

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
In cancer treatment, adequate surgical resection, including lymph node dissection (LND), is essential to achieve a curative state. In advanced gastric cancer (AGC), total or subtotal gastrectomy with D2 LND is widely performed as the standard treatment [123]. Since proximal gastric cancer, which has a steadily rising incidence [4], metastasizes to the splenic hilar lymph nodes (LNs; station No. 10) in 9%–26% [5678], D2 LND, including splenic hilar LND, is recommended for proximal AGC as per previous treatment guidelines [9].
To remove splenic hilar LNs, surgeons should perform splenectomy or spleen-preserving hilar LND. The theoretical background for the removal of splenic hilar LNs in AGC has been explored using lymphangiography [10]. With evidence of lymphatic flow from the upper greater curvature through the splenic hilum to the celiac trunk, splenectomy has been considered as an effective method for performing en-bloc resection of gastric cancer and adjacent LNs [10]. However, because of compromised immunological functions along with high morbidity and mortality rates, splenectomy poses serious adverse effects [111213]. Meanwhile, because surgical techniques have improved, some experienced surgeons perform spleen-preserving hilar LND, which could be an ideal method [1415]. Nevertheless, although this procedure is theoretically rational, it is technically challenging, and the oncological validity of the procedure remains unclear [14]. Thus, splenectomy and spleen-preserving hilar dissection should be avoided, if possible, because of the difficulty in the procedure and other aspects.
In previous Japanese guidelines, the decision of performing hilar LND was based on clinical T classification of cancer (T2 or more advanced lesion). However, the recently revised guidelines do not include splenic hilar LND for all proximal advanced cancers unless it involves the greater curvature of the stomach. However, even among the indicated patients, there may be patients who would gain little benefit or even detrimental effects from hilar dissection. Identifying the characteristics of this group of patients could be useful to prevent unnecessary hilar dissection.
In the present study, we presumed that pT2-4aN0 patients would not gain any additional oncological benefits from hilar dissection. Accordingly, we aimed to determine the survival impact of splenectomy or splenic hilar dissection in the proximal AGC patients without LN metastasis who underwent curative total gastrectomy. We also sought to investigate whether D2 LND, including splenectomy and spleen-preserving hilar dissection, should be mandatory for LN negative proximal AGC.
MATERIALS AND METHODS
Patients
By retrospectively analyzing our prospectively collected database from the Department of Surgery, Yonsei University College of Medicine from 2000 to 2010, we identified 2,453 patients who underwent total gastrectomy for gastric cancer. Of these, 2,083 patients were excluded (87 patients were diagnosed with other malignancies before the operation and 92 patients were treated with preoperative chemotherapy or radiotherapy). A total of 231 patients underwent non-curative surgery, among whom 120 had peritoneal seeding; 81 had positive washing cytology or other organ metastasis, including para-aortic LN metastasis; and 30 were not treated with R0 resection. Among the remaining patients, 400 met the pathological T2-4aN0 criteria, among whom 30 patients having incomplete clinicopathological information were excluded. Finally, 370 patients were included in the analysis (Fig. 1). The clinicopathological characteristics (age, sex, histological differentiation, tumor location, gross type, size, and T classification) of the 370 patients were analyzed. This retrospective study was approved by the Institutional Review Board (IRB) of Severance Hospital Yonsei University College of Medicine (4-2017-0711). Because of the retrospective nature of the study, signed patient informed consent was waived as per the IRB approval.

Operation
Curative total gastrectomy with LND was performed following the Japanese Gastric Cancer Association (JGCA) classification guidelines [9]. A total of 370 patients underwent total gastrectomy with LND by open, laparoscopic, or robot-assisted methods for gastric cancer. The patients who met the indications of minimally invasive surgery at our institution were able to select the surgical procedure after receiving information on the advantages and disadvantages of each procedure.
Survival impact of splenectomy on node negative T2-4a gastric cancer patients
For the current study, we divided the patients into 3 groups: splenectomy group, spleen-preserving hilar LND group (SPHLD group), and a group of patients in whom the extent of LND was not up to D2 dissection (D1+). To verify the survival impact of splenectomy on patients with proximal AGC, the splenectomy group was compared with the other 2 non-splenectomy groups (SPHLND+D1+) in terms of clinicopathological characteristics and long-term survival. Because the surgical treatment method or extent was pre-determined based on clinicopathological characteristics, we expected the study groups to show significant differences in perioperative outcomes, which we corrected using propensity score matching analysis. Accordingly, the long-term outcomes were compared by assessing overall and relapse-free survival among the groups before and after propensity score matching.
