

 Citation
Citation Print
Print


BACKGROUND
Psychosocial stress factors in the workplace affect the health of workers in various ways [1]. In terms of mental health, there has been an increase in the recognition of the importance of the effects of occupational stress factors [234]. Job strain model, which is combination of low job control and high job demand, extensively associated with various health problems [5]. Since the publication of a book on the ecology of organization by Adams [6], who first described the concept of ‘justice issues’ based on equity theory, research on organizational equity has been growing researchers attention. During this period, a number of studies have shown that justice plays an important role in the socio-organizational context. These studies focused on the point that organizational equity, i.e., whether an individual is treated fairly, has an important influence on work [16].
Organizational justice has also been proposed and recognized as a useful model for identifying occupational stress factors [1]. Organizational justice as originated from the equity theory described by Adams includes 3 sub-concepts: procedural justice, relational justice, and distributive justice [7]. Procedural justice assesses the stress related to the decision-making process of organization. Whether an organization's decision-making process is rational and democratic, it reflects the employees' opinion on the decision. Flexible convergence of opinions and assess ethics of the decision-making process. Relational justice indicates whether managers or senior staff respect workers and provide sufficient information. Distributive justice indicates whether the organization's resources are appropriately distributed according to the responsibility, ability and experience of workers [15].
It should be noted that the concept of organizational justice may be overlapped with other job stress model. For example, in the widely used job strain model of Karasek, ‘job control’, which refers to the control level over the decision-making process, can be considered part of procedural justice. Also, elements which indicate support of a senior worker can be overlapped with those that construct relational justice [8]. Effort-reward imbalance model also has similar concept of relation between reward and distributive justice. Among the items of Korean occupational stress scale (KOSS), which is widely employed for job stress evaluation in Korea, those involving relationship conflict domains can be considered similar to some items concerning relational [9]. However, organizational justice is different from such psychosocial factors. Organizational justice specifically explores the organizational structure perspective of the workplace. And it focuses on decision making process, relationship between managers and employees, the resources allocations within the workplace.
Previous studies reported clear linking between organizational justice and workers health. A meta-analysis study of U.S. shows systolic and diastolic blood pressure was increased with lower level of procedural justice. A prospective cohort study conducted in Japan found the insufficient relational justice is associated with insomnia, and the lack of procedural justice was shown to be associated with mental illness, self-rated health status, sickness absence, and increased risk of psychological distress [1011].
Although organizational justice model is widely used for assessing relationship between the job stress and health in overseas, yet in Korea the model has not used for the job stress and health of workers.
Therefore, the purpose of this study is investigating association between organizational justice which is composed of 3 subcategories and depressive symptoms among office workers in a securities company.
METHODS
Study setting and participants
A cross-sectional study based on a job stress survey was conducted during 18th of August to 2nd of November, 2016 among workers at a securities company in Korea. The company, headquartered in Seoul, was engaged in securities, asset management and fund operations. Fifteen hundred copies of the questionnaire were distributed and completed. The questionnaire included items addressing basic personal information, lifestyle habits such as smoking and drinking, working conditions and socioeconomic status, stress model with Organizational Justice and the KOSS. Also, the Center for Epidemiologic Studies Depression (CES-D) scale was used for estimating prevalence of depressive symptom [12]. The survey was conducted with method of anonymous self-reporting. 1,500 questionnaire copies were distributed to headquarters and branches by Korea Institute of Labor Safety and Health works through trade union, 1,122 (74.8%) copies were collected. After excluding questionnaires with missing data, the number of study participants was 689 (45.9%).
Variables
Socio-demographic and work-related characteristics
General characteristics surveyed included sex, marital status, and alcohol intake quantity per sitting, smoking, exercise, and medical history. Alcohol intake quantity per sitting was based on intake of Soju, Korea's popular alcohol, with options of either less than 0.5 bottle, between 0.5 to 1 bottle, and more than 1 bottle. Exercise amount was based on 30 minutes or more of aerobic activity, and offered options of either no exercise, less than 2 times weekly or more than 3 times weekly. Medical history assessed hypertension, diabetes, depression, and other illness diagnosed by a doctor. Other illness refers to all diseases diagnosed by doctors except for diagnosed hypertension, diabetes and depression. For this study other illness is included in the model as a single variable. Job classification was based on six categories which are branch sales, branch management, head office sales, head office management, information technology, and customer service center, and job positions were classified as employee, assistant manager, manager, deputy general manager and manager or above.
