

 Citation
Citation Print
Print



Abbreviations
BMI
body mass index
CES-D
Center for Epidemiologic Studies Depression Scale
CVD
cardiovascular disease
DBP
diastolic blood pressure
EMS
electronics manufacturing services
IRB
Institutional Review Board
FBS
fasting blood sugar
HbA1c
hemoglobin A1C
HDL-C
high-density lipoprotein cholesterol
hs-CRP
high-sensitivity C-reactive protein
KOSS-SF
Korean Occupational Stress Scale-Short Form
LDL-C
low-density lipoprotein cholesterol
PSQI
Pittsburgh Sleep Quality Index
SBP
systolic blood pressure
TG
triglycerides
WC
waist circumference
BACKGROUND
The definition of shift work in a narrow sense means a work schedule in which the same task is repeated from 1 worker to the next within 24 hours [1]. However, shift work is usually defined in a broader sense to include all hours worked outside of regular daytime hours, including night duty and rotating shift work [12]. In modern society, the number of people on shift work is increasing in accordance with social and economic needs. In a recent survey on work environments, the percentage of workers in the European Union who perform shift work rose from 17% in 2010 to 21% in 2015 [3]. According to the 4th Korean working condition survey conducted by the Occupational Safety and Health Research Institute in 2014, the proportion of Korean workers who perform night work more than 5 days per month was 7.5% and the proportion of workers who perform rotating shift work was 7.1% and have been continuously increasing since the start of the investigation in 2006 [4].
With the increase in the number of shift workers, many studies have been performed regarding the health problems that can occur due to this work. Epidemiological studies have identified shift work as a risk factor for chronic illnesses such as cardiovascular disease (CVD) [5], metabolic syndrome [6], breast cancer [7], depression [8], and sleep disorders [9].
Of these, CVDs comprise a large proportion of deaths worldwide, ranking as the fourth-highest cause of death in 1990 and the single largest cause of death in 2010 [10]. CVDs are an important public health condition in that the incidence rate can be lowered by controlling the risk factors and the mortality rate can be lowered with proper treatment of acute, chronic, and ischemic heart diseases [11].
Recent studies have assessed the development of CVDs due to shift work. Combining previous research findings, Puttonen et al. [12] proposed that shift work can cause an imbalance in the body's circadian rhythm which leads to psychosocial, behavioral, and physiological stress, which then can result in CVD. This model suggests that the complex interaction among “psychosocial stress” such as work stress, reduced recovery from work, and work-life imbalance; “behavioral stress” such as short sleep length, bad sleep quality, smoking, nutritional imbalance, physical inactivity, and weight gain; and “physiological stress” such as inflammation, blood coagulation, increased blood pressure due to activation of sympathetic nervous system, and overactivation of hypothalamic-pituitary-adrenal-axis can influence the development of diseases such as atherosclerosis, metabolic syndrome, and type II diabetes, which increases the risk of CVD.
Research has evaluated the relationship between CVD and inflammation, defined by Puttonen et al. [12] as “physiological stress”. The formation of atherosclerosis, the underlying pathology of CVD, is caused by a complex inflammatory response rather than a simple accumulation of lipids in the lining of the blood vessels. Inflammation plays a key role in the entire process of atherosclerosis, from the first stage of coagulating white blood cells into the inner walls of the arteries to the last stage of unstable plaque rupture [13]. A typical indicator of inflammatory condition is high-sensitivity C-reactive protein (hs-CRP) which is strong predictors of CVD [14]. The hs-CRP were significantly higher in shift workers than in daytime workers, suggesting that inflammation is a possible pathway linking shift work and CVD [15]. A prospective study by Ridker et al. [16] on healthy post-menopausal women investigated the risk of CVD associated with baseline levels of markers of inflammation, reporting that hs-CRP level was a univariate predictor of the risk of cardiovascular events. In this study, the predictive value of hs-CRP to predict CVD risk was significantly higher than that of prior physiological markers of CVD (total cholesterol, high-density lipoprotein cholesterol [HDL-C], and low-density lipoprotein cholesterol [LDL-C]) and that of new markers (lipoprotein(a), homocysteine, and apolipoproteins A1 and B).