Survival impact of D2 LND on node negative T2-4a gastric cancer patients
In addition, the splenectomy plus SPHLD groups, which underwent D2 LND, were compared with the D1+ group to verify the oncological impact of D2 LND on node-negative T2-4a gastric cancer patients. In the same way, the clinicopathological characteristics and long-term outcomes were analyzed for the D2 group and compared with the D1+ group.
Statistical analyses
The clinicopathological and long-term oncological results, including overall and relapse-free survival, were analyzed using the R package survival and Matchit (version 3.3.1). To minimize selection bias, seven perioperative variables representative of patient features (age and sex) and tumor characteristics (histological type, location, gross type, size, and T classification) were selected and matched 1:1 using propensity score matching, as these variables are considered to have a significant impact on patient survival. The patients were followed from the date of operation until December 31, 2014, or their death. Overall survival was defined from the date of operation to the last follow-up or death from any cause. Relapse-free survival was defined from the date of operation to recurrence of gastric cancer or death from any cause. The patients were censored at the last follow-up if they did not experience the designated events. The overall and relapse-free survival were assessed using the Kaplan-Meier method, and the differences in survival curves among the groups were examined using the log-rank test. The categorical and continuous variables were analyzed by the χ2 or Fisher's exact and Student's t-test, respectively. All P-values <0.05 (2-sided) were considered statistically significant. Multivariate analyses to assess the risk factors for overall survival were performed using the Cox proportional hazard model. The following variables were included in the analyses: age, sex, location, differentiation, Borrmann type, tumor size, and type of operation.
RESULTS
Demographic characteristics of the patients among the different groups and comparison of long-term survival
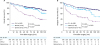
Among the 370 patients who underwent total gastrectomy for pT2-4aN0 proximal AGC, 43 patients underwent splenectomy, and 79 patients underwent spleen-preserving hilar LND. The remaining 248 patients underwent surgery with limited LND, excluding station No. 10. The splenectomy group tended to have more advanced disease (Table 1). In the comparison of survival curves among the splenectomy, SPHLD, and D1+ groups, the splenectomy group had worse overall survival than the other 2 groups (P<0.001 for D1+, P=0.003 for SPHLD). Relapse-free survival was also worse in the splenectomy group than the other two groups (P<0.001 for D1+, P=0.003 for SPHLD). There were no differences in the overall and relapse-free survival between the SPHLD and D1+ groups (P=0.239 and P=0.061, respectively; Fig. 2).
Table 1
Demographics of patients in the splenectomy, SPHLD, and D1+ groups
Comparison of the characteristics before and after propensity score matching between the splenectomy and non-splenectomy groups
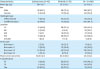
To investigate the impact of splenectomy on pT2-4aN0 patients, the two non-splenectomy groups were combined and compared with the splenectomy group (splenectomy group [n=43] vs. non-splenectomy group [n=327, SPHLD+D1+]) (Table 2). In this comparison, a few clinicopathological characteristics were found to be significantly different between the 2 groups: The mean tumor size of the splenectomy group was 60.6 mm, whereas that in the non-splenectomy group was 44.0 mm (P<0.001). Furthermore, compared with the non-splenectomy group, the splenectomy group had an advanced T classification (P<0.001). After 1:1 propensity score matching for seven variables, 39 pairs of patients with similar clinicopathological characteristics, including age, sex, histological type, location, gross type, size, and T classification, were matched (P>0.05).
Table 2
Demographics of patients before and after propensity score matching between the splenectomy and non-splenectomy (SPHLD+D1+) groups

Comparison of long-term outcomes between the splenectomy and non-splenectomy groups
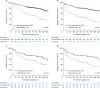
Comparing the survival curves, worse overall and relapse-free survival were observed in the splenectomy group (n=43) than in the non-splenectomy group (n=327) (P<0.001 and P<0.001, respectively) (Fig. 3A and B). After propensity score matching, a comparison of 39 matched pairs showed similar overall survival but worse relapse-free survival in the splenectomy group (P=0.123 and P=0.021, respectively) compared with those in the non-splenectomy group (Fig. 3C and D).
Fig. 3
Kaplan-Meier overall and relapse-free survival curves for patients with splenectomy compared with those for patients with non-splenectomy (SPHLD+D1+) before and after propensity score matching. (A) Overall survival before matching (P<0.001). (B) Relapse-free survival before matching (P<0.001). (C) Overall survival after matching (P=0.123). (D) Relapse-free survival after matching (P=0.021).