Questionnaire for organizational justice
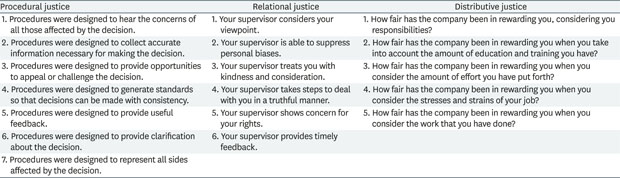
For this study, we translated and utilized the Moorman survey questionnaire, which is widely used to evaluate organizational justice in previous studies [13]. The questionnaire was translated by one researcher of this study than reverse translated by another researcher. Suitability of translation was confirmed from a professional translator. This survey questionnaire evaluates the subcategories of procedural justice, relational justice and distributive justice, and includes multiple scales. The procedural justice scale measures the extent to which the respondent agrees to the procedures of the workplace. The relational justice scale measures the evaluation of the general behavior of the respondent's seniors. Distributive justice is a sub-scale that measures the distribution of resources appropriate to responsibility, effort, and experience. For these 3 subcategories of organizational justice, responses were given along a 5-point scale from 1 (strongly disagree) to 5 (strongly agree). This survey questionnaires used in this study is provided in Appendix 1 [14].
Standardization scores were computed based on 3 elements of each organizational justice domain. Each score was weighted to obtain a score between 1 to 100 points. Higher scores indicate higher levels of organizational justice. The total sum of 3 subcategories was classified as ‘Lower’, ‘Intermediate’, and ‘Higher’ regarding the level of organizational justice. The level of organizational justice thus increases from the lower group to the higher group.
Depressive symptoms
Depressive symptoms were assessed with the CES-D. CES-D is a used to distinguish in the general population and is not a diagnostic tool for clinical depression, but it was regarded to be reliable and valid [15]. A cutoff score of than 21 points indicates a moderate depressive symptom, and a score higher than 25 points is considered indicates a significant depressive symptom [16]. In this study, more than 21 points was defined as ‘depressive symptoms’ for analysis.
Statistical analysis
Descriptive statistics and χ2 test were applied for studying general characteristics and difference of characteristics with or without depressive symptoms. Multiple logistic regression models are used for assessing the relationship between organizational justice and depressive symptoms. The scores obtained from the survey results of procedural justice, relational justice, and distributive justice were classified into 3 categories. The depressive symptom survey results were categorized into dichotomous. Model 1 assessed unadjusted odds ratio (OR) through univariate analysis. Model 2 included variables of biological factors, such as hypertension and diabetes and lifestyle habits such as sex, alcohol consumption, smoking, exercise, and illness excluding depression. Model 3 included variables from model 2, as well as jobs and positions, which are related to job performance. In addition, levels of job demands, job decision latitude, and job insecurity in the KOSS included in model 3.
All statistical analyses were performed using Stata version 13.1 (StataCorp., College Station, TX, USA).
RESULTS
Table 1 shows general demographic characteristics of study participants. Out of 689 respondents, 350 (50.8%) were males and 548 (49.5%) were married. By age group, 335 (48.6%) respondents were the most at 31–40 years old, followed by 41–50 at 269 (39.0%). Almost half (335 or 48.6%) reported a job classification of branch sales, followed in order by branch management, head office management, head office sales, information technology, and customer service center. the most frequent job position was deputy general manager with 178 (25.8%) of respondents, followed in order by manager, assistant manager, employee and higher than general manager. Two hundred ninety-one (42.2%) of respondents reported in taking less than 3 glass of alcohol per sitting. Three hundred thirty-four (48.5%) respondents did not exercise. One hundred thirty-nine (20.2%) of respondents were smoker. Ninety-one (13.2%) respondents were diagnosed with hypertension, and 24 (3.5%) respondents were diagnosed with diabetes.
