

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Chronic inflammation resulting from oxidative stress has been considered as an important risk factor in the pathophysiology of various diseases, such as diabetes mellitus, rheumatoid arthritis, arteriosclerosis, Alzheimer's disease, and various cancers [1]. Inflammatory mediators, such as growth factors, cytokines, prostaglandins, reactive oxygen species, and reactive nitrogen species exist in cancer microenvironments and may lead to both genetic and epigenetic modifications resulting in the activation of oncogenes, the inactivation of tumor-suppressor genes, and the induction of chromosomal rearrangement, gene fusion, and gene amplification [2]. The interleukin (IL)-1 superfamily of cytokines comprises 7 molecules with agonist activity (ILα and β, IL-18, IL-33, IL-36α, β, and γ), 3 receptor antagonists (IL-1Ra, IL-36Ra, and IL-38), and an anti-inflammatory cytokine (IL-37) [3]. The gene for IL-1β is located at position 2q13-2q21 [4]. IL-1β acts as a pro-inflammatory cytokine, and it is mainly produced by activated monocytes and macrophages [5]. In the development of breast cancer, IL-1β upregulates cyclooxygenase-2, increases vascular endothelial growth factor expression in tumor cells, and participates in angiogenesis caused by chronic inflammation [6]. Furthermore, IL-1 β induces breast cancer cell proliferation by increasing aromatase activity that converts androgens to estrogen and by increasing steroid sulfatase activity, which converts conjugate estrogens to free-acting estrogens. Moreover, leptin and IL-1β, which are pro-inflammatory adipocytokines, also have direct effect on breast epithelial cells to increase aromatase production and promote tumor growth, migration, and invasion through growth factors [7]. In breast cancer, a critical role of IL-1β was established in previous studies [8910]. These studies indicate that IL-1β expression may combine with estrogen receptor-alpha to affect transcriptional regulation of breast cancer cells [8], which is significant in regulating protumorigenic events within the human breast tumor microenvironment [9], thereby increasing tumor aggressiveness [10].
Single nucleotide polymorphisms in genes encoding cytokines alter the binding affinity of cytokines to transcription factors and consequently change the level and functional activities of secreted cytokines. Three polymorphisms, including IL-1β-511 C > T (rs16944), IL-1β-1464 G > C (rs1143623), and IL-1β-31 C > T (rs1143627), have been identified in the promoter region of IL-1 gene. The IL-1β-511 C > T polymorphism has been related with the promoter activity, and with increased risk of diseases such as cervical cancer [11] and gastric cancer [12]. Many epidemiologic studies have been focused on finding the relationships between IL-1β-G-1464C polymorphism and various diseases such as renal cell carcinoma [13], type 2 diabetes mellitus [14], and non-small cell lung cancer [15]. The association of IL-1β-C31T polymorphism and cancer has been studied in several cancers including non-small cell lung [16], hepatocellular carcinoma [17], and osteosarcoma [18]. Furthermore, many previous studies have been conducted to investigate the association between IL-1β-C31T polymorphism and breast cancer risk in women. However, the data from these studies are not consistent [19202122]. To the best of our knowledge, there is only 1 study investigating the association of IL-1β-C31T polymorphism with breast cancer in the Turkish population (126 cases and 110 controls) [20]. Therefore, in the present study, we sought to investigate whether IL-1β-C31T polymorphism was related to the risk of breast cancer and whether there was a relationship between this polymorphism and demographic factors in the Turkish population.
METHODS
Study population
The study involved 204 women, between 26–76 years old who had confirmed histopathological and immunohistochemical diagnosis of primary breast carcinoma at the pathology Department of the Medical Faculty of Mersin University. Tumor types were retrieved from the pathology reports of these cases in the automation database. The controls consisted of 210 women ranging from 33–79 years old and 11.9% of the controls had a family history of breast cancer. They were selected from the population residing in the same region. Ethical Approval for the research study was obtained from the Ethical Committee of the Medical Faculty of Mersin University (IRB No. 11/08). All women provided an informed consent for this study. Information was collected based on a variety of factors, including family history of breast cancer, reproductive and menstrual history, age, and smoking status. Body mass index (BMI) for individuals participating in this study was calculated using the following formula: weight (kg)/height2(m2). In this study, we included breast cancer patients that were diagnosed following histopathological and immunohistochemical examinations. Therefore, patients that had other malignant tumor histories than breast cancer, undefined diagnosis, and male breast cancer patients were excluded from the study.