Furthermore, an advantage of hs-CRP in predicting CVD is that the long-term physiological fluctuation of hs-CRP is small within individuals. A study of 236 subjects showed high correlations between log-normalized CRP levels in within-subject pairs of blood samples from the baseline period and after 5 years (r = 0.60) [17]. Thus, these findings suggest that inflammation plays a role in the pathogenesis of CVD in shift workers and that hs-CRP may be a good marker of the level of inflammation.
In a study on gender differences in hs-CRP levels, women showed higher levels than those in men and the increase of hs-CRP with an increase in body mass index (BMI) was also greater in women [18]. While men showed no difference in hs-CRP level depending on the length of sleep, women showed a significant difference [19]. Therefore, hs-CRP level and the response to the cardiovascular risk factors of hs-CRP differ between sexes; however, to our knowledge, the only studies to analyze hs-CRP levels in shift workers in Korea included only male subjects. Therefore, the present study compared the hs-CRP levels of female daytime and shift workers in electronics manufacturing services (EMS) in order to examine the association between shift work and hs-CRP in female workers.
METHODS
Study participants
Female workers of an EMS who received special medical examinations for workers at a university hospital in Changwon, Gyeongnam, Korea between January 2017 and December 2017 were enrolled in this study. Of a total of 2,154 recipients of medical examinations, 620 were female; after excluding those with missing data, history of CVD, cerebrovascular disease, hypertension, diabetes mellitus, and those who had recently suffered an infectious disease, a total of 589 women were recruited as subjects.
The work schedule of research subjects was Monday through Friday from 8 am to 5 pm for daytime workers. And some selective and autonomous work schedules allowed daytime workers to adjust their work hours freely within 52 hours a week. In contrast, the shift workers had a 2-rotation, 3-team schedule, which meant a rotation of 4 days of daytime work and 2 days off, followed by 4 days of nighttime work and 2 days off. The work hours for daytime and nighttime work were 8 am to 8 pm and 8 pm to 8 am, respectively.
General and psychological characteristics
For sociodemographic characteristics and daily habits, we investigated participant age, marital status, education level, alcohol consumption, smoking, and regular exercise as well as their quality of sleep, work stress, and level of depression.
Marital status was divided into married and other (unmarried, divorced, or widowed). Education level was divided into high school graduation or lower and college graduation or higher. For alcohol consumption, the subjects were categorized as a “drinker” (consumed alcohol 1 time or more per week) or a “non-drinker” (consumed alcohol less than 1 time per week). For smoking, the subjects were divided into current smokers and current non-smokers. For regular exercise, the subjects were divided into “regular exercise” (exercised 3 or more times per week) and “irregular exercise” (exercised fewer than 3 times per week). Occupational class was divided into white-collars and blue-collars. White-collar workers were mainly in the administrative and research & development departments, while blue-collar workers were in manufacturing and assembling departments for semiconductors and electronics.
The quality of sleep was evaluated using the Pittsburgh Sleep Quality Index (PSQI). The quality of sleep in the past month was evaluated on 7 subscales of subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbance, use of sleeping medication, and daytime dysfunction, with a total combined sleep value score between 0 and 3 for each subscale. A higher PSQI indicated poorer sleep quality.
Work stress was evaluated using the Korean Occupational Stress Scale-Short Form (KOSS-SF). The KOSS-SF contains 24 items in 7 areas of job demand, insufficient job control, interpersonal conflict, job insecurity, organizational system, lack of reward, and occupational climate. The score for each area is converted into a 100-point scale, the average of which was used in the present study. A higher score indicated a higher level of work stress.
The level of depression was measured using the Center for Epidemiologic Studies Depression Scale (CES-D). The frequency of 20 depression-related items in the past week was evaluated on a score of 0 to 3 for each question, and the total sum of the scores was used in the present study. A higher score indicated more severe depression symptoms.
