

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Papillary thyroid carcinoma (PTC) is the most common type of thyroid malignancy.12) The surgical removal has been accepted as the mainstay of its treatment and radical resection includes both complete removal of the diseased thyroid gland and metastatic lymph nodes.3) Regional lymph node metastasis are frequent at initial diagnosis of PTC, the role of therapeutic lymph node dissection is well established in clinical N1 disease.4) Less resection of lymph nodes and higher proportion of metastatic node per dissected lymph node are known risk factor for poorer prognosis in PTC.56789) However, in clinically N0 patients, there are conflicting data about effects of prophylactic lymph node dissection on long-term outcome, especially in central compartment area.451011) Moreover, the impacts of lymph node yield (LNY) and lymph node ratio (LNR) of prophylactic central compartment neck dissection (CCND) on the prognosis of PTC still remain controversial.6891213) Therefore, we evaluated the relationship between nodal factor and the recurrence free survival (RFS) of prophylactic CCND in large-scale PTC cohort.
Materials and Methods
Patients
A total of 2604 patients underwent thyroid surgery at Seoul St. Mary's Hospital, College of Medicine, the Catholic University of Korea, from 2009 to 2012. The management of thyroid cancer was determined in according to the guidelines issued by the American Thyroid Association.14) In our institution, prophylactic ipsilateral CCND was performed in all thyroid cancer patients and bilateral pCCND was selectively performed in bilateral thyroid cancer and/or in advanced primary tumor. In this study, we excluded non-classical variants such as follicular variant, tall cell variant, or diffuse sclerosing variant from this study and only patients with classical PTC by the final histologic report were enrolled. Additionally, we excluded the patients who underwent the therapeutic lymph node dissection for clinical N1 disease. Patients who were suspected of malignant lymph nodes in the central compartment or lateral neck on the pre-operative examination were also excluded. For analysis of nodal factor, the patients with minimum of one node was examined at final histology were enrolled.
Finally, we retrospectively reviewed 1754 patients of classic PTC who underwent thyroidectomy with pCCND by a single surgeon (Ja Seong Bae, MD, PhD). All patients took levothyroxine for thyroid stimulating hormone suppression postoperatively. Radioactive iodine therapy was performed 6 to 8 weeks after total thyroidectomy, based on risk factors according to the ATA guidelines.14) Serum thyroglobulin levels and neck ultrasonography were regularly checked during follow-up. The histologic report was revised according to AJCC 8th edition. The study protocol was approved by our Institutional Review Board (KC19RESI0015).
Nodal Factors
To focus on the effect of nodal factor on RFS, patients were divided into unilateral pCCND and bilateral pCCND groups. In unilateral pCCND, ipsilateral para-tracheal, peri-thyroidal and pre-tracheal lymph nodes were included, and sometimes, delphian node was included. Bilateral pCCND included pre-tracheal, both para-tracheal and peri-thyroidal node, and delphian node and occasionally para-esophageal lymph node. The LNY is the total number of lymph nodes removed and LNR was defined as a ratio of the number of metastatic lymph node (MLN) to LNY. In regarding the cutoff of nodal factors, patients were categorized as low/high MLN, LNR and LNY group, respectively.
Statistics
The groups were compared using the χ2 test, the Mann-Whitney U test, the Student's t test, or Fisher's exact test for qualitative or quantitative variables, as appropriate. Receiver operating characteristic curve analysis (ROC) curves and area under curves (AUC) were used to determine the cut-off values of nodal factors including LNY, LNR and MLN. The univariate and multivariate cox regression analysis were used statistically to analyze the factors affecting RFS. Kaplan-Meier survival analysis was used to compare RFS data between different groups. All Data were analyzed with SPSS 18 and p<0.05 was considered statistically significant.
Results
Clinicopathologic Characteristics
A total of 1754 patients, 1195 patients underwent thyroidectomy with unilateral pCCND and 559 patients underwent total thyroidectomy with bilateral pCCND (Table 1). The median follow up duration was 81.5 months (range 0–120). Mean age was 45.9 years old and 1325 (75.5%) patients were younger than 55 years at diagnosis. In unilateral pCCND group, 746 (62.4%) patients underwent total thyroidectomy. In cases of bilateral pCCND group, all patients underwent total thyroidectomy. Mean tumor size was 0.8±0.5 cm. A total 754 (43.0%) patients showed central neck node metastasis, of these, 410 (34.3%) patients were unilateral pCCND group and 344 (61.5%) patients were bilateral pCCND group. Mean MLN was 1.3±2.4, 0.8±1.6, 2.4±3.2 in entire study group, unilateral pCCND and bilateral pCCND, respectively. The mean LNY was 6.4±4.0 in unilateral pCCND group and 12.8±6.6 in bilateral pCCND group. In the aspect of LNR, mean LNR of unilateral group was 0.14±0.25 and mean LNR of bilateral group was 0.2±0.24. A total 45 patients (2.57%) showed recurrent disease during follow-up. Of these, 19 patients underwent bilateral pCCND and 26 cases were unilateral pCCND. The RFS was 18.7 (3–69) months in bilateral pCCND group and 21.8 (4–78) months in unilateral pCCND. In bilateral pCCND group, recurrence was found in the lateral neck nodes except one patient with thyroid bed recurrence. Among the 26 recurrent patients with unilateral pCCND, 19 patients had recurrence on their lateral neck area, three patients had recurrence on their contralateral thyroid lobe. Three patients showed recurrences at contralateral central node area without dissection at initial surgery and only one case showed recurrence in ipsilateral thyroid bed which was dissected at initial surgery.
