

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) is a small-vessel vasculitis characterized by the presence of ANCA and typical involvement of kidney and respiratory tract.1 D-penicillamine is one of the drugs that can induce drug-induced AAV.2 Rapidly progressive glomerulonephritis (RPGN) and pulmonary-renal syndrome (PRS) are primary manifestations of D-penicillamine-induced AAV.34567891011121314151617181920 Because most of them develop in adults, we could search only two cases of D-penicillamine-induced AAV diagnosed at age younger than 18 years,21 and both cases presented RPGN. Here, we report a case of D-penicillamine-induced AAV that developed in a 13-year-old girl and manifested a PRS without azotemia.
CASE DESCRIPTION
A 13-year-old female patient visited the emergency room for hemoptysis, fever, and dyspnea on September 8, 2017. She has been on D-penicillamine for five years under the diagnosis of Wilson disease with a well-controlled copper level. Urinalysis performed before the administration of D-penicillamine was normal. Since five months before admission, intermittent pain occurred at the ankle, foot, calf, and wrist. Two months prior to admission, urine test revealed microscopic hematuria (10-19 RBCs/HPF) and mild proteinuria (1+). Two weeks before admission, cough and fever developed followed by dyspnea and hemoptysis for a week before admission. She had no family history of autoimmune disease or Wilson disease.
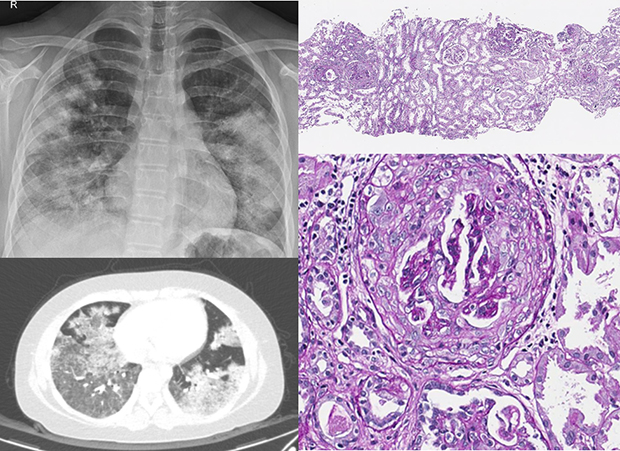
At admission, blood pressure was 132/74 mmHg, the temperature was 36.5°C, pulse rate was 132/min, and respiratory rate was 24/min. Crackle sounds were heard at both lower lung fields, and heartbeats were regular without a murmur. Hemoglobin was 8.7 g/dL, reticulocyte count 2.5%, the white blood cell count was 9,670/µL, and platelet count was 344,000/µL. Serum hepatic enzymes were normal, and albumin level was 3.7 g/dL. Blood urea nitrogen and serum creatinine were 12 mg/dL and 0.62 mg/dL respectively and estimated GFR was 109.8 mL/min/1.73 m2. C-reactive protein level was 9.1 mg/dL, and erythrocyte sedimentation rate was 28 mm/hr. The patient had microscopic hematuria (5-9 RBCs/HPF) and proteinuria (urine protein creatinine ratio 1.05 mg/mg). Anti-myeloperoxidase (MPO) IgG titer was over 600 U/mL (reference < 20 U/mL) while anti-proteinase 3 (PR3) IgG titer was within normal limit. Complement levels were normal and antinuclear antibody, anti-double-stranded DNA antibody, rheumatoid factor, anti-cardiolipin antibody, anti-glomerular basement membrane antibody were all negative. There was no evidence of infection or hemolysis. Chest radiography and computed tomography suggested diffuse pulmonary hemorrhage (Fig. 1). The echocardiographic findings were not remarkable. Renal Doppler ultrasonography revealed normal size and shape of both kidneys and an equivocal increase in cortical echogenicity.
 | Fig. 1Chest radiologic findings of the patient. (A) Bilateral extensive patchy consolidation at the plain film and (B) the multifocal patchy ground-glass opacity at chest computed tomography suggest diffuse pulmonary hemorrhage.
|
Under the tentative diagnosis of D-penicillamine-induced AAV, trientine was substituted for D-penicillamine. Because the patient's respiratory symptom aggravated, she was transferred to ICU and supported by a ventilator. Plasma exchange was performed for 3 days daily and methylprednisolone (1 g per day) was given intravenously for 3 days followed by the administration of IgG (0.7 g/kg) for 3 days.
A renal biopsy disclosed cellular and fibrocellular crescents in 39% (16/41) of the glomeruli. Glomerular size and mesangial cellularity were mildly increased. Immunofluorescent and electron microscopic findings were not noteworthy except focal effacement of the foot processes. These findings were compatible with the pauci-immune crescentic glomerulonephritis (Fig. 2).
 | Fig. 2Photomicrograph of the kidney biopsy. (A) Crescent formation is observed in 39% of the total 41 glomeruli by the light microscopy (PAS, ×40). (B) A representative crescent (arrow) is shown at a high power magnification (PAS, ×400).PAS = periodic acid–Schiff.
|
After confirming the renal pathology, intravenous cyclophosphamide (750 mg/m2) was administered, followed by administration of oral glucocorticoids (prednisolone 60 mg/day) and mycophenolate mofetil (1,500 mg/day). Acute phase reactants dropped a few days later with the rapid improvement of the respiratory failure. Proteinuria and microscopic hematuria disappeared five months later. MPO-ANCA titer decreased more gradually and still positive in a low titer (8.1 IU/mL) at 17 months after the withdrawal of D-penicillamine.