Table 1
Characteristics of study participants and depressive symptoms

We also compared characteristics of study participants according to depressive symptoms. Participants were compared based on depressive symptoms. Of 689 participants, 195 (28.2%) were observed to have depressive symptoms. The groups showing and not showing depressive symptoms were compared based on the socioeconomic characteristics of the participants. The risky alcohol consumption group and smokers had higher prevalence of depressive symptoms. Also, higher prevalence was shown within patients of diabetes and hypertension. Sex, marital status, job, position, and exercisewere not significantly associated with depressive symptoms.
The association between subcategory of organization justice and job classification is shown Table 2. Organizational justice is divided into three levels: higher, intermediate, and lower. Although no significant association observed for levels of distributive justice, significant associations were observed for procedural justice and relational justice. There, regarding procedural justice, the proportions of the lower level of justice were relatively higher for customer service center (26.7%) and branch sales (18.8%). Regarding relational justice, the percentages in the lower level of justice were relatively higher for branch sales (36.7%) and head office sales (35.6%).
Table 3 showed the association between job position and subcategories of organizational justice. However, there was no significant association between job position and three subcategories of organizational justice.
Table 2
Levels of organizational justice by job classification

Table 3
Levels of organizational justice by job position

The reliability of the items of the organizational justice survey questionnaire translated into Korean was analyzed by the Cronbach's α coefficient [17]. The Cronbach's α coefficient was 0.93 for procedural justice, 0.93 for relational justice, and 0.95 for distributive justice, indicating that the internal consistency of the survey questionnaire is reliable.
Table 4 shows association between each subcategory and depressive symptoms by logistic regression. In the model 2, compared to the reference group (higher level of organizational justice), OR of intermediate group is 1.83 (95% confidence interval [CI], 1.21–277) and OR lower group was 2.79 (95% CI,1.58–4.90) for procedural justice. Similarly, OR of intermediate group is 2.52 (95% CI, 1.21–277) and OR of lower group was 4.25 (95% CI, 2.66–6.78) for relational justice and OR of intermediate group is 2.48 (95% CI, 1.56–4.08) and OR lower group was 4.53 (95% CI, 1.58–4.90) for distributive justice. In every subcategory of organizational justice model dose-response relationship was observed and the lower levels of organizational justice is linked with the higher prevalence of depressive symptoms.
Table 4
Organizational justice levels and depressive symptoms by logistic regression analysis

OR: odds ratio; CI: confidence interval.
*Model 1 was adjusted based on sex, age, alcohol intake quantity per sitting, smoking, exercise, and medical history of hypertension and diabetes mellitus; †Model 2 included variables of model 1, job, position, job demands, job decision latitude, job insecurity.
DISCUSSION
Organizational justice is a concept that illuminates whether workers are treated justly at their workplace [5]. It is known to play an important role as a marker for overall organizational attitude, including the emotions and behaviors of workers. There is also an accumulation of research results on the negative effects on the mental health of workers from unfair treatment [18].
Lower level of organizational justice is linked to higher prevalence of depressive symptoms. Even after adjustment other potential confounders, depressive symptoms especially at lower levels of organizational justice are higher than other groups. In all 3 subcategories of organizational justice, the risk of depressive symptoms significantly increased as justice scores moved downwards from the higher group. It can be concluded that this study indicates that there is a dose-response relationship between the level of organizational injustice and the prevalence of depressive symptoms. This result of study indicated that mental health of workers could be deteriorated by lower level of organizational justice.
Interrelation between organizational justice and depressive symptoms can be explained by Lazarus and Folkman's cognitive appraisal model of stress and coping [19]. Lazarus and Folkman's model refers to work experiences that have detrimental effects as stressors. An event is regarded as a stressor with 2 step appraisal processes. In the primary process, the encountered event is cognitively evaluated for its potential for harm or loss. If individuals perceive the event as threatening, a secondary process is initiated, centering on whether one has enough resources to meet the situational demands to prevent threat of harm or loss. The model suggests that individuals experience stress if they feel they do not have the resources they need, and long-term stresses represent psychological symptoms such as depression [20].
