by ultrasound once every 2 weeks, with follow up by outpatient appointment after discharge.
Blood coagulation function indexes in two groups were compared. APTT, prothrombin time (PT), platelets (PLT), and fibrinogen (FIB) were measured using a full-automated blood coagulation analyzer at 1 week after surgery, 3 weeks after surgery, and the end of treatment, and then averaged. Also, we compared hemodynamic indexes of the two groups, including capillary plasma viscosity and erythrocyte aggregation. Hemodynamic indexes were evaluated at 1 week after surgery, 3 weeks after surgery, and the end of treatment, and then averaged.
The movement ability and state of knee joint were compared between the two groups. The hospital for special surgery (HSS) knee joint scoring system was used to evaluate postoperative function of the knee joint at 1 week after surgery, 3 weeks after surgery, and the end of treatment, and mean values were calculated to compare patients in the two groups. The HSS scoring system comprises six main aspects, including pain, function, joint mobility, muscle strength, knee flexion deformity, and knee instability, with a total score of 100 points. The higher the score, the better the movement ability and state of the knee joint.
Adverse reactions in the two groups were compared. Postoperative drainage volume, bleeding events (cerebral hemorrhage, primae viae bleeding, and subcutaneous hemorrhage), and liver and kidney function were observed.
Statistical analysis
SPSS 20.0 statistical software (IBM Corp., Armonk, NY, USA) was used to analyze all data. Measurement data were expressed as a mean±standard deviation (ˉx ±SD). The t test was used for comparisons between groups, and paired t test was used for the comparison of indicators before and after intervention. The comparison of indexes at different time points was analyzed by ANOVA of repeated measurements combined with post-Bonferroni test. Enumeration data are expressed as percentages, and the χ2 test was used for comparison between groups. There was a significant difference at p<0.05.
±SD). The t test was used for comparisons between groups, and paired t test was used for the comparison of indicators before and after intervention. The comparison of indexes at different time points was analyzed by ANOVA of repeated measurements combined with post-Bonferroni test. Enumeration data are expressed as percentages, and the χ2 test was used for comparison between groups. There was a significant difference at p<0.05.
±SD). The t test was used for comparisons between groups, and paired t test was used for the comparison of indicators before and after intervention. The comparison of indexes at different time points was analyzed by ANOVA of repeated measurements combined with post-Bonferroni test. Enumeration data are expressed as percentages, and the χ2 test was used for comparison between groups. There was a significant difference at p<0.05.RESULTS
Comparison of basic data
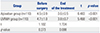
Between the two study groups, there were no significant differences in gender, age, body mass index, underlying disease, duration of operation, discharge time, ratio of general anesthesia to intraspinal anesthesia, expanded medical structure number, intraoperative blood loss, blood transfusion volume, and postoperative analgesia satisfaction (all p>0.05) (Table 1).
Comparison of VAS scores
There was no significant difference in preoperative VAS scores between the two groups. There was also no significant difference in VAS scores between the two groups at the end of treatment. VAS score of the end of the treatment, however, was significantly lower than that of before surgery in both groups (Table 2).
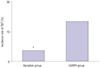
Comparison of the incidence of DVT
Vascular ultrasound revealed DVT in 6 patients in the apixaban group, including three in the iliac vein, one in the femoral vein, and two in the popliteal vein. There were 22 cases of DVT in the LMWH group, including 12 in the iliac vein, six in the femoral vein, and four in the popliteal vein. There was a significant difference in the incidences of DVT between the two groups (5.5% vs. 20.0%, χ2=410.480, p=0.001) (Fig. 1).
Comparison of blood coagulation function indexes
ANOVA of repeated measurements revealed significant differences in APTT, PT, PLT, and FIB at different time points. APTT and PT indexes were increased and PLT and FIB indexes were decreased at 1 week after surgery, 3 weeks after surgery, and the end of treatment in two groups, compared to before surgery. APTT and PT indexes in the apixaban group were higher than those in the LMWH group at 1 week after surgery, 3 weeks after surgery, and the end of treatment, while PLT and FIB indexes were lower than those in the LMWH group (Table 3, Fig. 2).
Comparison of hemorheology indexes
ANOVA of repeated measurements showed significant differences in capillary plasma viscosity and erythrocyte aggregation at different time points. Capillary plasma viscosity and erythrocyte aggregation index values at 1 week after surgery, 3 weeks after surgery, and the end of treatment in two groups were significantly lower than those before surgery. Capillary plasma viscosity and erythrocyte aggregation in the apixaban group were significantly lower than those in the LMWH group at 1 week after surgery, 3 weeks after surgery, and the end of treatment (Tables 4 and 5, Figs. 3 and 4).
