

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Helicobacter pylori (HP) infection on the gastric mucosa leads to mucosal atrophy and metaplasia of the intestinal epithelium and subsequently generates adenocarcinoma [123]. Lauren classified gastric adenocarcinoma into intestinal and diffuse types in 1965, and recent studies revealed the relevance between HP infection and generation of both intestinal-type early gastric cancers (I-EGCs) and diffuse-type early gastric cancers (D-EGCs) [45]. As the opportunity of screening the stomach without HP infection or after successful HP eradication therapy has increased, cases of HP-negative EGCs have been reported. Especially, it was reported that the other type of adenocarcinoma, gastric adenocarcinoma of the fundic gland type (chief cell predominant type) (GA-FG-CCP), was able to generate in the HP-uninfected mucosa, and GA-FG-CCP was newly added as a special type of cancer in the Japanese Classification of Gastric Carcinoma [678].
GA-FG-CCP is characterized as its differentiating potential toward fundic glands in terms of expressing fundic gland markers (pepsinogen I and H+/K+-ATPase) and mimicking a formation of fundic glands [6]. While most GA-FG-CCPs develop slowly and have lower malignant potential than the typical early gastric adenocarcinoma, some cases of GA-FG-CCPs showed lymphatic or venous invasion and lymphatic metastasis [691011]. The endoscopic features of GA-FG-CCP were described as follows: 1) submucosal tumor-like shape, 2) whitish color, 3) dilated vessels with branching architecture, and 4) background mucosa without atrophic change [7]. Especially, of these findings, “background mucosa without atrophic change” directly indicates HP-uninfected status. In contrast, there have been accumulating evidence indicating that residue of fundic gland in the atrophic epithelium is able to generate GA-FG-CCP [712]; thus, the finding of “background mucosa without atrophic change” is believed not to be a specific feature of GA-FG-CCP. Nowadays, successful eradication therapy of HP is easily performed worldwide. As the opportunity of screening the stomach with atrophic change after HP eradication therapy has increased, the number of GA-FG-CCP cases found in the HP-eradicated mucosa has also increased [12]. Nevertheless, so far, characterizing GA-FG-CCPs found in the atrophic epithelium has not been sufficiently discussed in literature. In this study, we compared endoscopic findings and clinicopathological features of GA-FG-CCPs generated in the HP-uninfected mucosa (4 cases) and the atrophic mucosa post HP eradication therapy (4 cases) to elucidate the effect of HP infection on the appearance of GA-FG-CCPs.
MATERIALS AND METHODS
Subjects
A total of 348 cases of gastric cancers that were treated with endoscopic submucosal dissection from August 2014 to August 2018 were retrospectively selected from the registry of endoscopy in Tokyo Medical and Dental University. Only 9 cases (2.6%) of GA-FG-CCP were found in the registry. There was no case of GA-FG-CCP treated with surgical resection in the registry of gastric surgery. Of 9 cases, 1 case was excluded because of a current HP infection. Consequently, the remaining 8 cases of GA-FG-CCPs were classified into 2 groups according to the status of HP infection: HP-uninfected group (4 cases) and HP-eradicated group (4 cases). This study protocol was approved by the ethical committee of our institution (approval number: 1803).
Endoscopic evaluation
All patients underwent conventional white light imaging (WLI) to determine the type of lesions (elevated, flat, or depressed) and were subsequently observed by magnifying endoscopy with narrow band imaging (M-NBI). The location and shape of lesion were classified according to the Japanese Classification of Gastric Carcinoma [1314]. Elevated lesions were described as 0–I type. Flat lesions were classified into 3 types including 0–IIa, 0–IIb, and 0–IIc type according to the degree of difference in height. Depressed lesions were described as 0–III type. The surface structures and vessels observed in the lesions by M-NBI were classified into regular, irregular, or absent pattern according to the vessels plus surface (VS) classification system proposed by Yao et al. [1516]. In addition to the VS classification, we analyzed characteristic tapered microvessels that branched from larger cyanic vessels (collecting venules) at the deeper layer. Endoscopically, we defined tapered microvessels as smaller vessels that are observed in the normal gastric mucosa with uniform and open-looped shape, symmetrical arrangement, and regular distribution, which are classified into “regular microvessels” according to the VS classification system. All patients underwent only 1 biopsy sampling from the lesion preceding the observation by M-NBI.