The results of this study are consistent with previous studies. Lower levels of organizational justice can lead to issues in poor mental health. A longitudinal study that was conducted in Finland showed organizational injustice lead to increasing level of sickness absences and minor psychiatric morbidity. In that study, men in the low level of organizational justice group had a 41% higher risk (relative risk [RR], 1.4; 95% CI, 1.1–1.8) of sickness absence than those in the high-level group, while women had a 12% higher risk (RR, 1.1; 95% CI, 1.0–1.2). Regarding the minor psychiatric morbidity in this same study, the OR in men was 1.6 (95% CI, 1.0–2.6) and in women was 1.4 (95% CI, 1.2–1.7). A study conducted in the Netherlands also showed perceived justice to contribute to lowering depressive symptoms. In that study, the depressive symptoms affecting organizational justice was also found [21].
This study may be the first study explores the association between organizational injustice and depressive symptoms in Korea. When the survey survey was conducted, reliability and validity of Korean version of questionnaire which was used in this study had not been certified. However, the correlation between organizational structure, which is similar to organizational justice model, and depressive symptoms was explored. A study conducted in Korea among firefighters discusses the association between organizational system and depressive symptoms. The survey items used in this study on organizational system were fairness, organizational support, balance between union, and autonomy, which are similar idea that of organizational justice. In a previous study, the group with low level of organizational system showed 8.3 times higher risk of depressive symptoms than that of the high-level group (OR, 8.03; 95% CI, 1.73–37.22) [22].
The proportion of depressive symptoms in this study was higher than that of the general population. Out of 689 participants, 195 (28.15%) were considered to have depressive symptoms. The prevalence of depression with 25 points or higher on the CES-D scale had a large variation of 8.7%–21.1% in a previous epidemiological study using identical questionnaire. Considering that ages 20-40 show the lowest depression symptoms (7.6%–10.1%) and that depressive symptoms are higher with low education levels and poor financial conditions, the frequency of depressive symptoms in this study observed higher than general population [23]. At the point of survey, the company was under merger and acquisition. Workers in the company might have tendency of job insecurity at that time. Results of a sociological study have shown the perception of downsizing procedure and compensation, external pressures, and victim mentality to influence anxiety and depression through perception of changed working conditions [24]. This suggests that the characteristics of the workplace undergoing the pressure of downsizing at the time when the survey was conducted may have influenced the prevalence of depressive symptoms when compared to that of general population.
In January 2018, after this study was conducted, Korean version of Organizational Justice Questionnaire was presented [25]. For that questionnaire, Cronbach's α coefficients of the internal consistency reliability was 0.92 for procedural justice and 0.94 for interactional justice. The translated questions were similar to the translated questions of this study. For East Asian countries like Korea, the organizational structure is more vertical, collective and hierarchy-oriented than the Western countries. We suggest that further studies on the association between mental health of workers and organizational justice in Korea are needed with the official questionnaire.
This study has several limitations. First, as this was a cross-sectional study, it was not possible to establish the causal relationship between organizational justice and depressive symptoms due to the time sequence. Second, it should be noted that the depressive symptoms and not clinical depression that is not diagnosed by psychiatric specialists. Third, this study was conducted in workers at a securities company, and result of the study could not apply to other industries. Forth, the complete response rate of questionnaire was low because the survey was conducted byself reporting of trade union members without survey reporters. Fifth, selection bias cannot be excluded since the survey was done by only in trade union membership and only in agreed with survey and low rate of complete response. Sixth, the survey questionnaire was not officially translated into Korean when this survey was conducted.
CONCLUSION
This study may be the first Korean study applied an organizational justice mode among more than 600 workers. In this study, clear association was observed between organizational justice and mental health. Researchers have to pay attention to the organizational justice of workplace for mental health of workers and in the future, prospective cohort studies are required for making causal relationship between organization justice and wokers’ health.
 XML Download
XML Download