

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Hypothyroidism is a common endocrine disorder with a prevalence of 2–3% in the general population.12) The therapeutic goal for hypothyroidism is to restore clinical and biochemical euthyroidism through adequate thyroid hormone replacement. The standard treatment of hypothyroidism is administration of levothyroxine (L-T4) to normalize the serum TSH level. This approach has been supported by the hypothesis that the deiodinase in peripheral tissues can produce adequate amount of active triiodothyronine (T3) from thyroxine (T4). Physiologically, only 20% of T3 is secreted by the thyroid gland, and 80% is produced by deiodinase from T4 in peripheral tissues. Furthermore, L-T4 has long half-life, allowing a once-daily dosing and stable T3 levels.34)
However, recent studies suggested that a significant proportion of patients treated with L-T4 monotherapy have persistent symptoms and complaints despite the normalized serum TSH levels.1567) This could be because the serum T3 levels might not be sufficiently normalized only with peripheral T4-T3 conversion.89)
The serum T3 level might be an important indicator for the treatment of hypothyroidism; however, the guidelines do not recommend measurement of the serum total T3 or free T3 (fT3) levels.34) The T3 levels vary with circadian changes or other illness, and the performance of assays used to measure the serum T3 level is known to be inadequate.4) However, recent progress in technologies, measurement of the serum T3 became more accurate.
In this study, we aimed to evaluate differences in thyroid hormone parameters and the relationships of these hormones after L-T4 treatment. We compare thyroid hormone levels between euthyroid L-T4 treated patients after total thyroidectomy and radioactive iodine (RAI) ablation therapy and euthyroid healthy control subjects. Thyroid hormones from patients who underwent total thyroidectomy and radioactive iodine ablation were solely from L-T4 and these patients might be good subjects for analyzing changes in thyroid hormones with L-T4 treatment. The serum free T4 (fT4) and fT3 levels were measured using two assay kits from two different companies for validation.
Materials and Methods
Study Subjects
We retrospectively reviewed medical records of patients who underwent total thyroidectomy and RAI ablation therapy and followed up in Asan Medical Center between August 2017 and September 2017. We found 70 euthyroid L-T4 treated athyreotic female patients with remnant blood samples in the clinical laboratory after measurement of requested blood tests from out-patient clinic. After excluding 1 patient who were treated by liothyronine and L-T4 combination treatment, 69 patients who treated L-T4 monotherapy were included in this study. We also retrospectively found 90 healthy female subjects with remnant blood samples as controls. All these subjects underwent routine health check-up in our hospital, and presented euthyroidism during the same period. We only selected subjects aged 20–80 years old and without any history of thyroid disease, taking any drug influencing thyroid function, other cancer, or any evidence of chronic/acute disease. Serum fT3 and fT4 levels were retrospectively analyzed in these subjects using remnant blood samples using two assay kits. Euthyroidism was defined as serum TSH levels in the reference range (0.4–5.0 mIU/L). The study was approved by the Institutional Review Board of our institution. Informed consent was waived due to retrospective nature of this study.
Laboratory Methods
Serum TSH levels were measured with an immunoradiometric assay (B·R·A·H·M·S TSH 1 RIA kit; B·R·A·H·M·SGmbH, Henningsdorf) with a functional sensitivity of 0.07 mU/L. Serum fT3 and fT4 levels were measured by using two different kits from two different companies, respectively. A functional assay sensitivity of kits from the company A (Kit As) was 1.0 pmol/L for fT3 and 2.34 pmol/L for fT4. A functional assay sensitivity of kits from the company B (Kit Bs) was 1.2 pmol/L for fT3 and 5 pmol/L for fT4.
Statistics
R studio (version 3.1.2) and the R libraries xlsx, lubridate, survival, car, psych and gdata were used to analyze the data (R Foundation for Statistical Computing, http://www.R-project.org/). Continuous variables are presented as medians with interquartile range (IQR) and Wilcoxon rank-sum test was used to compare variables. Log-transformed TSH values were used for statistical analysis. Intra-class correlation coefficient (ICC) was measured by two-way mixed model. ICC values <0.5, 0.5–0.75, 0.79–0.9, and >0.9 was considered as poor, moderate, good and excellent reliability, respectively.10) Non-linear relationships were tested using Kendall's tau rank correlation and non-linear relationship curves were fitted by local polynomial regression. Area under the curve (AUC) values showing each kit capacity to discriminate the patient group from the control group, were evaluated. All p-values were two-sided, and p value of <0.05 was considered statistically significant.
Results
Subjects Characteristics
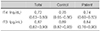
Characteristics for the control (n=90) and patient (n=69) are shown in Table 1. All subjects were female and the median age of patients was 55 years. All subjects showed euthyroidism and the median TSH level was 2.50 mIU/L (IQR 1.60–3.45). Age and TSH level was not different between controls and patients (p=0.139 and p=0.739). All 69 patients underwent total thyroidectomy with RAI ablation therapy due to papillary thyroid cancers and had no evidence of disease status during median 9.3 years of follow-up.
According to the Kit As, the median fT4, fT3 level and fT3/fT4 ratio of total study subjects was 1.5 ng/dL, 2.8 pg/mL, and 0.19, respectively. Serum fT4 level was significantly higher in patients (p<0.001). Serum fT3 level and fT3/fT4 ratio were significantly higher in controls (p=0.047 and p<0.001). According to the Kit Bs, the median fT4, fT3 level and fT3/fT4 ratio of total study subjects was 1.2 ng/dL, 3.6 pg/mL, and 0.29, respectively. Serum fT4 level was significantly higher in patients (p=0.046) and fT3/fT4 ratio was significantly higher in controls (p=0.009) but, serum fT3 level was not different between groups. Even though fT3 level was lower in patients, all fT3 levels in patients were in the manufacturer's recommended reference range.
