

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Thyroid cancer incidence has been sharply increasing worldwide during the last few decades.12) This is partially due to increased medical surveillance and the widespread use of highly sensitive diagnostic tools such as ultrasound (US) and fine-needle aspiration biopsy (FNA).1) However, the increased incidence of large papillary thyroid cancer cannot be explained solely by these reasons.3)
There are many potential risk factors for thyroid cancer such as ionizing radiation, history of thyroid cancer in first degree relatives, prior history of thyroid cancer, and a high calcitonin level.45) Recently, attention has been drawn toward obesity, which may be another potential risk factor for thyroid cancer, as there was a dramatic increase in the prevalence of both thyroid cancer and obesity during the similar period.36) Up to the present, the best level of evidence has been derived from a pooled analysis of prospective studies (n=848,932) showing that obesity is an independent risk factor for thyroid cancer (hazard ratio: 1.21 in men and 1.16 in women).7) This was also true in a health checkup setting with 15068 subjects and with FNA results of 1427 patients; the prevalence of thyroid cancer in women was associated with a high body mass index (BMI), per 5 kg/m2 increase (odds ratio [OR], 1.63; p<0.001).8) Along with high BMI, a high thyroid stimulating hormone (TSH) level was reported to be a risk factor for malignant thyroid nodules.91011) There was a positive association between BMI and TSH levels in a study that included euthyroid patients1213) as well as hypothyroidism patients.14)
Although association between thyroid cancer and high BMI or high TSH level has been reported, risk stratification of thyroid nodules detected on US follows the US feature of nodules. Therefore, the most important factor that determines the need for FNA is US features of a thyroid nodule, not BMI or TSH level. None of the previous studies have evaluated the association of high BMI or TSH levels with thyroid malignancy after adjusting for US features and it remains unclear whether these two potential risk factors would affect nodule selection for FNA. Therefore, the purpose of this study was to evaluate whether high BMI or TSH levels would affect the selection of thyroid nodules for FNA after US evaluation, an essential procedure for choosing an adequate treatment plan.
Materials and Methods
This retrospective study was approved by the institutional review board, and informed consent was waived. Informed consent for US-guided FNA was obtained from all patients prior to each biopsy.
Study Population
Among thyroid nodules that were biopsied in our institution from February 2006 through December 2008 (13,182 nodules in 12,028 patients), we selected 3698 nodules with the following criteria; nodules 5 mm or larger, nodules found in patients without thyroid hormone medication history, and those found in patients with information on height, weight, and TSH values available on medical records within three months from the day of FNA. Among the biopsied nodules, 3954 nodules were operated. Five hundred forty three nodules in 536 patients were excluded due to a lack of definitive cytologic or further pathologic diagnosis following surgery. In the study period, cytological reports were categorized as ‘benign’, ‘indeterminate’, ‘suspicious for papillary thyroid carcinoma’, ‘malignant’, or ‘nondiagnostic’.15161718) Definitive cytologic results for analysis included ‘benign’ and ‘malignant’. We excluded 230 nodules (42.4%) with nondiagnostic, 95 (17.5%) nodules with indeterminate, and 218 (40.1%) nodules with suspicious for malignancy cytologic results. Finally, 3155 nodules in 3005 patients were included as the study population.
Data Acquisition and Patient Grouping
Patients were grouped according to gender. Clinical information was systematically summarized and collected from electronic medical records by a 4th year resident and a trained employee who had worked in our radiology department for 5 years. The patients included in this study had records available of their height, weight, and serum TSH levels for each day of their outpatient clinic visits within three months from the day of FNA. The BMI was calculated (weight (kg)/height (m2)) using each patient's height and weight. Patients were assigned four grades according to BMI using the World Health Organization classification; underweight with BMI <18.5; normal with BMI 18.5 to 24.9; overweight with BMI 25 to 29.9, and obese with BMI ≥30.19) Our institution's TSH assay method altered from radioimmunoassay to IRMA method during the study period. Therefore, TSH levels were determined by radioimmunoassay (Trinity Biotech, Co. Wicklow, Ireland, reference range 0.4–3.1 µIU/mL) or IRMA (TSH-CTK-3, SORIN Biomedica, Saluggia, Italy, reference range 0.3–4.99 µIU/mL). The reference ranges of the two TSH level measurement methods were based on each company's recommendation. TSH values were classified into three levels, low (lower than reference range), normal (within reference range), and high (higher than reference range).
Ultrasound Evaluation and FNA
Images of US were obtained using 5–12 MHz linear transducers (HDI 5000 and IU-22, respectively; Philips, Bothell, WA, USA). Ultrasonographic features of the thyroid nodules that underwent US-guided FNA were recorded according to internal component, echogenicity, margin, calcification, shape, and vascularity (Appendix). Suspicious US features include marked hypoechogenicity, microlobulated or irregular margin, microcalcification, taller than wide shape. Nodules are considered ‘suspicious for malignancy’ if there is one or more of the above suspicious US features. Nodules with no suspicious US features are considered as ‘probably benign’. Based on US features, thyroid nodules were divided into two categories, ‘probably benign’ and ‘suspicious for malignancy’.20)
All FNA on thyroid nodules was done under US guidance. For FNA, a 23-gauge needle attached to a 2-mL disposable plastic syringe was used. In each nodule, aspiration was done twice or more and aspirated materials were expelled onto glass slides followed by smearing. All smeared glass slides were placed in 95% alcohol for Papanicolaou staining and the remaining material was rinsed in saline solution. After the glass slides of expelled aspirated material were moved to the pathologic department, they were interpreted by five experienced cytopathologists.
