

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Current guidelines recommend post-mastectomy radiation therapy (PMRT) for patients who have four or more metastatic lymph nodes (LNs) following primary mastectomy [12]. However, the benefit of PMRT in patients with pN1 tumors remains controversial [3]. Recently, the use of neoadjuvant chemotherapy (NAC) has been increasing, especially for node-positive breast cancer. Although current guidelines recommend deciding on PMRT based on initial clinical stages before NAC [4], the indication for PMRT following NAC has not yet been established [5].
Residual LN disease (ypN+) is the most unfavorable prognostic factor. PMRT cannot be omitted for high-risk patients who have residual LN disease following NAC and mastectomy [6]. However, in patients who achieve ypN0 following NAC, the role of PMRT is controversial [7]. We have previously reported that PMRT is not significantly related to clinical outcomes in those who have achieved ypN0 following NAC and mastectomy in our multi-institutional study called Korean Radiation Oncology Group (KROG) 12-05 [8].
Recently, several studies have demonstrated different benefits of PMRT depending on intrinsic molecular subtypes in adjuvant chemotherapy settings [91011]. However, the benefit of PMRT in NAC settings has not yet been addressed. In our previous study, molecular subtypes were unknown in 20% of patients and only 6% of patients with human epidermal growth factor receptor 2 (HER2)-positive cancer received HER2-targeted therapy, limiting further investigation using previous data [8].
Therefore, the objective of this study was to collect multi-institutional data containing complete information about molecular subtypes to investigate if the benefit of PMRT is different according to molecular subtype in patients who achieve ypN0 following NAC.
METHODS
Patients
A total of 450 patients initially suspected with axillary disease who achieved ypN0 following NAC were enrolled from 13 institutions of the KROG between January 2005 and December 2011. This study was approved by all participating institutions' Institutional Review Boards (IRBs). Each IRB approved a waiver of informed consent. The IRB number of the representative institution was 2015-11-111. We excluded patients with a history of previously receiving radiation therapy, a history of previous or concurrent malignancy except for thyroid cancer at the time of diagnosis, distant metastases, clinically positive supraclavicular or internal mammary LNs, or unclassified HER2 status. Of 450 patients, 189 were analyzed in this study. According to immunohistochemistry (IHC) expression of primary tumors, these patients were classified into three molecular subtypes: luminal (estrogen receptor [ER]- or progesterone receptor [PR]-positive), HER2 (ER- and PR-negative and HER2-positive), or triple-negative (ER-, PR-, and HER2-negative). HER2 overexpression was defined when HER2 expression was detected as grade 2 or 3 on IHC and confirmed by fluorescence in situ hybridization or a silver in situ hybridization test.
Treatment
Axillary LN confirmation based on fine-needle aspiration before NAC was performed in 104 (55.0%) patients. The remaining 85 patients were assessed by either positron emission tomography–computed tomography (n = 41), magnetic resonance imaging (n = 24), or ultrasonography (n = 58). The most frequently used regimen for NAC was anthracycline plus taxane (AT, n = 105, 55.6%), followed by anthracycline plus cyclophosphamide followed by taxane (AC-T, n = 43, 22.8%), anthracycline plus cyclophosphamide (AC, n = 19, 10.1%), and taxane only (n = 7, 3.7%). Other regimens (n = 14, 7.4%) included fluorouracil plus AC (n = 5), gemcitabine plus taxane (n = 8), and herceptin alone (n = 1). The median number of NAC cycles administered was 4 (range, 2–9). Neoadjuvant HER2-targeted therapy was delivered to 15 (7.9%) patients.
All patients underwent mastectomy following NAC. For axillary management, 172 (91.0%) patients underwent axillary LN dissection and 17 (9.0%) patients underwent sentinel LN biopsy only. The median number of sampled LNs was 13 (range, 1–44). Adjuvant chemotherapy was delivered to 121 (64.0%) patients. The most common regimen was AT (n = 82, 43.2%), followed by AC (n = 14, 7.4%). The median number of cycles of adjuvant chemotherapy administered was 3 (range, 1–8). Adjuvant hormone treatment was administered to 89.5% (77/86) of patients with luminal-type tumors, while adjuvant HER2-targeted therapy was delivered to 69.5% (57/82) of patients with HER2-positive tumors.