Status of HP infection
The status of HP infection was confirmed by at least 3 distinct examinations including enzyme immunoassay with specific serum immunoglobulin G (IgG) against HP, urea breath test, and fecal HP antigen test or direct observation of HP on biopsy samples. High titer >3 IU/mL of serum IgG was regarded as positive for current HP infection. In patients in whom HP was previously eradicated, success of eradication therapy was determined by the urea breath test. The extent of atrophic gastritis was described according to the Kimura-Takemoto classification [17].
Pathological examination
Resected samples were fixed by 10% formaldehyde and embedded into paraffin block. Sectioned samples were pathologically diagnosed under hematoxylin and eosin stain (H&E) staining and immunohistochemistry of mucin 2 (MUC2) (Leica, NCL-MUC-2), MUC5AC (Leica, NCL-MUC-5AC), MUC6 (NCL-MUC-6), pepsinogen I (Bio-Rad, 7240-1009), H+/K+-ATPase (MBL, D031-3), p53 (Leica, NCL-L-p53-DO7), and Ki67 (Agilent, M7240). The findings of H&E staining that mainly composed of highly differentiated columnar cells mimicking fundic gland cells, predominantly of chief cells, with pale gray-blue, basophilic cytoplasm and mildly enlarged nuclei were referred for diagnosis. The diagnosis of GA-FG-CCP was further confirmed by the results of mucin histochemistry (positive staining of MUC6 and negative staining of MUC2 and MUC5AC) and the extent of differentiation toward fundic gland cells (diffuse staining of pepsinogen I and scattered staining pattern of H+/K+-ATPase) [6]. The thicknesses of the lesion and covering layer over the tumor ducts were measured at the center of the lesion. The diameter of the vessels was measured as the shortest diameter of the 10 largest vessels observed within the covering layer over the tumor ducts.
Statistical analyses
All statistical analyses were performed with GraphPad Prism 7 (GraphPad Software, San Diego, CA, USA). To compare averages of data between 2 independent groups, Student's t-tests were performed and presented as mean±standard error of the mean. P-values <0.05 were considered statistically significant.
RESULTS
Patient characteristics
Summaries of background characteristics of 8 patients are shown in Table 1. Four patients (50%) were male, and the mean age was 71.6±3.74 years. There were no significant differences in sex and age between the HP-uninfected and HP-eradicated groups.
Table 1
Patient characteristics and endoscopic findings of GA-FG-CCPs
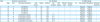
GA-FG-CCP = gastric adenocarcinoma of the fundic gland type (chief cell predominant type); WLI = white light imaging; M-NBI = magnifying endoscopy with narrow-band imaging; HP = Helicobacter pylori; duration = duration between successful HP eradication therapy and incidence of GA-FG-CCP; BG = background; SMT = submucosal tumor; DL = demarcation line; MV = microvascular; MS = microsurface; F = female; M = male; U = upper; M = middle; L = lesser curvature; G = greater curvature; A = anterior.
Macroscopic findings
Representative endoscopic findings of 4 patients (2 cases of GA-FG-CCP seen in the HP-uninfected group and 2 cases of GA-FG-CCP seen in the HP-eradicated group) in routine observation (WLI) are shown in Fig. 1. Endoscopic findings of WLI are presented in Table 1. All lesions were small, with diameter <15 mm. Average lesion sizes were 7±2.0 mm and 9.5±1.2 mm in the HP-uninfected group and HP-eradicated group, respectively, and there was no significant difference (P=0.38). There was no difference in appearance and location between the 2 groups. These results indicated that GA-FG-CCP generated on the normal mucosa and atrophic mucosa displayed similar macroscopic findings.

M-NBI findings
Representative M-NBI images are shown in Fig. 2. The classification of microvascular and microsurface structures of each lesion is shown in Table 1. All lesions in the HP-uninfected group had no demarcation line with regular microvascular and microsurface patterns. Slightly elongated microvessels were observed, but there was no change in diameter and meandering of vessels. In contrast, the existence of the demarcation line and pattern of microsurface structure differed by lesion in the HP-eradicated group. The microvascular pattern observed in the HP-eradicated group was also classified into regular microvascular pattern. However, characteristic tapered microvessels that branched from larger cyanic vessels at the deeper layer were observed in all lesions in the HP-eradicated group. Notably, GA-FG-CCP generated in the normal mucosa of the HP-uninfected group did not show these characteristic microvessels.