SPHLD = spleen-preserving hilar lymph node dissection.
Comparison of the characteristics before and after propensity score matching between the D2 and the D1+ groups
To investigate the impact of D2 LND, the D2 group (n=122, splenectomy+SPHLD) was compared with the D1+ group (n=248) (Table 3). More advanced disease (larger tumor size and higher T classification) was observed in the D2 group than in the D1+ group (P=0.011 and P=0.011, respectively). After 1:1 propensity score matching with the same seven variables, 107 pairs of patients with similar clinicopathological features were matched (P>0.05).
Table 3
Demographics of patients before and after propensity score matching between D2 dissection (splenectomy+SPHLD) and D1+ groups

Comparison of long-term outcomes between the D2 and the D1+ groups
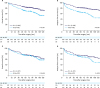
When comparing the survival curves between the D2 and the D1+ groups before propensity score matching, the D2 group had worse overall and relapse-free survival than the D1+ group (P=0.001 and P<0.001, respectively) (Fig. 4A and B). After propensity score matching, comparison of the 107 matched pairs revealed similar overall and relapse-free survival between the 2 groups (P= 0.619 and P=0.112, respectively) (Fig. 4C and D).
Fig. 4
Kaplan-Meier overall and relapse-free survival curves for patients with D2 LN dissection (splenectomy+SPHLD) compared with those for patients with D1+ before and after propensity score matching. (A) Overall survival before matching (P=0.001). (B) Relapse-free survival before matching (P<0.001). (C) Overall survival after matching (P=0.619). (D) Relapse-free survival after matching (P=0.112).
SPHLD = spleen-preserving hilar lymph node dissection.
Recurrence patterns
During the median follow-up period of 93.3 months, 52 of 370 patients (13, 7, and 32 patients in the splenectomy, SPHLD, and D1+ groups, respectively) were found to have a recurrence. Among them, spleen or splenic hilar LN recurrence was found in 3 (1.2%) patients. The first patient (54-year-old male) had T4aN0 cancer located on the lesser curvature and underwent D1+ LND. He experienced a recurrence in the splenic hilar and the paraaortic LNs at 36 months after the primary operation. The second patient (64-year-old male) had T2N0 cancer located on the posterior wall and underwent D1+ LND. He had recurrence at the splenic hilar and the paraaortic LNs at 39 months after the operation. These patients were treated with palliative chemotherapy after diagnosis of recurrence but died within 6 and 18 months. The third patient (40-year-old male) underwent D1+ LND for cancer (pT3N0) located at the greater curvature. He had recurrence only at the splenic hilum. Splenectomy was followed, and 12 metastatic LNs were found among 14 dissected LNs. This patient was followed up and remained disease-free for more than 6 years.
Cox proportional hazard model for multivariate analysis
In a multivariate analysis to identify risk factors for overall survival using Cox proportional hazard model, hazard ratios (HRs) of the SPHLD group and D1+ group were 0.49 (95% confidence interval [CI], 0.26–0.91; P=0.023) and 0.41 (95% CI, 0.24–0.68; P<0.001), respectively, compared with those of the splenectomy group (Supplementary Fig. 1).
DISCUSSION
In this study, we found that prior to propensity score matching, patients with splenectomy tended to have tumors of larger size and more advanced T classification than patients who did not undergo splenectomy. Thus, we performed a propensity score matching to correct the differences in clinicopathological characteristics due to selection bias that could skew oncological results. After propensity score matching, we noted no difference in the clinicopathological characteristics between patients who underwent splenectomy and those who did not. Similar results were obtained with patients who underwent D2 LND compared with those who underwent D1+ dissection. Survival curves after propensity score matching suggested that neither splenectomy nor D2 LND had a positive impact on long-term survival in patients with LN-negative T2-4a AGC.
