

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Psoriasis is a chronic inflammatory skin disease with prevalence of 1%~3% worldwide. Skin lesions are characterized by multiple, well-demarcated, raised, red plaques with a white scaly surface1. It is considered to be a systemic disease because it is frequently accompanied by comorbidities that include psoriatic arthritis (PsA), diabetes, dyslipidemia, and cardiovascular disease23. PsA is an inflammatory arthritis associated with psoriasis and its prevalence varies between 0.02% and 0.42% in the general population45 and between 6% and 48% in psoriasis patients6. The skin manifestations of psoriasis precede symptoms of arthritis by 10 years on average and, in 15% of the total cases, PsA and psoriasis either occur simultaneously or PsA precedes the skin disease7.
Early diagnosis of and prompt intervention for PsA are crucial because delaying treatment may result in devastating, irreversible joint damage. Moreover, PsA is known to be an important determinant of vascular comorbidities in psoriatic patients8. Dermatologists, therefore, have an important role in examining other body systems as well as the skin lesions associated with psoriasis that might be involved in this immune-mediated inflammatory disease (IMID).
However, there is no specific indicator for monitoring systemic inflammation in patients with psoriasis, such as the C-reactive protein levels used in clinical practice to monitor disease activity in rheumatic and inflammatory bowel disease. On the other hand, some screening tools have been developed for the identification of PsA in patients with psoriasis; these include the Psoriatic Arthritis Screening and Evaluation (PASE)9, the Psoriatic and Arthritic Questionnaire10, the Psoriasis Epidemiology Screening Tool11, the Toronto Psoriatic Arthritis Screen12, and the Early Arthritis for Psoriatic Patients13. Of these, PASE has the most questions, with possible scores of 0 to 75, with a broader range to screen arthritis-related symptoms and functions. In this analysis, we sought to determine whether the symptoms of inflammatory arthritis, and their effect on patient functioning, are positively associated with cutaneous disease activity in order to enable better management of patients with psoriasis, in a holistic approach to IMID.
Go to : 
MATERIALS AND METHODS
Study design
The EPI-PSODE14 study was a multicenter, noninterventional, cross-sectional study. The 25 participating centers were primarily university hospitals, located across Korea (with the exception of the Jeju island region). This study was reviewed and approved by the Institutional Review Board of each center (Corresponding author's institution [Asan Medical Center]: IRB no. 2013-0161). To extract a representative sample reflecting the distribution of psoriasis in Korea, the numbers and locations of the study centers were selected on the basis of population distribution and health insurance reimbursement data of patients with psoriasis. Patients were examined and enrolled consecutively in order of visiting the center. After obtaining informed consent, all study procedures were performed on 1 day. The study patients were adults aged 20 years or older diagnosed with psoriasis. Data were collected by interviewing and assessing the patients on demographic factors (age, gender, height, weight, waist circumference, disease duration, age at diagnosis, family history in first-degree relative, drinking/smoking history, and medication history). Physical examinations for disease-severity measures (Psoriasis Area and Severity Index [PASI] and body surface area [BSA]) and blood pressure were performed. Quality of life was evaluated by the Dermatologic Life Quality Index (DLQI) and Medical Outcomes Study 36-Item Short-Form Health Survey (SF-36)15. In order to evaluate patient satisfaction with various therapies, questions from the existing Medication Satisfaction Questionnaire (MSQ) were included16. Lastly, the PASE tool was used to assess arthritis-related symptoms and functions.