IL-1β-C31T genotyping
The peripheral blood samples from women were transferred into an ethylenediaminetetraacetic acid tube, and DNA was extracted from the 414 blood samples using the phenol-chloroform method. All specimens were stored at −20°C until subsequent analysis. To determine the IL-1β-31 polymorphism, polymerase chain reaction (PCR) method was used with forward primer: 5′-AGA AGC TTC CAC CAA TAC T-3′ and reverse primer: 5′-TAG CAC CTA GTT GTA AGG A-3′ [20]. The 23 µL PCR mixture contained about 50 pmol of each primer (forward and reverse), 30 ng of DNA, 125 mM of deoxynucleotide triphosphates, 500 U of Taq DNA polymerase (MBI Fermentas, Vilnius, Lithuania), 20 mM PCR buffer of (NH4)2SO4, and 2.5mM of MgCl. The PCR amplification consisted of an initial melting step of 5 minutes at 94°C; followed by 25 cycles for 1 minute at 94°C, 1 minute at 54°C and 1 minute at 72°C, and a final elongation step for 5 minutes at 72°C [23]. The 240 bp PCR products were cut with AluI restriction enzyme (MBI Fermentas) by overnight incubation at 37°C, and electrophoresed in 3.0% agarose gel stained with ethidium bromide. The IL-1β T-31C was digested into 3 expected results: CC genotype showing 1 band with 240 bp, TT genotype showing 2 bands with 138 bp and 103 bp, CT genotype showing 3 bands with 240 bp, 138 bp, and 103 bp. For quality control, the analyses on a random 10% of the samples were repeated to assess the reproducibility of results.
Statistical analysis
All calculations were performed using SPSS version 22 (IBM Corp., Armonk, USA). Student's t-test was used for comparison of numerical variables. The χ2 test was used for categorical variables. Analyses were performed for breast cancer risk factors such as age (years), BMI (< 25, ≥ 25 kg/m2), smoking status (never/ever), menopausal status (premenopausal and postmenopausal), and age at first pregnancy (< 20, ≥ 20 years of age). Hardy–Weinberg equilibrium attained by the χ2 test was used to evaluate the genetic distributions of participants. Furthermore, multivariate binary logistic regression analysis was performed to adjust the impact of the significant demographic characteristic of breast cancer while investigating the relationship between breast cancer and the IL-1β-C31T polymorphism. p-value < 0.05 is accepted as statistically significant.
RESULTS
The selected demographic characteristics of subjects are shown in Table 1. There was no statistical difference in average of participants' age, age at first birth, age at menarche, or smoking status between control and case groups (p > 0.05). However, significant differences in BMI (p = 0.001), family history (p = 0.031), and age at menopause (p = 0.001) were detected between the studied groups.
Table 1
The demographic characteristics of breast cancer cases and controls
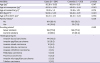
Data are shown as mean ± standard deviation or number (%).
BMI = body mass index.
*Student t-test; †The χ2 test.
![]()
Allele frequencies between breast cancer cases and control groups were compared through χ2 test. The T allele frequency of IL-1β-31 gene increased in the breast cancer group versus control group (56.1% vs. 47.9%; odds ratio [OR]; 1.39; 95% confidence interval [CI], 1.06–1.83; p = 0.017). Additionally, multivariate binary logistic regression analysis showed statistically significant differences in genotype distributions between the breast cancer and control groups. Among the cases, the prevalence of CC, CT, and TT genotypes were 22.1%, 43.6%, and 34.3%, while they were 24.3%, 55.7%, and 20.0% among the controls, respectively. The associations of IL-1β-C31T polymorphism with breast cancer risk were examined with stratification by body-mass index and family history. Compared with IL-1β-31 CC wild-type genotype, a significant increased risk was associated with TT homozygous variant genotype (adjusted OR, 2.06; 95% CI, 1.16–3.66; p = 0.014), but it was not related with CT heterozygous genotype (OR, 0.88; 95% CI, 0.53–1.46; p = 0.862) (Table 2). We did not observe a deviation from Hardy–Weinberg equilibrium in the breast cancer or the control group. We found that the frequency of IL-1β-31 CC genotype in Hardy–Weinberg equilibrium in case group was χ2 = 35.23 (p = 0.100) while in the control group, it was χ2 = 47.91 (p = 0.090).