Statistical Analysis
Two sample t-tests were used to compare continuous variables including age, nodule size, height, and weight of patients in the malignant and benign nodule groups. The Chi-square test was used to compare categorical variables including BMI grade, TSH level, and US category in the two groups.
The OR with 95% confidence intervals (CI) of malignancy for each clinical and US feature was calculated with univariate and multivariate logistic regression analysis. As some previous studies showed a positive association between BMI and TSH levels, we analyzed their association.1321) We evaluated the association between BMI and TSH levels (both in multimodal distribution) by using cumulative logit link and it was not significant (p=0.318). Therefore, we included both BMI value and TSH level as independent variables in multivariate logistic regression analysis. After adjusting for all factors in the univariate analysis except for height and weight, which were used to calculate BMI, multivariate logistic regression analysis was performed to assess independent associations of thyroid malignancy with all clinical factors and US categories. To evaluate the effect of clinical factors on nodule selection for FNA, univariate and multivariate logistic regression analysis was done for nodules of each US category. We used logistic regression with GEE (generalized estimating equation) for clustered data. SAS ver. 9.2 (SAS Inc., Cary, NC, USA) was used for statistical analysis. A p value of less than 0.05 was considered significant for statistical analysis.
Results
Among 3155 nodules, 2663 nodules were in female and 492 nodules were in male. Among the nodules, there were 2159 benign and 996 malignant nodules. There were 2088 patients with benign nodules; 2017 patients had one benign nodule and 71 patients had two benign nodules. There were 933 patients with malignant nodules; 870 patients had one malignant nodule and 63 patients had two malignant nodules. Sixteen patients had both malignant and benign nodules; 15 patients had one malignant and one benign nodule and one patient had two malignant and one benign nodule.
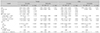
The number of nodules with each clinical and US feature is shown in Table 1. Patients with malignant nodules were significantly younger compared to patients with benign nodules in both genders (p<0.001). Malignant nodules had significantly smaller size in both genders (p<0.001). In both genders, the grades of BMI showed no significant difference between the malignant and benign groups (female, p=0.074; male, p=0.157). TSH levels were significantly different between the malignant and benign groups in both genders (p<0.001) showing a higher percentage of high TSH levels among the malignant group (12.6–23.9%) compared to the benign group (7.1–12.1%). The US ‘suspicious for malignancy’ category was significantly more frequent in the malignant group compared to the benign group in both genders (p<0.001).
In both genders, younger age and ‘suspicious for malignancy’ US category was significantly associated with malignancy on multivariate logistic regression analysis (Table 2). In females, a high TSH level (OR=1.010, p<0.001) and smaller nodule size (OR=0.999, p=0.044) also had significant association with malignancy on multivariate analysis. In males, low BMI (underweight; OR=1.145, p=0.025) was significantly associated with malignant thyroid nodules on multivariate analysis. In both genders, a low TSH level was significantly associated with decreased risk of malignancy (OR=0.766–0.896, p<0.001–0.012).
The results of multivariate logistic regression analysis for each US category are shown in Table 3. In ‘probably benign’ US category, younger age was significantly associated with malignancy in both genders. In females, smaller nodule was significantly associated with malignancy in ‘probably benign’ US category. In nodules with ‘suspicious for malignancy’ US category, younger age was significantly associated with malignancy in both genders.
Regarding BMI grade, it did not show any significant association with malignancy in females in both US categories. In males, low BMI was significantly associated with malignancy among nodules with ‘suspicious for malignancy’ US category. Regarding TSH levels, high TSH level was significantly associated with malignancy in females in ‘suspicious for malignancy’ US category, but not in males. In both genders, low TSH level was significantly associated with decreased risk of malignancy in ‘suspicious for malignancy’ US category.
Discussion
In this study, malignant thyroid nodules were significantly associated with ‘suspicious for malignancy’ US category in both genders on multivariate analysis. In terms of TSH and BMI, there were different results according to the gender on multivariate analysis. High TSH levels in females and low BMI grades in males were significantly associated with malignancy. However, when we evaluated the association of thyroid malignancies according to US category, neither a BMI grade nor a TSH level was significantly associated with malignancy in nodules with the ‘probably benign’ US category. On the other hand, a high TSH level in females and a low BMI grade in males were significantly associated with malignancy in nodules with the ‘suspicious for malignancy’ US category. Therefore, neither a BMI grade nor TSH levels have additional value in the selection of thyroid nodules for FNA after adequate categorization with US. These results are important because, to date, although the significant associations between malignancy and BMI or TSH levels have been studied,78910) there has been no study showing whether different approaches are needed for patients with BMI or TSH levels when performing FNA.