Statistical analysis
Descriptive statistics for continuous variables are presented as means with standard deviation (SD), and dichotomous variables are presented as frequencies with percentages in parentheses. Respective proportions are presented using 37 points1718, 44 points19, and 47 points9 as cut-off values in PASE, and variables collected were compared to assess the statistical significance of any differences among the groups using a cutoff threshold of 37 points of PASE (PASE <37 and PASE ≥37) based on a validation study for Korean patients (sensitivity of 77.8%, specificity of 82.3%, positive predictive value of 37.8% and negative predictive value of 96.4%)17. We used, where appropriate, the Mann-Whitney U-test and t-test for continuous variables and Pearson's chi-square test and Fisher's exact test for dichotomous variables, without missing data imputation. In addition, multiple linear regression analysis was used to assess association between disease activity (using PASI) and inflammatory arthritis-related symptoms and functions (using PASE) after excluding the effect of each confounder such as gender, age, and body mass index (BMI) which are considerably related to occurrence of arthritis. All statistical tests were performed using 2-sided tests and p-values <0.05 were considered statistically significant. Analyses were performed using the statistical software package SAS 9.4 (Statistical Analysis System; SAS-Institute, Cary, NC, USA).
Go to :
RESULTS
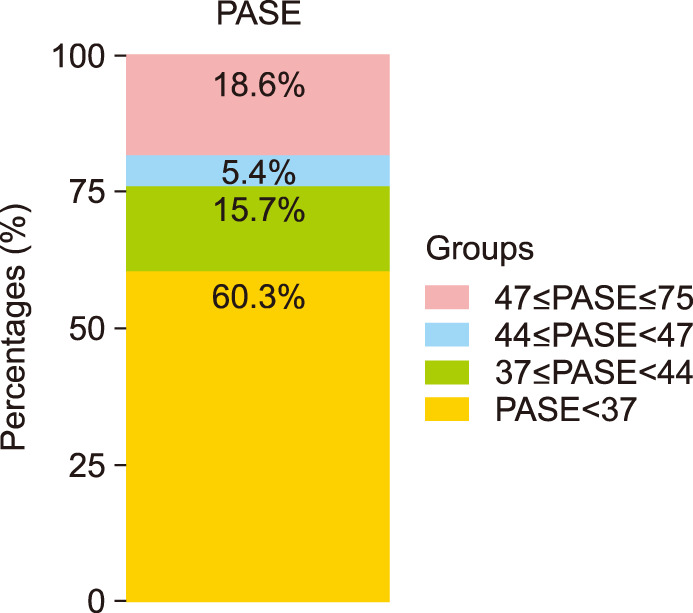
Of 1,260 patients who completed the study, PASE data were available for 1,255 patients. The proportions of patients scoring ≥47, ≥44, and ≥37 points were 18.6% (n= 233), 24.0% (n=301), and 39.7% (n=498), respectively (Fig. 1).
At the 37-point cut-off, there were 757 patients in the group with PASE <37 and 498 in the group with PASE ≥37. The group with PASE ≥37 had a higher proportion of women than the group with PASE <37 (48.8% vs. 34.9%, p<0.0001); older mean age (50.5 years vs. 44.7 years, p<0.0001); and older mean age at diagnosis (41.7 years vs. 36.4 years, p<0.0001). The higher-score PASE group (PASE ≥37) had more severe disease activity using PASI and BSA (difference of PASI=1.5; p=0.0021 and difference of BSA=3.1; p=0.0008, respectively) than the lower-score PASE group (PASE <37). Nail involvement and family history of psoriasis were more frequent in the PASE ≥37 group but this did not reach statistical significance. The group with PASE ≥37 had higher mean BMI (24.1 vs. 23.7, p=0.0411) and greater waist circumference (85.87 cm vs. 83.22 cm, p=0.0002) but there was no significant relationship with blood pressure between the 2 groups. A significantly lower percentage of patients in the group with PASE ≥37 had a smoking and drinking history than the group with PASE <37, but this appears to be affected by the difference in the gender ratio (no statistical significance based on Cochran-Mantel-Haenszel [CMH] test between the 2 groups stratified by gender; smoking (pCMH=0.9297) and drinking (pCMH=0.1261) (data not shown). Regarding medication history, only use of systemic treatment was significantly greater in the group with PASE ≥37 than the group with PASE <37 (66.3% vs. 58.0%, p=0.0032). DLQI and both physical and mental component SF-36 scores were significantly higher in the group with PASE ≥37 compared to the group with PASE <37, and satisfaction with treatment was lower in the group with PASE ≥37 (p=0.0015) (Table 1).