Among all patients, 111 (58.7%) received PMRT. The median radiation dose to the chest wall was 50.4 Gy (range, 45–54 Gy) with 1.8–2.0 Gy per fraction. Elective nodal irradiation (ENI) including the supraclavicular region was performed in 98 (51.9%) patients. Fifty-four (28.6%) patients received internal mammary irradiation. The median ENI dose was 50.4 Gy (range, 45–54 Gy) with 1.8–2.0 Gy per fraction.
Statistical analysis
Categorical variables according to PMRT were compared using the χ2 or Fisher's exact test. Loco-regional recurrence (LRR) was defined as disease recurrence within the ipsilateral chest wall or regional lymphatic area (axillary, supraclavicular, or internal mammary LNs). The time from the initiation of NAC to LRR or death was defined as loco-regional control (LRC). The time from the initiation of NAC to any recurrence or death was defined as disease-free survival (DFS). Overall survival (OS) was defined as the time from the initiation of NAC to death from any cause. LRC, DFS, and OS rates were estimated using the Kaplan-Meier method and compared between subgroups using log-rank tests. All factors with p < 0.1 by univariate analysis were included for multivariate analysis. In multivariate analysis for survival, the Cox proportional hazards model was used to calculate hazard ratios and 95% confidence intervals. A p-value < 0.05 was considered statistically significant. All statistical analyses were conducted using SPSS Statistics version 20 (IBM Corp., Armonk, USA).
RESULTS
Patient characteristics
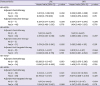
Distributions of characteristics according to PMRT are summarized in Table 1. The PMRT group had more advanced clinical T-stages (cT3–4: 62.2% vs. 34.6%, p < 0.001) and advanced N-stages (cN2–3: 40.5% vs. 26.9%, p = 0.053). Distributions of other factors including histology, subtype, histologic grade, ypT stage, resection margin status, axillary management, and lympho-vascular invasion (LVI) did not differ significantly according to PMRT.
Table 1
Patient characteristics and treatment according to adjuvant radiation therapy

Values are presented as number (%).
PMRT = post-mastectomy radiation therapy; IDC = invasive ductal carcinoma; ILC = invasive lobular carcinoma; HER2 = human epidermal growth factor receptor 2; NAC = neoadjuvant chemotherapy; AC = anthracycline plus cyclophosphamide; AT = anthracycline plus taxane; ACT = anthracycline plus cyclophosphamide followed by taxane; SLNB = sentinel lymph node biopsy; ALND = axillary lymph node dissection; LVI = lympho-vascular invasion.
![]()
Clinical outcomes in all patients
The median follow-up duration was 78.0 (range, 3.0–149.0) months. Five-year LRC, DFS, and OS rates for all patients were 91.9%, 77.1%, and 89.3%, respectively. Among all patients, 46 (24.3%) developed recurrence. Most of these patients (n = 30, 65.2%) developed distant metastasis, while 11 (23.9%) patients developed distant metastasis and LRR simultaneously. Only 5 patients (10.9%) developed isolated LRR (Figure 1).

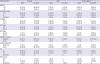
The prognostic significance of several factors (including age, molecular subtype, histologic grade, cT stage, cN stage, ypT stage, LVI, resection margins, axillary dissection, PMRT, and adjuvant systemic therapy) was analyzed using univariate analyses (Table 2). Age, cT stage, cN stage, ypT stage, and axillary dissection were not significant factors for clinical outcomes (LRC, DFS, or OS). Significant factors for LRC and DFS were LVI (p = 0.008 and p < 0.001, respectively) and close resection margins (both p < 0.001). Histologic grade (p = 0.011), LVI (p = 0.032), and adjuvant endocrine therapy (p = 0.020) were significant factors for OS. The prognostic effect of PMRT on DFS or OS was not significant, although it was marginally significant on LRC (p = 0.075).