Comparison of HSS scores
The HSS scores for patients in the apixaban group at 1 week, 3 weeks, and 5 weeks after surgery were 82.4±6.5, 85.7±7.1, and 89.5±8.4, respectively. The HSS scores for patients in the LMWH group at 1 week, 3 weeks, and 5 weeks after surgery were 80.9±6.2, 84.1±6.9, and 87.4±7.9, respectively. ANOVA of repeated measurements showed that there were no significant differences in HSS scores at the different time points between groups (Table 6).
Comparison of adverse reactions
No deaths occurred during follow up in either group, and no liver and kidney function damage occurred during medication. In the LMWH group, some patients experienced ecchymosis and allergic reactions at the injection site, which recovered after active symptomatic treatment. Some patients in the apixaban group complained of nausea and anemia, and recovered significantly after symptomatic treatment. Compared with the LMWH group, postoperative drainage volume in the apixaban group was significantly lower (215.7±20.5 mL vs. 298.2±26.2 mL, t=4.295, p=0.013). There was no significant difference in the incidence of bleeding events between groups (10.9% vs. 5.5%, χ2=1.089, p=0.297) (Fig. 5).
DISCUSSION
DVT is a common complication after clinical orthopedic surgery, especially in older adult patients undergoing artificial joint arthroplasty. The formation of DVT can lead to organ dysfunction, such as pulmonary embolism and so on, which is one of the major causes of perioperative death and seriously threatens the life and health of patients.11 One study has reported that the incidence of DVT after artificial joint arthroplasty can reach up to 30%, if no corresponding measures are taken.12 The high incidence of DVT in older adult patients after artificial joint arthroplasty may be associated with more underlying diseases in older adult patients, physiological function degeneration, blood in a hypercoagulable state, a lack of postoperative functional exercise, surgical injury to the vascular endothelium, and activation of the coagulation-fibrinolytic system.1314
At present, the prevention and treatment of DVT after artificial joint arthroplasty have primarily relied on drug therapy with LMWH, unfractionated heparin, and vitamin K antagonists. Although these drugs have a desirable effect, there are also many adverse reactions.1516 Therefore, it is of great significance to find a safe and effective drug to prevent DVT after artificial joint arthroplasty in older adult patients. LMWH has been widely used as a thromboprophylaxis drug after total knee arthroplasty. LMWH can target complex enzymes in the internal and external pathways of the coagulation cascade, and it can also be combined with anticoagulant enzymes to enhance its effect.17 However, research has shown that it is inconvenient for patients undergoing total hip arthroplasty, especially for older adults, given its route of administration.18 Apixaban, a new type of oral anticoagulant, has a simpler route of administration than LMWH. Through the selective inhibition of the coagulation FXa, apixaban can block endogenous and exogenous pathways generated by thrombin and can inhibit thrombus formation.19 In recent years, a study revealed that apixaban has a certain effect in the prevention and treatment of DVT after surgery of hip fracture.20 However, the differences in the prevention of DVT between apixaban and LMWH in older adult patients undergoing total knee arthroplasty have remained unclear. The results of the present study showed a significantly lower incidence of DVT with apixaban than with LMWH. The study of Lanitis, et al.21 also suggested that apixaban had obvious advantages in the prevention and treatment of DVT, compared with LMWH. Notwithstanding, previous research has reported that there was no significant difference in the incidence of DVT between the apixaban group and the LMWH group, which may be due to the subject selection (older adult patients), different sample size, and patient compliance in this study.10
In terms of blood coagulation function and hemorheology indices, the results of this research showed that blood coagulation function and hemorheology after intervention in the apixaban group were significantly better than those in the LMWH group. In the aspect of adverse drug reactions, postoperative drainage volumes in the apixaban group were significantly lower than those in the LMWH group. While the incidence of bleeding events in the apixaban group was higher than that in the LMWH group, the difference was not statistically significant. These findings further indicate that apixaban is more effective than LMWH in the prevention of DVT after total knee arthroplasty in older adult patients, as it elicits fewer adverse reactions and is safer. The results of a study on 520 acute symptomatic DVT patients who received different doses of apixaban also showed that apixaban was effective in reducing DVT and was safe.22
There are certain limitations in this research. Although digital subtraction angiography is the “gold standard” for the diagnosis of DVT, in view of its large trauma and high cost, vascular doppler ultrasound examination was used in this study. Also, the sample size enrolled in this study was small, and this study reflects results at a single center. Further studies need to collect and increase the number of cases and conduct prospective studies of multi-center follow-up control, confirming changes in index values at multiple time points, studying the risk of thrombosis over a longer period of time, and studying drugs at different doses.
In summary, the efficacy and safety of apixaban in the prevention of DVT after total knee arthroplasty in older adult patients was better than that of LMWH. Apixaban, as an oral agent, is an effectively antithrombotic and anticoagulant drug worth promoting in the treatment of DVT after artificial joint arthroplasty.








 XML Download
XML Download