

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Skull base chordomas are rare, malignant tumors with incidence rate fewer than 0.1 per 100,000 inhabitants per year that arise from primitive notochord remnants of the axial skeleton and make up about 25–35% of all chordoma cases.1) Most cases of advanced chordoma are extraosseous, with lesions extending beyond osseous margins.2) Previous case reports have described chordomas as firm, meaty masses protruding from the posterior nasopharyngeal wall,3) but in the present case report, the gross findings revealed a nasopharyngeal chordoma with a soft, cystic appearance. This chordoma was treated with wide excision and post-operative radiotherapy. In this work, we report an unusual case of cystic nasopharyngeal chordoma found incidentally in a papillary thyroid cancer patient.
CASE REPORT
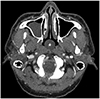
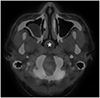
A 37-year-old male presented to the Thyroid Center with suspicious papillary thyroid cancer with neck metastasis and a known nasopharyngeal mass. The patient had no known underlying disease other than thyroid cancer, and no relevant family history was noted. A poorly vascularized cystic mass, approximately 2 cm in size and protruding from the midline of the posterior nasopharyngeal wall, was examined. There was no sign of inflammation or induration, and the tumor was covered in translucent mucosa (Fig. 1). The initial nasopharynx computed tomography (CT) scan revealed a well-circumscribed 2.2 cm cystic lesion in the nasopharyngeal midline with no enhancing solid material inside. The relationship between the tumor and clivus was equivocal in the axial scans of CT images. The imaging report indicated possibility of a benign lesion, such as Tornwaldt's cyst (Fig. 2). Preoperative positron emission tomography (PET)-CT scan taken for the work up for thyroid cancer revealed no unusual hypermetabolism in the nasopharynx (Fig. 3). A biopsy of the nasopharyngeal mass was planned along with total thyroidectomy. During the procedure, the cystic mass was noted to have its peduncle rooted in the midline of the posterior nasopharyngeal wall, while lacking adhesion to either lateral wall or the posterior septum. Biopsy was performed using grasping forceps, and the gelatinous content was sent for testing and was later proven to be consistent with chordoma. Post-biopsy follow-up CT and magnetic resonance imaging (MRI) scans of the nasopharynx showed residual chordoma with bony scalloping in the clivus (Fig. 4). In addition, reconstruction of the sagittal cut of the pre-biopsy CT scan clearly showed clival erosion that was ambiguous in axial view. Wide excision of the nasopharyngeal chordoma was planned for radical removal of the remnant tumor. An endoscopic navigation system was used to approximate the upper, lower, and both lateral margins of the remnant tumor. The antero-inferior walls of both sphenoid sinuses were removed, and posterior nasopharyngeal deep muscle was extirpated. Remnant tissues and bones were carefully drilled using the navigation system to secure a safe distance to the spine. Frozen biopsies were performed on samples from all four surrounding resection margins, and the results showed no tumor cells. A permanent biopsy revealed a chordoma with free resection margins. To treat possible residual tumor, the patient underwent radiotherapy on the postoperative nasopharyngeal tumor bed, with daily administration of 180 to 6,300 cGy in 35 fractions. Follow-up CT scan was taken (Fig. 5) and MRI, chest CT, and PET-CT scans of the nasopharynx are planned to check for local recurrence and distant metastasis.
