

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Dear Editor:
Cervical chondrocutaneous branchial remnants (CCBRs) are rare, congenital, benign neck masses, and are derived from dislocated branchial apparatus components comprised of cartilage tissues1.
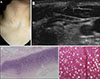
Herein, we describe a 44-year-old female who presented with a solitary asymptomatic skin-colored nodule on the lower part of right side of the neck anterior to SCM (Fig. 1A). The patient denied any history of trauma, surgery, or injection. No remarkable findings except for the skin lesion were observed. Ultrasonography showed a hyperechoic nodule (0.8×0.3 cm) in the subcutaneous layer; No internal vascularity, fistula, or sinus connection with the deep underlying structures of the neck was found (Fig. 1B). Histopathological examination after surgical excision showed a hyaline cartilage core in the dermis with isogenous chondrocytes, a glassy extracellular matrix and absence of elastic fiber, which characterize hyaline cartilage (Fig. 1C, D). A diagnosis of CCBR was confirmed, and the patient showed no recurrence during 9 months of follow-up.
CCBRs have been reported under numerous names, such as wattle, cervical auricle, accessory tragus, cervical skin tag, and congenital cartilaginous rests of the neck1. Several pervious authors identified CCBRs comprised of elastic cartilage, suggesting that CCBRs arise from ectopic auricular tissue2. However, Begovic et al.1 reported numerous cases of CCBRs comprised of hyaline cartilage. Because the second branchial arch can differentiate into both elastic and hyaline cartilage, the authors insisted that the origin of CCBRs is the second branchial arch. In addition, CCBRs are located in the middle or lower portion of the SCM and are deeply connected with the superficial fascia of the neck. CCBRs are considered a second branchial remnant disorder rather than an ectopic auricular migratory disorder3. Therefore, the use of particular terms such as cervical auricle and accessory tragus should be avoided.
Recent studies have revealed more detailed histological features of CCBRs. Large nerves and cluster of Pacinian corpuscles have been observed in the periphery of CCBRs4. Pacinian corpuscles are primary mechanoreceptors that are usually located in the deep dermis and detect gross pressure changes and vibration. Researchers in that study hypothesized that CCBRs attract sensory axons and neural crest cells that organize as Pacinian corpuscles.
CCBRs are often associated with numerous congenital anomalies; auditory, gastrointestinal, genitourinary, cardiovascular, musculoskeletal, and visual anomalies, as well as complex syndromes, occur in up to 76% of cases2. Thus, detailed additional examinations, such as abdominal and cardiac ultrasonography, are recommended for patients with CCBRs. However, the prevalence of associated anomalies varies greatly. Begovic et al.1 reported that 29% of CCBR patients exhibit anomalies. Compared to those in the studies of Atlan et al.2 and Begovic et al.1, all patients included in the study of Atlan et al.2 exhibited CCBRs composed of elastic cartilage. Meanwhile, Begovic et al.1 found that more than half of the patients in their study exhibited CCBRs composed of hyaline cartilage. Retrospective analysis revealed that among 11 cases of CCBRs composed of hyaline cartilage, only one case involved an associated anomaly (vesicoureteral reflux, which is common in normal neonates) (Table 1)135. Although the cause remains uncertain, the presence of hyaline cartilage in CCBRs can be considered a favorable marker, indicating a low possibility of associated anomalies.
This rare case involving a CCBR comprised of hyaline cartilage further supports the current knowledge regarding the embryogenesis and associated anomalies of CCBRs.

 XML Download
XML Download