Table 2
Prognostic factors for LRC, DFS, and OS by univariate analysis

LRC = loco-regional control; DFS = disease-free survival; OS = overall survival; HER2 = human epidermal growth factor receptor 2; LVI = lympho-vascular invasion; SLNB = sentinel lymph node biopsy; ALND = axillary lymph node; Adj. = adjuvant.
![]()
In multivariate analysis, LVI and close resection margins were unfavorable factors for LRC (p = 0.014 and p < 0.002, respectively) and DFS (p = 0.001 and p < 0.001, respectively). The only significant factor for OS was LVI (p = 0.005). The prognostic effect of PMRT on LRC was not significant in multivariate analysis (p = 0.641, Table 3).
Table 3
Prognostic factors for LRC, DFS, and OS by multivariate analysis

LRC = loco-regional control; DFS = disease-free survival; OS = overall survival; CI = confidence interval; LVI = lympho-vascular invasion; RM = resection margin; PMRT = post-mastectomy radiation therapy.
![]()
Role of PMRT in subgroup analysis
The prognostic significance of PMRT for LRC and DFS was evaluated in different subgroups (Table 4). The effect of PMRT on LRC differed by molecular subtype (p for interaction = 0.019). However, the effect of PMRT on DFS did not differ by molecular subtype (p for interaction = 0.678). PMRT was not a significant factor for LRC or DFS in subgroup analysis by clinical stage or adjuvant treatment (Table 4). Figure 2 shows the LRC curves according to PMRT for different molecular subtypes. In the luminal subtype (Figure 2A), LRC was greater in patients who received PMRT than that in those who did not (p = 0.046). However, LRC did not differ according to PMRT in patients with either HER2-type (Figure 2B) or triple-negative type (Figure 2C) tumors. To identify the role of PMRT independent from adjuvant treatment, we further assessed the prognostic effect of PMRT on LRC and DFS in diverse adjuvant treatment settings (Table 5). In all subgroups, adjuvant PMRT was not a significant factor for LRC and DFS.
Table 4
Effect of post-mastectomy radiation therapy on LRC and DFS in subgroups by univariate analysis

LRC = loco-regional control; DFS = disease-free survival; CI = confidence interval; HER2 = human epidermal growth factor receptor 2; Adj. = adjuvant.
*p for interaction.
![]()
 | Figure 2Kaplan-Meier curves of LRR according to PMRT in subgroups by molecular subtype and residual breast disease. LRR according to PMRT in the (A) luminal subtype (n = 86), (B) HER2 subtype (n = 49), and (C) triple-negative subtype (n = 54).LRR = loco-regional recurrence; PMRT = post-mastectomy radiation therapy; HER2=human epidermal growth factor receptor 2.
|
Table 5
Effect of post-mastectomy radiation therapy on LRC and DFS in subgroups by subtypes and adjuvant systemic treatment
LRC = loco-regional control; DFS = disease-free survival; CI = confidence interval; HER2 = human epidermal growth factor receptor 2; HR = hormone receptor; N/A = not applicable.
![]()
DISCUSSION
The current guidelines recommend PMRT according to the worst clinical and pathologic stages in NAC settings [4]. If the pathologic stage following NAC does not differ from the initial stage, the decision to administer PMRT is not difficult. However, if an initially evident nodal disease or large breast mass disappears following NAC, the decision regarding PMRT administration becomes complicated. In this study, as expected, those who received PMRT had higher proportions of advanced clinical stages than those who did not receive PMRT, suggesting that the use of PMRT had been chosen mainly in terms of initial clinical stage even if patients achieved ypN0. However, PMRT was not significantly related to clinical outcomes in either clinical T stage or N stage subgroups in the current study (Table 4). Similarly, Kantor et al. [12] reported that the survival benefit of PMRT in patients with clinically LN-positive disease disappears if they achieve ypN0 following NAC. Therefore, candidates for PMRT may be selected based on clinicopathological factors other than initial clinical stage.