DISCUSSION
Chordomas are rare, slow-growing, and malignant bony tumors that arise from remnants of the notochord.4) The clinical features of spheno-occipital or nasal chordomas vary depending on tumor extension and the involvement of surrounding structures. Patients may be asymptomatic or can present with symptoms ranging from mild nasal obstructions to severe headaches and cranial nerve palsies due to intracranial spread.1) The histopathologic features of chordoma include dark, giant, oval nuclei and vacuolated or granular eosinophilic cytoplasm, while immunohistochemical characteristics include strong positivity for the S-100 protein and epithelial membrane antigen.4)
Previous literature focusing on nasopharyngeal chordomas have described the tumors as pinkish or gray masses with a “meaty” appearance.3) However, in this case, the chordoma was found to have an unusually soft, yellowish, polypoid appearance like a cyst, but with gelatinous content. The differential diagnoses of nasopharyngeal cystic masses are quite diverse, and one possible consideration is Tornwaldt's cyst, a benign developmental lesion in the midline of the nasopharynx. Other possible pathologically distinguishable cystic lesions include dermoid cysts, epidermoid cysts, and teratomas. During embryological development, congenital inclusion of one, two, or three germinal layers may result in the formation of such cysts. Other differential diagnoses include retention cysts and intra-adenoid cysts, which are also often asymptomatic and incidentally found. The initial diagnosis of chordoma by nasoendoscopy alone is uncertain, and the cystic appearance in this case makes the clinical decision even more difficult. Even when encountering a cystic and benign-looking nasopharyngeal mass, an accurate health history, physical examination, and endoscopic biopsy are crucial before performing curative surgery.
Simultaneous double malignancies of chordoma with papillary thyroid cancer have not yet been reported. The two cancers have completely different disease entities but can often be mistaken for each other, as cervical chordomas can masquerade as thyroid neoplasms and thyroid cancer can metastasize to the skull base, mimicking clivial chordomas.5)6) Furthermore, there are reports of rare metastases of other cancers, such as prostate and hepatocellular carcinoma, to the clivus, which is an important part of distinguishing a clivial mass.7)
CT and MR imaging features may help to narrow down the possible differential diagnoses for nasopharyngeal mass to chordoma. Imaging work ups are essential before any surgery of the posterior nasopharyngeal wall to avoid resection of crucial structures such as brain. CT imaging of chordomas is crucial to determine bony involvement. MRI scanning is an excellent tool for delineating the tumor lesion from the surrounding anatomy. Chordomas have intermediate to low signal intensity on T1-weight MRIs and high signal intensity on T2-weight scans. Studies are yet to be conducted on use of PET-CT to diagnose chordoma, but there are reports of sacrococcygeal chordoma or metastatic chordoma to lung that show heterogeneously increased F-18 fluorodeoxyglucose (FDG) uptake.8) PET-CT of the case discussed here, however, showed no abnormal hypermetabolic lesion in the nasopharynx, suggesting a benign lesion. Low FDG uptake may be due to low cellularity and low number of mitoses, which are typical features in chordoma.9) The discrepancy between degrees of uptake in chordoma may be due to differences in the metabolism of tumors from different origins. Further research and case reports are needed to elucidate this relationship. To accurately evaluate a nasopharyngeal tumor, findings from multiple imaging modalities should be taken into consideration.
Surgical removal is an effective treatment for chordoma, and longer survival rates have been associated with more extensive tumor removal but the role of adjuvant radiation therapy is still unclear.10) Therefore, complete surgical excision with a free resection margin provides the most promising recurrence-free survival. Traditionally, extended open skull base approaches have been applied to achieve total resection of the clival tumor, but with advent of endoscopic practice, endonasal approaches have become an uprising alternative.11) In this case, the tumor was located in only midline of nasopharynx with minimal depth of invasion into clival bone, providing safe distance from vital structures such as carotid arteries and cranial nerves. This allowed endoscopic transsphenoidal approach with minimally invasive route to skull base.
Due to their rarity, nasopharyngeal chordomas are not often encountered and are difficult to diagnose even for expert rhinologists or radiologists. Taking into account the initial gross findings and CT reports, a benign neoplasm was determined to be more likely than a malignant one in this case. To make an accurate clinical decision, the findings of various imaging modalities should be considered. In addition, when a cystic nasopharyngeal tumor is encountered, the possibility of chordoma should be examined as a differential diagnosis.



 XML Download
XML Download