Statistical analysis
The hs-CRP level was treated as a continuous variable and was analyzed after log-transformation. T- and chi-square tests were used to compare the general characteristics and biochemical figures between the daytime and shift worker groups. Age-adjusted partial correlation analysis was performed to examine the linear relationship between hs-CRP level and the risk factors for CVDs. In addition, the difference in hs-CRP levels depending on the work schedule were analyzed through ANCOVA after adjusting for variables that showed a significant difference between daytime and shift workers such as age, waist circumference (WC), BMI, marital status, education level, smoking, systolic blood pressure (SBP), diastolic blood pressure (DBP), LDL-C level, HDL-C level, and triglyceride level. Statistical analysis was done using IBM SPSS Statistics for Windows version 21.0 (IBM Corp., Armonk, NY, USA) with a confidence level set to 95% and significance level set to p < 0.05.
RESULTS
General and psychological characteristics of study participants
Out of 589 total research subjects, 145 (24.6%) were daytime workers and 444 (75.4%) were shift workers. The average age of daytime workers, 31.6 years, was significantly higher than that of the shift workers (27.5 years; p < 0.001). The proportion of married subjects was significantly higher in daytime workers (60.7%) compared to that in shift workers (28.4%; p < 0.001). The proportion of workers with an education level of college graduate or above was higher in daytime workers (64.1%) than that in shift workers (35.8%; p < 0.001). The proportion of current smokers was significantly higher in shift workers (21.6%) than that in daytime workers (4.8%; p < 0.001). There was no statistically significant difference between daytime and shift workers in alcohol consumption and regular exercise. Shift workers had a poorer quality of sleep, with an average PSQI score of 6.4 ± 3.2, in comparison to daytime workers, with an average PSQI score of 5.0 ± 3.0 (p < 0.001). Shift workers also had a higher level of work stress, with an average KOSS-SF total score of 50.2 ± 12.9 in comparison to daytime workers, with an average score of 45.7 ± 12.8 (p < 0.001). The frequency of depression symptoms in shift workers was higher, with a total CES-D score of 11.8 ± 10.0, compared to 9.5 ± 8.3 in daytime workers (p = 0.012) (Table 1).
Table 1
General and psychological characteristics of study participants

Data are shown as mean ± standard deviation or number (%).
PSQI: Pittsburgh Sleep Quality Index; KOSS-SF: Korean Occupational Stress Scale-Short Form; CES-D: Center for Epidemiologic Studies Depression Scale.
*Compared using χ2 test or t-test; †Alcohol consumption: drinker = consume alcohol at least once a week, non-drinker = consume alcohol less frequently than once a week; ‡Regular exercise: yes = exercise 3 times or more per week, no = exercise less than 3 times per week.
Anthropometric and biochemical characteristics of study participants
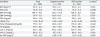
Two groups did not show significant differences in BMI, WC, SBP, fasting blood sugar (FBS) level, hemoglobin A1C (HbA1c) level, triglyceride level, or HDL-C level. The DBP of daytime workers was significantly higher (68.6 ± 8.5 mmHg) than that in shift workers (67.0 ± 7.7 mmHg; p = 0.037). The total cholesterol level of daytime workers was significantly higher (181.6 ± 32.7 mg/dL) than that in shift workers (175.6 ± 30.5 mg/dL; p = 0.043). The LDL-C level of daytime workers was also significantly higher (107.2 ± 28.3 mg/dL) than that in shift workers (100.4 ± 27.9 mg/dL; p = 0.011). The average hs-CRP of shift workers tended to be higher than that in daytime workers (1.07 ± 2.20 vs. 0.92 ± 1.87 mg/L), but the difference was not statistically significant (p = 0.067) (Table 2).
Table 2
Anthropometric and biochemical characteristics of study participants
Data are shown as mean ± standard deviation or number (%).
BMI: body mass index; WC: waist circumference ;SBP: systolic blood pressure; DBP: diastolic blood pressure; FBS: fasting blood sugar; HbA1c: hemoglobin A1C; TG: triglycerides; LDL-C: low-density lipoprotein cholesterol; HDL-C: high-density lipoprotein cholesterol; hs-CRP: high-sensitivity C-reactive protein.
*Compared using t-test; †Log transformed hs-CRP was used for all estimates; mean and standard deviation were back-transformed to return estimates to original hs-CRP units (mg/L).