Pathological findings
All lesions were pathologically diagnosed by H&E staining and immunohistochemistry. Thin epithelium and a decreasing number of fundic glands in the background mucosa were observed in the HP-eradicated group, which was consistent with endoscopic findings of mucosal atrophy. Of 4 patients, 3 showed metaplastic change in the intestinal mucosa in the background epithelium. The diagnosis of GA-FG-CCP was confirmed by mucin phenotype and cellular differentiation toward chief and parietal cells. As shown in Table 2, all lesions exhibited negative staining for MUC2 and positive staining for MUC6, which indicated gastric phenotype of mucin. Furthermore, all lesions exhibited diffuse staining for pepsinogen I. Of all, case 2 showed positive expression of H+/K+-ATPase. Consistent with previous studies, all cases did not exhibit overexpression of p53 and high Ki67 index, which suggested their lower malignant potential. As seen in the macroscopic findings, tumor cells expanded and formed clusters in the middle to lower part of the mucosa and uplifted the normal surface that consisted of fundic glands in the HP-uninfected group (Fig. 3A). In contrast, in the HP-eradicated group, the covering layer over tumor cells was thinner than that seen in the HP-uninfected group (Fig. 3B). Quantitative analysis showed that there was no significant difference in thickness of the lesions between the 2 groups (Fig. 3C), whereas the covering layer was significantly thinner in the HP-eradicated group (350.5±13.1 µm vs. 138±65.7 µm, P<0.05) (Fig. 3D). Further investigation revealed that a decreased number of original fundic epithelial cells was observed in thinned covering layer in the HP-eradicated group (Fig. 3E and F), and the foveolar epithelium was as thin as the background atrophic epithelium (Fig. 3G and H).
Table 2
Pathological findings and prognosis of gastric adenocarcinoma of the fundic gland type (chief cell predominant type)
Fig. 3
(A, B) Representative H&E staining of all cases of GA-FG-CCP generated in the HP-uninfected group (A) and HP-eradicated group (B) showed the difference in the thickness of covering layer over the tumor ducts. (C) There was no significant difference in thickness of the lesions between the HP-uninfected and HP-eradicated groups. (D) The covering layer over the tumor ducts seen in the HP-uninfected group was significantly thicker than that in the HP-eradicated group (350.5±13.1 µm vs. 138±65.7 µm, P<0.05). Data are expressed as mean±standard error of the mean. (D, E) High-magnification view focusing on the surface lesion of H&E staining of all cases of GA-FG-CCP generated in the HP-uninfected group (E) and HP-eradicated group (F) showed the difference in the number of residue of fundic epithelial cells. (G, H) H&E staining focusing on the border of the lesions of GA-FG-CCP generated in the HP-uninfected group (G) and HP-eradicated group (H) showed the difference in thickness of the background mucosa.
HP = Helicobacter pylori; H&E = hematoxylin and eosin stain; GA-FG-CCP = gastric adenocarcinoma of the fundic gland type (chief cell predominant type); NS = not significant.

The diameter of vessels located just below the surface of the lesion observed in the HP-eradicated group was larger than that observed in the HP-uninfected group (Fig. 4A and B). The average diameter of vessels that was calculated in the 10 vessels existing in the surface lesions over tumor ducts was significantly larger in the HP-eradicated group than that in the HP-uninfected group (44.5±9.8 μm vs. 17.0±3.0 μm, P<0.05) (Fig. 4C). Moreover, predominant infiltration of inflammatory cells including neutrophils and lymphocytes were noted in 3 of 4 patients in the HP-eradicated group; consequently, these patients showed expansion of the tumor stroma (Fig. 4A and B).
Fig. 4
(A, B) Representative hematoxylin and eosin stain staining focusing on the surface of the lesion generated in the HP-uninfected group (A) and HP-eradicated group (B). (C) Vessels observed within the covering layer of gastric adenocarcinoma of the fundic gland type (chief cell predominant type) generated in the HP-eradicated group were significantly larger than those in the HP-uninfected group (44.5±9.8 μm vs. 17.0±3.0 μm, P<0.05). Data are expressed as mean±standard error of the mean.