Table 2
Comparison of the allele and genotype frequencies of IL-1β-C31T in breast cancer cases and controls
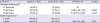
OR = odds ratio; CI = confidence interval.
*Multivariate binary logistic regression analysis; †The χ2 test; ‡Adjusted for body-mass index and family history.
![]()
We analyzed the genotype distribution of IL-1β-31 according to major breast cancer risk factors using the χ2 test (Table 3). The TT genotype showed a 2.19-fold of increased breast cancer risk for obese women (BMI ≥ 25 kg/m2). Among women with late age at first birth, the TT genotype was associated with an increased breast cancer risk (OR, 2.43; 95% CI, 1.29–4.56) compared to CT and the CC genotype. Postmenopausal women with the TT genotype had a greater risk for breast cancer than those with CT and CC genotypes (OR, 3.15; 95% CI, 1.39–7.16). Never-smoking women with TT genotype had increased breast cancer risk compared to the current smoker (OR, 2.52; 95% CI, 1.32–4.82). However, in breast cancer subjects, the TT genotype was not associated with age factor.
Table 3
OR values (95% CI) for breast cancer based on major risk factors and distribution of IL-1β-C31T genotypes (case/control)

OR = odds ratio; CI = confidence interval; BMI = body mass index; OR = odds ratio; CI = confidence interval.
*The χ2 test.
![]()
Genotype distribution in relation to pathological types of breast cancer is shown in Table 4. In the χ2 test, combined CT/TT genotypes were associated with a significantly increased risk of breast cancer in women with invasive ductal carcinoma (OR, 2.82; 95% CI, 1.38–5.76; p = 0.004) when compared to the CC genotype.
Table 4
Genotype distribution in relation to pathological types of breast cancer

![]()
DISCUSSION
In the current study, we evaluated the possible influence of IL-1β-C31T polymorphism within the promoter region of the IL-1 gene, on the susceptibility of breast cancer. We also investigated whether major risk factors play a role in breast cancer development.
Allele frequency often varies substantially across population groups. Akisik and Dalay [20] found the frequency of T allele to be 55.4%, while we detected it as 47.9% in the Turkish population. Interestingly, the frequency of T allele in our control group is similar to that found in the Asian population from Korea (0.509) [24]. In the study of Liu et al. [22], T allele frequency was found as 0.541 in Asian population from China, which was similar to that reported in a Turkish population [20]. Previously, T allele frequency for this polymorphism in Asian population from Japan was reported to be 0.849 [19], which is significantly higher than that in other Asian populations including Chinese [22] and Koreans [24]. As given above, the distribution of genotype frequencies for IL-1β-C31T polymorphism is different in individuals from different geographical regions. These differences in genotype distribution in various studies may be due to the small sample size.
The inflammasome is a multiprotein oligomer that activates pro-inflammatory cytokines including IL-18 and IL-1β [25]. IL-1β could enhance the production of chemokines, adhesion molecules, and prostaglandin. The increased expression may initiate an inflammatory cascade, such as cell chemotaxis, angiogenesis, and adhesiveness, which then cause cancer-associated inflammation [26]. Several studies have been conducted based on this close association between IL-1β levels and invasiveness, aggressiveness, and high tumor grade of breast cancer [272829]. A study showed that IL-1β was present in 90% of invasive breast carcinomas, and it was suggested that elevated levels of IL-1β were associated with tumor invasiveness and tumor aggressiveness [10]. Another study indicated that grade III tumors had higher IL-1β expression levels compared to grade I and II tumors, and macrophage inflammatory protein-1β was found to be associated with inflammation [28]. Kurtzman et al. [29] demonstrated that IL-1β accumulated in tumor microenvironment, which might play an important role in regulating the growth and progression of breast tumor. IL-1β found together with estrogen receptor-α was detected to increase gene expression with an estrogen responsive element in breast cancer cells [8].