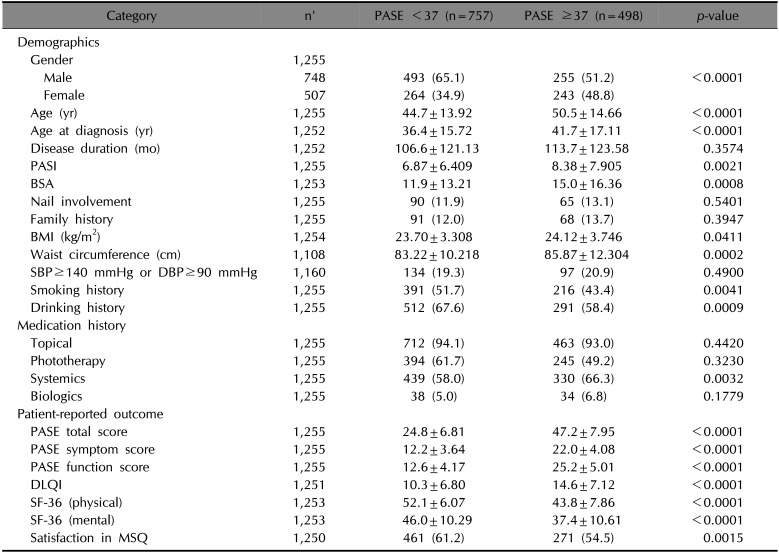
Table 1
Comparison of related factors between 2 groups divided by PASE 37
Values are presented as number (%) or mean±standard deviation. Percentages were based on the total number of subjects with each available result in each group. n': Total number of subjects with each available result, PASE: Psoriatic Arthritis Screening and Evaluation, PASI: Psoriasis Area and Severity Index, BSA: body surface area, BMI: body mass index, SBP: systolic blood pressure, DBP: diastolic blood pressure, DLQI: Dermatology Life Quality Index, SF-36: Medical Outcomes Study 36-Item Short-Form Health Survey, MSQ: Medication Satisfaction Questionnaire.
![]()
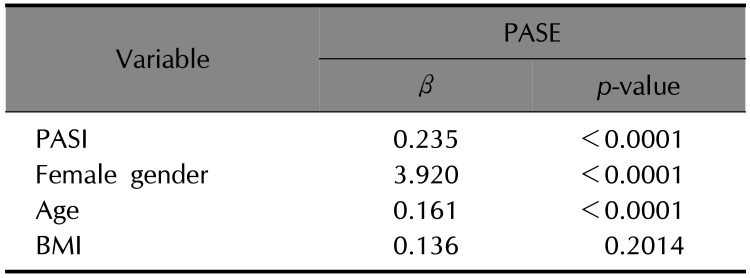
A multiple linear regression model was used to explore the potential for an association between disease severity represented by PASI and PASE scores by designating factors with representativeness among significant independent variables in the univariate analysis. It appeared that female gender, age, and BMI affected arthritis symptoms and function. PASE and PASI were associated with each other, even after adjustment for the these factors (p<0.0001) (Table 2).
The comparison of scores between the group with PASE ≥37 and the group with PASE <37 for each question of the PASE questionnaire is shown in Fig. 2 and Table 3 for the symptom subscale and Fig. 3 and Table 4 for the function subscale. For the symptom subscale, the highest score difference between the 2 groups was for question 2, “My joints hurt”. The highest score in both groups was for question 1, “I feel tired for most of the day”, and the lowest score in both groups was for question 5, “My joints feel hot”. This last question had the lowest score difference between the groups. For the function subscale, the score difference between the 2 groups was highest for question 8, “I feel that my joint problems have affected my ability to work”, then question 12, “I am unable to be as active as I used to be” and question 13, “I feel stiff for more than 2 hours after waking up in the morning”. Lastly, the question with the lowest score in both groups and the lowest score difference between the 2 groups was question 10, “I have trouble wearing rings on my fingers or my watch”.