HP = Helicobacter pylori.

DISCUSSION
There were few studies on GA-FG-CCP generated in the atrophic mucosa after successful HP eradication therapy. In this study, we analyzed 4 cases of GA-FG-CCP found in the atrophic mucosa and compared them to the lesions of which the background was totally matched. As a result, we found that the appearance of GA-FG-CCP generated in the atrophic mucosa was similar to that generated in the normal mucosa. While GA-FG-CCP generated in the HP-uninfected mucosa exhibited 4 previously reported features, 1) submucosal tumor-like shape, 2) whitish color, 3) dilated vessels with branching architecture, and 4) background mucosa without atrophic change, we found that the atrophic mucosa post HP eradication therapy was able to generate similar elevated lesions. Previous studies on GA-FG-CCP observed in the HP-uninfected normal mucosa have explained that submucosal tumor-like appearance was due to covering normal fundic glands and foveolar epithelium over tumor cells. Cases reported in previous studies also indicated results similar to ours that HP eradication therapy might influence the appearance of GA-FG-CCPs; however, it was uncertain whether the background epithelium was atrophic [712]. In this study, our histological investigation revealed the original mucosal layer covering tumor cells was significantly thin in the HP-eradicated group. Change in the thickness of the covering layer had 2 reasons. First, a decreased number of original fundic epithelial cells was observed in the thinned covering layer in the HP-eradicated group. Second, the foveolar epithelium itself was as thin as the background atrophic epithelium. However, no significant effect on appearance was observed by WLI. Although both decrease in the number of fundic glands and thinned foveolar epithelium were observed in the HP-eradicated group, the residue of fundic glands was seen in the surrounding mucosa around the GA-FG-CCP generated in the HP-eradicated group. This observation is important in seeking evidence on why GA-FG-CCP could generate in the atrophic mucosa.
M-NBI can visualize microvessels and microstructures of surface pits. Classifying microvascular and microsurface structures into regular, irregular, and absent pattern enabled us to endoscopically determine whether the lesion was tumor or non-tumor and what type of tumor (I-EGC or D-EGC) the lesion was. Furthermore, evaluating the borderline of microvascular or microsurface pattern (also called demarcation line) contributed to the determination of the range of lesion [1516181920]. Moreover, the existence of the demarcation line means that the tumor cells or duct reaches the surface of the lesion. In contrast to the WLI findings, the M-NBI findings were clearly different between the 2 groups. The thinner covering layer enabled to see through tumor microvessels branching from larger vessels from the surface of lesions by M-NBI. Furthermore, expansion of tumor stroma might enable to see dilated vessels as withered branches. Based on the findings that these tapered microvessels like withered branches did not exhibit diversity in diameter and heterogeneous distribution, we regarded them as regular vessels and clearly distinct from corkscrew microvessels in D-EGC. We would like to describe these characteristic vessels as “microvessels like withered branches.” The diametric change in vessels might contribute to the visualization of microvessels like withered branches by M-NBI. As there was no irregular vessel in the surface of the lesion generated in the HP-uninfected group, the appearance of vessels in the HP-eradicated group did not deviate from regular vascular pattern. The common finding in the formation of vessels like withered branches was efficient to distinguish vessels of GA-FG-CCP generated in the atrophic mucosa from that generated in the normal mucosa. Notably, we emphasize that the area where withered branches were seen was not clearly separated from other areas with distinct vessel pattern; thus, the finding of withered branches cannot provide diagnostic value in the VS classification system by M-NBI. In the future, further studies validating whether the finding of withered branches is specific in GA-FG-CCPs generated in atrophic mucosa should be conducted.
This study has several limitations. First, this was a retrospective observation study conducted in only 1 institution, and we analyzed only 8 cases of GA-FG-CCP. Moreover, we excluded a case with current HP infection. Further studies including cases with current HP infection should be conducted to clarify the exact effect of HP on the appearance of GA-FG-CCP. Second, all patients underwent biopsy sampling preceding observation by M-NBI; thus, the effect of biopsies on the findings of M-NBI and pathology cannot be excluded.
 XML Download
XML Download