Correlation of hs-CRP with study parameters
Partial correlation analysis of hs-CRP and CVD risk factors after adjusting for age showed a positive correlation between hs-CRP and BMI and WC. SBP and DBP, HbA1c level, total cholesterol level, LDL-C level, and triglyceride level also showed a weak positive correlation, while HDL-C level showed a weak negative correlation. FBS, CES-D, PSQI, and KOSS-SF values did not show a correlation with hs-CRP (Table 3).
Table 3
Correlation of hs-CRP with clinical or biochemical parameters*

hs-CRP: high-sensitivity C-reactive protein; r: correlation coefficient; BMI: body mass index; WC: waist circumference; SBP: systolic blood pressure; DBP: diastolic blood pressure; FBS: fasting blood sugar; HbA1c: hemoglobin A1C; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol; TG: triglycerides; CES-D: Center for Epidemiologic Studies Depression Scale; PSQI: Pittsburgh Sleep Quality Index; KOSS-SF: Korean Occupational Stress Scale-Short Form.
*Log transformed hs-CRP was used for all correlation analyses; †Compared using age-adjusted partial correlation.
Difference in estimated marginal means of hs-CRP in each group
The difference in hs-CRP levels according to work schedule was analyzed through ANCOVA after adjusting for variables showed correlation with hs-CRP in partial correlation analysis. The analysis showed a significantly higher estimated average hs-CRP level in shift workers (1.324 ± 0.156 mg/dL) than that in daytime workers (0.653 ± 0.350 mg/dL; p = 0.003) (Table 4).
Table 4
Difference of estimated marginal means of hs-CRP at each group*

| Group | Adjusted (mean ± SE)† | p-value |
|---|---|---|
| Daytime worker | 0.653 ± 0.350 | 0.003 |
| Shift worker | 1.324 ± 0.156 |
Adjusted for age, waist circumference, body mass index, marital status, education level, smoking, systolic blood pressure, diastolic blood pressure, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglycerides.
hs-CRP: high-sensitivity C-reactive protein; SE: standard error.
*Log transformed hs-CRP was used for all estimates; adjusted mean and SE were back-transformed to return estimates to original hs-CRP units (mg/L); †Compared using analysis of covariance.
DISCUSSION
As an acute-phase reactant, hs-CRP plays an important role in innate immune response and is considered a marker for the level of inflammation and an intermediary of atherosclerotic diseases. hs-CRP has been shown to induce complement, regulate endothelial nitric oxide synthase expression and nitric oxide synthesis, and upregulate expression of cellular adhesion molecules [20]. Prospective studies of hs-CRP levels in individuals without a history of CVDs showed that a 1-time hs-CRP level measurement in a non-fasting state was a strong predictor of future vascular diseases such as coronary heart disease [21], myocardial infarction [22], stroke [23], and cardiovascular death [24]. Other studies showed that the relationship between hs-CRP level and the increase in future cardiovascular risks was independent of cholesterol and other traditional cardiovascular risk factors [2526].
Several studies have evaluated the relationship between shift work and hs-CRP level. Male and female workers working 2-shift, 3-shift positions in a Finnish airlines company had a higher hs-CRP level and white blood cell count in comparison to those of daytime workers, a relationship that was mostly independent of cardiovascular risk factors [15]. In a Korean study of young male workers working at a display manufacturing company, shift workers had a higher hs-CRP level and white blood cell count compared to those in daytime workers even after adjusting for variables that can increase levels of inflammation markers [27]. Our study showed similar results to those of previous studies reporting significantly higher hs-CRP levels in female shift workers than those of female daytime workers even after adjusting for variables that can influence hs-CRP level, suggesting that inflammation is a possible pathway linking shift work and CVD.
Previous studies have reported differences in hs-CRP levels among sex and race. For example, Khera et al. [18] showed that women and African American people had higher hs-CRP levels than that of men and people of Caucasian descent [17]. Additionally, in a study on the relationship between hs-CRP level and BMI, WC, and waist-to-hip ratio in European and Chinese women and men, Lear et al. [28] showed that sex had a large impact on the relationship between hs-CRP and WC and that the hs-CRP level showed a greater increase in women compared to that in men in individuals with a WC larger than 70 cm. Our study analyzed the change in hs-CRP depending on shift work in Korean women, a subject not previously studied, and found a higher hs-CRP level in female daytime and shift workers in comparison to data from previous studies that analyzed Korean men [27], which support the results of previous studies.