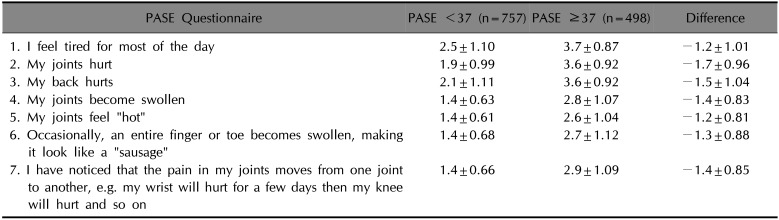
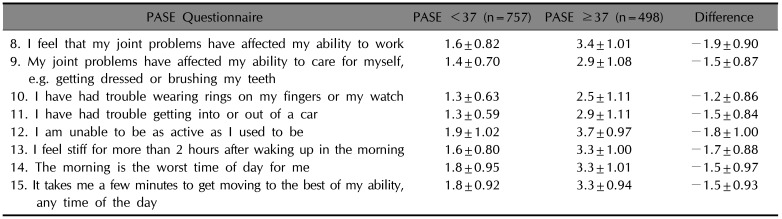
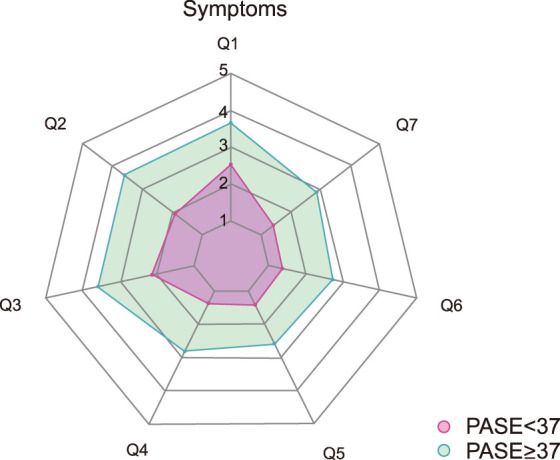
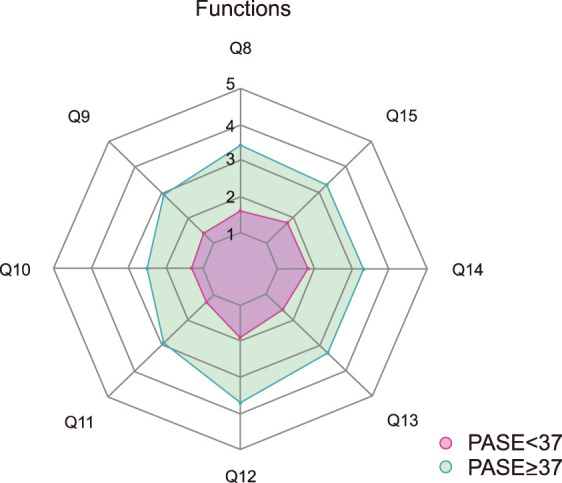
Table 3
Comparisons in symptom subscale of PASE
![]()
Table 4
Comparisons in function subscale of PASE
![]()
Go to :
DISCUSSION
The prevalence of PsA in Korea according to previous studies was approximately 9.0%~14.1%202122. When PASE scores of ≥47, ≥44, and ≥37 were applied as cut-off values, the proportions of screened patients in each group were 18.6%, 24.0%, and 39.7%, respectively. Of these, approximately 40% of patients with a cut-off score of ≥37 validated in the Korean population may require additional assessments to confirm a diagnosis of PsA. In our study, the prevalence of PsA in patients with psoriasis was numerically estimated to be 15.0% by applying positive predictive value of 37.8% to the patients screened with a cut-off of 37 points17. In addition, a recent study performed in Japan showed that the prevalence of PsA in patients with psoriasis reached around 20% in some areas23. Continued studies are required to further characterize the prevalence of PsA in Korea.