DISCUSSION
AAV is an autoimmune small-vessel vasculitis characterized by ANCA, an autoantibody specific for neutrophil granule components, MPO or protease 3 (PR3).1 Drugs such as propylthiouracil, hydralazine, penicillamine, allopurinol, sulfasalazine, and levamisole have been described to induce AAV, the majority with MPO-AAV.22 D-penicillamine-induced AAV is reported to affect kidneys with or without concurrent involvement of the respiratory tract, therefore, leads to either RPGN345678910112021 or PRS.1213141516171819
PRS describes a syndrome of respiratory failure in association with renal failure or a diffuse alveolar hemorrhage complicating acute glomerulonephritis.23 PRS often results in severe life-threatening systemic disease requiring urgent aggressive therapy and renal and lung biopsy reveals histological features of the glomerular crescents and pulmonary capillaritis.24 Serum creatinine is usually elevated in PRS, but it may not always be elevated.23 Among the 11 cases of penicillamine-associated PRS reported with the serum creatinine available, there was an adult woman who had normal serum creatinine.25 Our case also showed microscopic hematuria and proteinuria with normal renal function while renal biopsy revealed cellular or fibrocellular crescents in 39% of the glomeruli. McAdoo et al.26 analyzed 258 cases of necrotizing or crescentic glomerulonephritis and found that 14.7% of the patients represent preserved renal function. This silent crescentic glomerulonephritis with normal renal function is more likely to be identified in PRS because pulmonary manifestations facilitate earlier biopsy and diagnosis of the glomerulonephritis before renal function deteriorates. In our case, if the renal biopsy was performed later and the treatment was delayed, azotemia might have developed.
Most of the reported AAV patients were adults. Only two cases of D-penicillamine-induced AAV are reported at the age younger than 18 years, and both pediatric cases presented as RPGN.21 Therefore, to the best of our knowledge, this is the first pediatric case of D-penicillamine-induced AAV that manifests a PRS.
Loss of tolerance and development of autoimmunity to MPO and PR3 is the first step in the development of AAV. Mechanism of losing tolerance is unclear, though dysregulation of the adaptive immune response, neutrophil extracellular trap (NET), ANCA antigen on the surface of apoptotic neutrophil, and functional abnormality in regulatory T cell are implicated.1 Subsequently, T-cell helped activation of autoreactive B-cell produces ANCA. Finally, ANCA induces activation of circulating neutrophils that localize to vascular beds, degranulate and release NET resulting in endothelial injury.127
How individual drug triggers the AAV is not well understood. Because the molecular weight of most drugs is low, the formation of a bigger complex is required to provoke immune response.28 In animal experiments, penicillamine is reported to activate macrophages through binding to aldehyde-containing molecules and production of TNF-α, IL-6, and IL-23,2930 giving rise to induction of autoimmunity. Though mechanistic studies about penicillamine induced AAV is not sufficient, it can be compensated by investigations performed for other drug-induced AAVs, because the clinical manifestations are very similar.28 Propylthiouracil, another causative drug of AAV, is reported to be oxidized in the presence of activated neutrophils forming reactive drug metabolites that stimulate ANCA production.31 It was also reported that propylthiouracil induces abnormal conformation and impaired degradation of NET leading to the development of autoimmunity.32 In hydralazine-associated AAV, neutrophil apoptosis in response to hydralazine MPO binding is hypothesized to result in the production of autoantibodies.33
The prevalence of ANA in drug-associated AAV has been reported to vary from 17% to 80%. It was reported that the prevalence is higher in AAV induced by hydralazine and lower in the vasculitis associated with propylthiouracil.22 In authors review of the literature, ANA was present in 76% of the 17 reported cases of the D-penicillamine-induced AAV. Clinical significance of the ANA positivity in drug-induced AAV remains to be elucidated.
Because the diagnosis of drug-induced vasculitis is complicated by a variety of factors such as the dose and duration of medication, and frequency of diagnostic laboratory studies according to the physician's awareness of the disease, involved organs and clinical presentations may be diverse. Therefore, treatment should depend on the severity of clinical manifestations.28 The first step is to discontinue the offending agent. For those with active and significant organ involvement, additional immune suppression by glucocorticoid is necessary. For severe organ failure associated with alveolar hemorrhage or RPGN, cyclophosphamide or other immunosuppressants such as mycophenolate mofetil or rituximab may be added. Intravenous pulse methylprednisolone and plasmapheresis can be used in life-threatening cases. Supportive care would include ventilatory support and renal replacement for severe PRS.34
Delayed diagnosis of drug-induced AAV may cause serious results. Therefore, it is preferable to avoid long-term use of AAV inducible medications such as propylthiouracil, hydralazine, penicillamine, allopurinol, sulfasalazine, and levamisole. When long-term use of these drugs is inevitable, it is desirable to monitor respiratory symptoms and signs, and urinalysis closely, and when suspected, check ANCA titer and chest radiography. However, it should be emphasized that though positive seroconversion of ANCA is a clue to the diagnosis of drug-induced AAV, positive ANCA titer only is not sufficient to diagnose the drug-induced AAV and begin treatment, because only a small proportion of the patients with positive ANCA develop clinical vasculitis.28
In this case, crescentic glomerulonephritis was found in the renal biopsy despite the mild renal manifestations and completely normal renal function. Therefore, when urinary abnormalities are found in a patient with suspected AAV and pulmonary hemorrhage, even if the renal function is normal, renal biopsy is highly recommended.
Although anti-MPO antibody titer decreased steadily from over 600 to 8.1 IU/mL, the value was still above the normal range at 17 months after the withdrawal of D-penicillamine. This long-lasting ANCA activity is consistent with the finding in propylthiouracil (PTU)-induced AAV that anti-MPO titer was within the reference range only in six of the thirteen patients at a median follow-up of 38 months after discontinuation of PTU.35 Therefore, drug-induced ANCA seems to last for a substantial period after withdrawal of the triggering agent.
 XML Download
XML Download