The significance of PMRT in patients who achieve ypN0 following NAC and mastectomy has been investigated in several studies with inconsistent results. Our group has previously revealed that DFS is not different according to PMRT in patients who achieve ypN0 [8]. A French study and National Cancer Database (NCDB) analysis have also shown that PMRT does not improve OS in patients who achieve ypN0 [1314]. Conversely, another NCDB analysis suggested that PMRT is associated with better OS in patients who achieve ypN0 [15]. Rong et al. [16] investigated the role of PMRT in achieving ypN0 following NAC and mastectomy and suggested that PMRT can improve LRC and DFS, especially in cT3–4 disease. The present study showed that LRC, DFS, and OS did not differ between patients who received PMRT and achieved ypN0 and those who did not receive PMRT and achieved ypN0, similar to the results of our previous study. The most relevant factors for LRC and DFS were LVI and close resection margins in multivariate analysis. The association between the presence of LVI after NAC and poor prognosis has been demonstrated in several other studies [171819]. Close resection margins have been reported to be present in 6.1%–12.5% of patients following mastectomy [2021]. Close or involved resection margins have been suggested to be a predictor for LRR in patients who have undergone mastectomy without NAC [2223]. The present study suggests that close resection margins might also be a predictor for worse LRC and DFS in patients who have received NAC before mastectomy.
Subgroup analysis revealed a significant improvement in LRC by PMRT in the luminal subtype in univariate analysis (Table 4), but not in multivariate analysis (Table 5). A greater benefit of PMRT in the luminal subtype has been demonstrated in several studies [91011]. All these studies included cases of primary resection without NAC. In the second analysis of the Danish Breast Cancer Cooperative Group (DBCG) trial [9], the benefit of PMRT for survival was the largest for the luminal subtype. Tseng et al. [10] also analyzed the effect of PMRT on LRR according to subtype and showed that PMRT can reduce LRR in the luminal subtype, although it does not improve LRR in the triple-negative subtype. Laurberg et al. [11] examined different benefits of PMRT according to molecular subtype using data of two randomized trials: the British Columbia trial and DBCG 82b trial. They also found that the benefit of PMRT in lowering LRR was the largest for the luminal subtype. However, this study suggested that the benefit of PMRT in luminal subtypes disappears after adjusting for other factors including adjuvant systemic therapy. Although it was not significant, LVI and close resection margins were more frequent in the no-PMRT group of the luminal subtype compared to the PMRT group (Table 6). These factors might have induced lower LRC in the no-PMRT group in univariate analysis.
Table 6
Patient characteristics according to subtypes and radiotherapy
Values are presented as number (%).
PMRT = post-mastectomy radiation therapy; IDC = invasive ductal carcinoma; LN = lymph node; SLNB = sentinel lymph node biopsy; ALND = axillary lymph node dissection; LVI = lympho-vascular invasion; LRR= loco-regional recurrence; DM = distant metastasis
*p < 0.05 by χ2 test.
![]()
This multi-institutional study included heterogeneous systemic treatment and radiation therapy techniques, thereby limiting conclusive interpretation of the results. Particularly, subgroup analyses to identify the independent effect of PMRT in diverse treatment settings failed to show informative results because of the small number of patients. Furthermore, due to its retrospective nature, there might be considerable selection bias regarding the administration of PMRT. A randomized trial, the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-51 trial, is ongoing to evaluate the role of PMRT in patients who achieve ypN0. The results of the NSABP B-51 trial could provide guidance regarding optimal radiation therapy strategies for patients who achieve ypN0. Nevertheless, this was the first study to investigate the different effects of PMRT according to molecular subtype in patients who initially had LN disease and achieved ypN0 following NAC. The results of this study suggest that we should not underestimate the effect of PMRT in patients with the luminal subtype who achieve ypN0 by assuming that they would have excellent survival.
In conclusion, the benefit of PMRT was not found in any molecular subtype among patients who achieved ypN0 following NAC and mastectomy.
 XML Download
XML Download