Smoking is a rectifiable, important cardiovascular risk factor and epidemiological studies have related smoking to the development of CVDs [2930]. In particular, smoking has been reported to comprise about 50% of all causes of the development of CVD in middle-aged women [29]. Although the pathogenesis of how smoking causes vascular inflammation remains unclear, previous studies also reported increased hs-CRP levels in smokers [3132]. A systematic review of 14 studies by Frost et al. [33] reported that daytime workers generally had a lower proportion of smokers in comparison to that in shift workers. Compared with future day workers, fixed evening or fixed night workers already smoked more before they began shift work [34]. Being an ex-smoker was significantly associated with 2- or 3-shift work including night work. These results indicate that smoking status should not solely be treated as a mediator between some variants of shiftwork schedules and CVDs but should also be considered a confounder. Therefore, including smoking as covariates may partially dilute the true effects of shiftwork. Although the proportion of smokers in the shift workers was significantly higher in the present study, the trend of results in our study did not change even after adjusting for smoking status.
Psychological stress and sleep deprivation may activate immunological defenses [3536] and are also important pathways of several health effects of shiftwork [37]. Leproult et al. [38] showed in a study on circadian misalignment, insulin resistance, and inflammation, that circadian misalignment alone, independent from insufficient sleep, can increase diabetes risk and inflammation. Furthermore, Morris et al. [39] showed that circadian misalignment in shift workers can increase hs-CRP level and blood pressure irrespective of differences in work stress and quality of food. In our study, work stress (a psychosocial stress), depression symptoms, and quality of sleep (a behavioral stress) did not show a relationship with hs-CRP level. Thus, other variables not included in the study may underlie the observed associations. And the results suggest that circadian misalignment may be a causal factor for the inflammatory response in concordance with previous research, further detailed research is needed.
Our study had several limitations. First, the cross-sectional design is limited in explaining cause-and-effects despite identifying the relationship between shift work and hs-CRP. Shift workers are a selected population and, according to the healthy worker effect, those who cannot adapt to irregular work hours and those with worsened health conditions due to shift work or other reasons are more likely to quit this type work, which can result in a healthy worker effect between daytime and shift workers. However, shift workers showed a higher hs-CRP level in our study; this finding is significant even considering the healthy worker effect. Our study did not specifically categorize previous shift workers, so we could not analyze the health effects of previous shift work; thus, the results may have been confounded by the inclusion of previous shift workers in the daytime worker group. Also, we could not obtain individual data on shift working years, working hours, and work details using medical examination data. Therefore, the effect of these variables on hs-CRP could not be analyzed. These may serve as potential confounding factors and attention should be paid to interpret the results. Moreover, daytime workers are usually office workers while shift workers usually held manufacturing jobs, so there could have been confounding variables that were not investigated in our study such as exposure to substances that could have affected the levels of inflammation in the 2 groups. Further studies will be needed to supplement these limitations.
Despite these limitations, our study is the first study to examine the relationship between shift work and hs-CRP level in Korean female workers. Even after adjusting for variables that can influence hs-CRP level, the hs-CRP level of shift workers was significantly higher than that of daytime workers, which indicated the relationship between shift work and increased hs-CRP level. Because CVD is progressive, periodic examination of hs-CRP level to discover the health effects of shift work early may be important. Furthermore, future prospective research on the prediction of CVD risk using hs-CRP measures in shift workers is necessary.
CONCLUSIONS
In summary, this study investigated the relationship between shift work and increased hs-CRP level in women. In this study, we found statistically significant differences in serum hs-CRP levels between female shift workers and non-shift workers. Because multiple studies have reported associations between increased hs-CRP and CVD, follow-up of hs-CRP may help early detection of CVD in shift workers. This research is a cross-sectional study and validation of the results in a cohort study containing a larger sample size is warranted.
 XML Download
XML Download