When we evaluated ICC values of thyroid hormones according to the kits, serum fT4 levels presented moderate reliability and serum fT3 levels presented good reliability between different kits (Table 2).
Relationship between TSH and Free T3, Free T4, Free T3/Free T4 Ratio
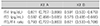
We evaluated the relationship between fT3, fT4, fT3/fT4 ratio and TSH in the control and patient group. As shown in Fig. 1, fT3 levels, measured by both the Kit As and Bs, presented an inverse correlation with TSH level (tau=−0.16, p=0.005 in Kit A and tau=−0.18, p=0.001 in Kit B). fT4 levels also inversely correlated with TSH level (tau=−0.11, p=0.046 in Kit A and tau=−0.13, p=0.026 in Kit B). However, fT3/fT4 ratio was not correlated with TSH level (tau=−0.03, p=0.584 in Kit As and tau=−0.03, p=0.598 in Kit Bs) (Table 3).
These relationships were different in the patient group from the control group. In the control group, serum fT3 levels was stable and not correlated with TSH level (tau=−0.10, p=0.18 in Kit A and tau=−0.06, p=0.40). Serum fT4 levels were significantly correlated with TSH level (tau=−0.16, p=0.049 in Kit A and tau=−0.16, p=0.034). However, in the patient group, only fT3 levels were significantly correlated with TSH level (tau=−0.22, p=0.012 in Kit A and tau=−0.31, p<0.001 in Kit B) (Table 3).
When we evaluated the AUC values of fT3, fT4 and fT3/fT4 ratio for discriminating the patient group from the control group in both kits, the Kit As presented higher values than Kit Bs in all thyroid hormone parameters (Table 4).
Discussion
In this in-depth analysis of thyroid hormones, we found significant differences in thyroid hormone parameters and the relationships of these hormones between euthyroid L-T4 treated athyreotic patients and euthyroid healthy subjects. Serum fT4 levels were significantly higher in athyreotic patients than controls. Conversely, serum fT3 levels were significantly lower in athyreotic patients than controls, which resulted in significantly lower fT3/fT4 ratio in athyreotic patients. This phenomenon was not different between two different kits. Our results are consistent with previous studies7811) and also suggested that peripheral T3 conversion from T4 might be insufficient for L-T4 treated athyreotic patients to maintain normal T3 levels.5812)
The relationship between serum TSH and fT4 or fT3 levels was also different between the patient group and the control group. In euthyroid healthy controls, serum fT3 levels were steady and only serum fT4 levels were inversely correlated with serum TSH level. However, serum fT3 levels were varied and inversely correlated with serum TSH level in euthyroid L-T4 treated athyreotic patient. These relationships also were not different between two different kits. These findings imply that maintaining stable T3 levels is important for healthy individuals and deiodinase activity might be positively correlated with serum TSH levels to maintain T3 levels in euthyroid healthy subjects as previously reported.5913) In athyreotic euthyroid patients, however, the relationship was not restored even with normal serum TSH levels from sufficient L-T4 treatment. Our findings suggest that L-T4 monotherapy might not be optimal replacement modality for some hypothyroid patients and suggest the possible advantages of low dose liothyronine combination with L-T4.56131415) Further well-designed prospective studies are needed to clarify the best management of post-operative hypothyroidism.
In euthyroid healthy subjects, not only fT3 levels, but also fT3/fT4 ratios were steady irrespective of TSH level. This finding suggests that fT3 level or fT3/fT4 ratio might be a reliable indicator of individual thyroid functional status in subjects with functional thyroid and suggest that post-operative serum fT3 level or fT3/fT4 ratio might be a helpful biomarker for discriminating patients who have problems in T4-T3 conversion. A previous study suggested that post-thyroidectomy serum fT3 levels of patients with mildly suppressed TSH levels were equivalent for the preoperative levels and those of patients with normal TSH levels were lower than preoperative levels.16)
Serum fT4 and fT3 values measured by two different kits presented moderate to good concordance but, the median fT4 levels were higher with Kit A and the median fT3 levels were higher with Kit B (p<0.001 and p<0.001, data not shown). When we compare thyroid hormones between patients and controls, thyroid hormones measured by Kit As presented more significant differences with higher AUC values for discriminating patients from controls than those measured by Kit Bs. These findings suggest that free thyroid hormone levels and their ratio might vary according to the assay methods and this way of comparison might be helpful for choosing appropriate assay kits to use.
There are some limitations in this study. First, the number of subjects in this study was small and only females were included in this study. In this study, fT4 in euthyroid athyreotic patients was not related with TSH, which is different from previous studies.813) This result might be biased due to small number of subjects. Second, we did not measured patient's well-being state or any biochemical parameters suggesting tissue thyroid function. As a result, we could not confirm the clinical significance of low and variable fT3 levels and could not find clinical features associated with low and variable fT3 levels in athyreotic patients. However, our study has an advantage in that we measured free thyroid hormone levels by two different assay kits at the same time. Differences in thyroid hormone parameters between the patients and the controls were similar irrespective of what assay was used and this validated our results.
In conclusion, serum fT3 levels were significantly lower and varied in L-T4 treated athyreotic euthyroid patients than euthyroid healthy controls. These findings suggest that L-T4 monotherapy might not be an appropriate replacement modality for some athyreotic patients to maintain optimal T3 levels. Future studies are needed to find a more physiological treatment for these patients but, our results suggest the possible role of low dose liothyronine combination with L-T4 as a better treatment for them.



 XML Download
XML Download