The controversy surrounding the benefits of splenectomy to oncological outcomes in gastric cancer regardless of LN involvement has been longstanding. Previous reports have shown that splenectomy offers no survival benefit in the presence of metastatic LN [816]. Meanwhile, the recently published JCOG0110 trial, which compared splenectomy group with a non-splenectomy group for clinical AGC (cT2-4/N0-2) not invading the greater curvature, concluded that splenectomy was not superior to spleen preservation [1718]. However, a recent report from our institution demonstrated that splenic hilar LND during splenectomy or with spleen preservation had a positive impact on long-term survival similar to that with the removal of other extra-perigastric LN groups [19]. Watanabe et al. [20] also reported from a single institutional data that splenectomy offers a survival benefit when cancer involves the greater curvature. In this study, the LN positive ratio was 68.2% in cancers involving the greater curvature [20]. Additionally, Ji et al. [21] recently reported that spleen-preserving hilar dissection elicited better survival than splenectomy for upper and middle third AGC. Thus, dissecting hilar LNs and preserving the spleen could be desirable in certain patients with proximal AGC. In the current study, we focused on patients who could be exempted from splenectomy or splenic hilar dissection although they had advanced diseases. Thereby, we were able to analyze the impacts of splenectomy and D2 LND in patients with an advanced disease without LN metastasis. Our results suggest that the potential hazards posed by these procedures may outweigh their benefits in this specific group of patients.
After the results of JCOG 0110 trial were published, there was a drive to alter the extent of LND in proximal AGC. Because this trial did not include tumors located in the greater curvature, it was considered that tumors on the other side of the proximal stomach could be indicated for limited LND. In this regard, Kinoshita [22] recently suggested 3 different procedures as follows: D2-No. 10, spleen-preserving D2, and splenectomy D2. In addition, according to the latest guidelines revised in 2018, splenic hilar LND is not necessary unless cancer involves the greater curvature of the stomach. However, in the JCOG 0110 trial, N0 cancer accounted for 42.2% (213/505) of all cancers. Thus, there was a possibility of decreased survival in the splenectomy group because of the potential adverse oncological impact of splenectomy on N0 cancer, although in the subgroup analysis of the study, contrary to our expectations, splenectomy in patients with N0 cancer tended to have a positive impact on the survival (HR, 1.23; 95% CI, 0.68–2.25) [17]. In this study, we tried to investigate whether it is possible to identify patients who do not require splenic hilar LND based on tumor factors, including the location. Accordingly, we suggested that patients with T2-4aN0M0 tumors, which are classified as stage IB–IIB based on the 7th Union for International Cancer Control/American Joint Committee on Cancer TNM staging system, could be the ideal candidates for limited LND regardless of tumor location. These patients in our database comprised 28.7% of the patients for whom D2 LND was indicated with a curative aim.
Herein, we showed the survival impact of splenectomy or D2 LND in patients with pT2-4aN0M0 cancer involving a large amount of data using propensity score matching. However, there are some limitations to this study. The critical limitation of our study is that we compared pathological findings. Thus, it would be difficult to apply these results to clinical practice, because the current preoperative diagnosis is limited to predicting pN0 cancer. While computed tomography (CT), endoscopic ultrasound, and positron emission tomography-CT are used for gastric cancer staging before surgery, their sensitivity and specificity are not high enough to confirm nodal involvement [23]. Although Tokunaga et al. [24] showed that clinical findings have an effect on the survival outcomes even among patients with the same pathological findings, we attempted to identify the specific patient group which does not require splenectomy or splenic hilar LND by analyzing the pathological data. Nevertheless, with ongoing research, we expect that the accuracy of the preoperative diagnosis of N classification will improve with time, and our results could be more applicable for the accurate preoperative prediction of N classification. Secondly, our study was performed as a retrospective analysis using data from a single institution. Although the reasons for splenectomy were sometimes unclear, we tried to reduce selection bias by excluding T4b cancer and using propensity score matching. In addition, our data could be considered robust because these were derived from the results of a standardized treatment administered by experienced surgeons from a center with a high volume of patients with gastric cancer. For instance, although the extent of LND did not adhere to the standard treatment guidelines in the D1+ group, more than 40 LNs were retrieved, which was much greater than the 16 LNs required for proper staging (50.7, 46.6, and 42.9 in splenectomy, SPHLD, and D1+ groups, respectively). Furthermore, there was no accurate information on postoperative adjuvant chemotherapy which might have an impact on the survival. However, in general, gastric cancer patients in stage II or higher received our institution's standard 5-fluorouracil-based adjuvant chemotherapy since early 2000. Finally, even after propensity score matching, there were still differences in the clinicopathological characteristics and unseen bias due to latent variables, although we tried to reduce the bias by matching the patients for seven clinically important characteristics known to affect survival after treatment.
In conclusion, we found that splenectomy does not have an oncological benefit in patients with LN-negative AGC. In addition, we deemed D2 LND to be unnecessary for these patients. Although the accuracy of current preoperative nodal classification is not high enough, our results could play an important role in determining and revising the extent of LND for the treatment of proximal AGC.
 XML Download
XML Download