To date, many epidemiological studies have evaluated the polymorphism of the IL-1β gene with the risk of cancer such as cervical [11], gastric [12], and non-small cell lung cancer [15]. Several studies have focused on the association between the IL-1β-C31T polymorphism and breast cancer risk. However, the findings of earlier studies are conflicting. Ito et al. [19] showed the protective role of TT genotype (IL-1β-C31T rs1143627) against breast cancer onset in Japanese population (age-adjusted OR, 0.58; 95% CI, 0.32–1.02). A meta-analysis conducted in 2010, which included 8 case-control studies, concluded that CC genotype was associated with 1.37-fold increase in breast cancer risk [21]. Furthermore, Liu et al. [22] observed a positive relationship between IL-1β-31CC genotype and breast cancer risk (adjusted OR, 1.72; 95% CI, 1.16–2.54). However, we observed a stronger relationship between the IL-1β-31TT genotype and breast cancer risk (adjusted OR, 2.06; 95% CI, 1.16–3.66; p = 0.014). Two studies on the contrary, found that there was no difference in the distribution of genotypes between breast cancer cases and controls [2024].
Previous studies have identified the risk factors that increase breast cancer risk. Major risk factors comprise age, age at first birth, menopausal status, BMI, and smoking status. Liu et al. [22] found 1.74-fold (95% CI, 1.13–2.67) increased risk of breast cancer in older women with CT/CC genotypes; however, our findings did not show any correlation between TT genotype and late age. In this study, we found an association between breast cancer risk and TT genotype among women with late age at first birth. In contrast, Liu et al. [22] did not observed association between IL-1β-31TC/CC genotypes and early age first birth. In this study, TT genotype was associated with increased breast cancer risk in postmenopausal women. However, a case-control study showed that IL-1β-31CT/CC variant genotypes were associated with increased breast cancer risk in postmenopausal Chinese women (adjusted OR, 1.56; 95% CI, 1.00–2.42) [22]. However, in subgroup analyses of menopausal status, IL-1β-31CT/CC variant genotypes showed a preventive effect among postmenopausal women [19]. On the contrary, another study showed no significant modification of ORs for CC genotype by menopausal status [24]. In the current study, women who have TT genotype with BMI ≥ 25 kg/m2 had a statistically significant 2.19-fold increased risk for developing breast cancer. Ito et al. [19] did not demonstrate any significant association between TT genotype and BMI ≥ 22 kg/m2 in Japanese case-control study. We also detected that never smokers having TT genotype had an elevated risk of breast cancer. This may be because the smoking affected the metabolism of estradiol, leading to enhanced formation of the inactive catechol estrogens [30]. Moreover, for IL-1β-31CT/TT variant genotype carriers, we observed a 2.82-fold increase in breast cancer risk associated with women diagnosed with invasive ductal carcinoma. To the best of our knowledge, our study is the first to evaluate the relationship between the genotypes of IL-1β-C31T polymorphism and pathologic types of breast cancer.
In conclusion, we observed that a significantly increased risk of breast cancer was associated with IL-1β-C31T polymorphism. Furthermore, we found that IL-1β-C31T polymorphism might contribute to the development of breast cancer in women with: BMI ≥ 25 kg/m2, late age at first birth, postmenopausal status, negative smoking history, and invasive ductal carcinoma. In future studies, these findings may elucidate the potential role of IL-1β gene product, known as an inflammatory cytokine, in breast cancer development. However, genetic polymorphisms may vary among different ethnic groups and further studies including larger sample sizes of different ethnic groups are required to examine the association between IL-1β-C31T polymorphism and breast cancer.
 XML Download
XML Download