Before multivariate analysis was done to evaluate clinical factors and malignant thyroid nodules, we performed the interaction test between BMI and TSH because a high BMI and TSH level have been shown to have positive association with thyroid malignancy.121321) It is well known that TSH is related to the energy metabolism of the body,22) and perhaps due to the higher prevalence of hypothyroidism in obesity, there are early studies showing increased TSH levels in patients with high BMI.1423) However, in our study, there was no significant association between BMI values and TSH levels, i.e., increasing BMI values and high TSH levels did not show significant association. Therefore, it was possible to include both BMI grade and TSH level as confounding factors in multivariate analysis to evaluate their association with malignant thyroid nodules.
The association between high BMI, TSH level, and risk of thyroid cancer cannot be explained in a simple manner. One proposed mechanism is explained by the role of leptin, which is an adipokine and known to be related to obese patients.24) Elevated leptin levels will increase susceptibility to thyroid autoimmunity, which can lead to hypothyroidism and elevated TSH levels.25) Another main mechanism is explained by insulin resistance in obese patients.26) Insulin resistance, which is also related to diabetes mellitus, increases the insulin level in obese patients. Insulin can promote the secretion of regulatory factors including adipocytokines and TSH.26) In either of the suggested mechanisms, a high BMI will lead to a subsequent elevated TSH level and the increased amount of TSH stimulates the production of thyroid hormones and influences the growth and differentiation of thyroid cells.27) The positive association between a high TSH level and increased risk of thyroid cancer28) and its aggressiveness29) have been revealed. Recently, therapeutic strategy for thyroid cancer by means of controlling obesity with a drug has also been studied in mouse models.30)
TSH stimulates the production of thyroid hormones and supports thyroid growth.27) Although it is still controversial, some conclude that TSH receptor stimulation is related to the increased incidence and aggressiveness of thyroid cancer,29) and there are reports that a high TSH level was significantly associated with thyroid malignancy.910) On the other hand, suppression of TSH prevents the growth of thyroid nodules.31) In our study, although it was not a significant factor in determining nodules for FNA, a high TSH level was significantly associated with malignancy in both univariate and multivariate analysis.
In a previous study, a low TSH level was associated with a lower risk of thyroid malignancy.32) According to our results, low TSH levels were found to decrease risk of malignancy in both genders. There were 14.7% (318/2159) of benign nodules with suspicious US features in our study, therefore, if we can exclude those nodules for FNA, it will decrease the number of unnecessary FNAs. Further studies are needed to show the association between low TSH levels and lower risk of thyroid malignancy combined with US features of thyroid nodules.
Our results showing significant association between underweight (i.e., a low BMI grade) and thyroid malignancy in males is novel and not yet recognized. Most of the studies showing association between low BMI and cancer regards low BMI factor as a poor prognostic factor after surgery.3334) Still, in contrast to high BMI and cancer, there is a lack of report showing positive association between low BMI and malignancy. However, a recent study with a large cohort showed underweight was significantly associated with increased risk of breast cancer in premenopausal women.35) Since number of males with low BMI was limited in our study, the relationship between thyroid malignancy and low BMI in males warrants further confirmation.
According to our results, smaller nodules were associated with malignancy in females. There are contradictory results regarding the thyroid nodule size and the risk of malignancy. Some studies show consistent result with ours, showing inverse relationship between the thyroid nodule size and risk of malignancy.3637) Still, other studies reported that a larger nodule is associated with higher risk of malignancy.3839) The higher malignancy rate in smaller nodules in our study could be related to higher rate of FNA on smaller nodules with suspicious US feature. There were some limitations to our study. First, there is an inevitable selection bias in our study. If a patient did not undergo surgery after FNA with inconclusive cytological results (indeterminate, suspicious for papillary thyroid carcinoma, or nondiagnostic), those nodules were excluded from the study subjects. Second, there is a possibility of false-negative or false-positive results for the thyroid nodules, as we included FNA cytological results, not surgical pathology, of malignant and benign nodules. However, we cannot attribute the potential misinterpretation of the results to false results on FNA, as previous studies conducted in our institution showed a relatively low rate of false-negative (1.9–3.2%) or false-positive (1.9%) results.1640) Third, there was a relatively small number of obese patients (3.23%, n=102) in our study population, which may limit the hazard assessment of the various factors. Different results may be found in other study populations with a higher proportion of obese patients such as in western countries. Lastly, there were two different methods for TSH assay and associated two different reference levels for normal TSH level. According to a previous study, although the two assay methods well correlate with each other, IRMA was more sensitive than radioimmunoassay.41)
In conclusion, although there were more malignant thyroid nodules in patients with a high BMI grade or high TSH level, high BMI and high TSH levels were not significant factors in the determination of thyroid nodules for FNA when considered with US features.


 XML Download
XML Download