The maximum score for the PASE is 75; for a continuous variable with such a wide range, the ability to detect changes becomes relatively greater and sensitivity is higher than a continuous variable with a narrow range. In general, most patients who develop PsA progress from psoriasis alone to psoriasis with PsA and these patients have more severe psoriasis24; this finding aligns with our analysis in which the group with PASE ≥37 showed higher PASI scores and BSA affected than the group with PASE <37. Moreover, disease severity in psoriasis is associated with elevated proinflammatory cytokines25 and this level of inflammation is related to the development of hyper tension26. A systematic review found that there is a greater prevalence of hypertension in patients with psoriasis, and patients with severe psoriasis are more likely to have hypertension than those with mild psoriasis27, consistent with hypertension considered as a type of inflammatory disease28.
The disease severity of psoriasis has been shown to be related to the activity of inflammation. In our analysis, PASE scores were positively associated with PASI scores after adjusting for confounding factors such as female gender, age, and BMI which affect arthritis symptoms and our result also showed positive linearity through each regression coefficient (β) in Table 2. In addition, Husni et al.29 confirmed that the PASE tool is sensitive to changes in response of patients treated with biological therapy, which might be applied similarly to change in disease activity or systemic inflammation. Therefore, the use of PASE could monitor changes in inflammatory activity, in other words disease activity, in patients with psoriasis. PASE is not only used for PsA screening but also for management of psoriasis as an IMID. Patients with PsA showed more severe psoriasis than patients without PsA in some studies243031. In line with these results, our analysis showed that the group with PASE ≥37 had significantly higher PASI and BSA affected than the group with PASE <37; greater and more active systemic inflammation may affect many body systems so this increased disease activity may promote the development of PsA. The most common identified risk factor for development of PsA was the presence of nail disease in many studies303233. In our study, nail involvement was higher in the group with PASE ≥37 than the group with PASE <37, but this was not statistically significant. Obesity has also been shown to increase the risk of occurrence of PsA in some studies3435; this suggests that weight loss may alleviate disease severity and reduce the risk of developing PsA. Consistent with this, the BMI of the group with PASE ≥7 was significantly higher in our study than that of the group with PASE <37. However, further studies are needed to determine the relationship between obesity and development of PsA in Korean patients with psoriasis because the difference in BMI between groups was small (0.42 kg/m2) and weight gain may increase the risk of osteoarthritis, which is not related to systemic inflammation36.
The association between smoking/drinking and PsA is controversial because there have been opposing results from a variety of studies37. In our analysis, the percentage of patients with a history of smoking was higher in the group with PASE <37 using a univariate model, though there was no statistically significant difference between the 2 groups when stratified by gender. In other words, no association between smoking and PASE score was identified in our analysis. Drinking was also not associated with PsA when stratified by gender. Tey et al.38 reported that sex, age of onset of psoriasis, and a family history of psoriasis were not associated with PsA, but our study showed that age at diagnosis was significantly higher in the group with PASE ≥37 than the group with PASE <37.
A potential limitation of the PASE questionnaire is its length, and it may be difficult for patients to complete all 15 questions in the real-world setting of dermatology clinic practice. However, it may be sufficient to use only the questions that showed the greatest difference between the two groups. Question 2, “My joints hurt” in the symptom subscale and question 8, “I feel that my joint problems have affected my ability to work” showed the greatest difference between the 2 groups in our analysis. According to the Turkish PASE tool validation study39, questions 2, 8, and 12 indicated the highest sensitivity (77%) for the answers “agree” or “strongly agree”. This result is closely aligned with our analysis. If the scores for these questions are increased, physicians may consider completing the entire PASE questionnaire with the patient or performing regular follow-up, at least once every 6 or 12 months so that changes in inflammatory activity, which might not be apparent by examination of the skin, may be checked by evaluation of joint symptoms. Lastly, further studies are needed to support results from the present study. For example, a study on specific population excluding confounders could be conducted or a study to follow up changes in intra-subject setting.
In conclusion, PASE scores is independently associated with PASI scores after risk adjustment and can be sensitive to disease activity. From the perspective that psoriasis is treated as one of the IMIDs, PASE may be utilized as a tool to monitor changes in inflammatory activity and their effect on the course of the disease.
Go to :
 XML Download
XML Download