Nodal Factors
The cutoff value of nodal factor was described in Table 2. In the unilateral CCND group, these values were LNY 5.5 (AUC=0.624, specificity=0.654, sensitivity=0.463), LNR 0.15 (AUC=0.683, specificity=0.615, sensitivity=0.732) and MLN 0.5 (AUC=0.695, specificity= 0.654, sensitivity=0.664), respectively. In bilateral pCCND group, the cutoff value of LNY was 10.5 (AUC=0.584, specificity=0.632, sensitivity=0.396), that of LNR was LNR 0.3 (AUC=0.806, specificity=0.789, sensitivity=0.739) and that of MLN was 4.5 (AUC=0.770, specificity=0.632, sensitivity=0.813), respectively. According to these cutoff values, we categorized the groups according to the criteria as low and high group (Table 3). In the unilateral pCCND group, 410 (34.3%) patients were high MLN group. A total 633 (53.0%) unilateral pCCND patients were assigned as high LNY and 329 (27.5%) were grouped as high LNR. In bilateral pCCND group, 113 (20.2%) patients were high MLN group and 338 (60.5%) patients were high LNY, 156 (27.9%) were assigned in high LNR.
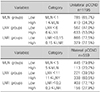
Univariate and Multivariate Cox Regression Analysis in Unilateral CCND Group (Table 4)
The univariate and multivariate cox regression analysis was performed to examine the factors affecting RFS in the unilateral CCND group. Gross extrathyroidal extension, high MLN and high LNR showed statistically significant correlation on RFS (hazard ratio [HR] 16.695 [4.754–58.628], p<0.0001, 3.587 [1.599–8.049], p<0.002 and 4.207 [1.909–9.272], p<0.0001, respectively). However, age, sex, the extent of thyroidectomy, tumor size category and LNY was not statistically significant. In multivariate cox regression, gross extrathyroidal extension (HR 13.056 [3.687–46.238], p<0.0001) and high LNR (HR 3.979 [1.785–8.867], p=0.001) were independent risk factor of recurrence.
Univariate and Multivariate Cox Regression Analysis in Bilateral CCND Group (Table 5)
In univariate cox regression analysis of bilateral pCCND group, larger tumor size, minimal extrathyroidal extension showed statistical correlation on RFS. In regarding nodal factors, high MLN and high LNR were statistically significant factors for RFS in univariate cox regression analysis (HR 3.587 [1.599–8.049], p=0.002 and HR 10.216 [3.390–30.783], p<0.0001). However, LNY had no statistically significant effect on RFS. In multivariate analysis, tumor size between 2 cm and 4 cm (HR 9.689 [2.722–34.485], p<0.0001) and multifocal tumor (HR 2.829 [1.053–7.601], p=0.039) were independent variables. High LNR remains an independent variable among nodal factors in bilateral CCND group (HR 8.192 [2.699–24.862], p<0.0001).
Recurrence Free Survival According to LNR Groups
In unilateral pCCND group, patients with LNR <0.15 showed 109.0 months in RFS and those with LNR ≥0.15 did 104.5 months in RFS in unilateral pCCND group (p<0.0001, Fig. 1A). In bilateral pCCND group, the estimated RFS of patients with LNR <0.3 was 107.1 months and that of patients with LNR ≥0.3 was 98.9 months (p<0.0001, Fig. 1B).
Discussion
PTC usually spreads via lymphatic channels, cervical lymph node metastasis is common.1) Lymph node metastasis at initial diagnosis was up to 40–60% of all patients in various studies.14151617) Similarly, in this study, a total 754 (43.0%) patients showed central neck node metastasis. Regional lymph node metastasis in cases with clinical presentation, larger metastatic node than 3 cm and multiple metastatic lymph node (N>5) was associated with recurrence.4) However, routine lymph node dissection was not recommended in all PTC patients due to minimal effect on survival and issues about complication.4) According to American thyroid Association guidelines, CCND with therapeutic intent in clinically involved central node was recommend and prophylactic nodal dissection only was recommended in advanced primary tumor.4) Nevertheless, lymph nodes in the central compartment were difficult to evaluate accurately in preoperative imaging studies due to thyroid gland and air-filled trachea.1819) In a similar view, 116 (6.6%) cN0 patients (36 [3.0%] patients in unilateral pCCND and 80 [14.3%] patients in bilateral pCCND) showed more than 5 metastatic node which were classified ATA intermediate risk group.4)
The impacts of pCCND on the prognosis of PTC were controversial. Some researchers suggest pCCND may convert clinical N0 patients to pathologic N1a, and it results upstaging and may lead overtreatment without definite survival benefit.414) Other studies demonstrated higher morbidity of pCCND including transient/permanent hypoparathyroidism and recurrent laryngeal injury with no improvement of prognosis.41420) Some researchers reported that pCCND reduced local recurrence.10112122) Furthermore, prophylactic node dissection has been suggested to reduce post-treatment serum Tg levels and to improve disease specific survival.51021) Furthermore, preoperative evaluation of According to guideline of Japanese Association of Endocrine/Japanese Society of Thyroid Surgery, pCCND was generally performed due to it reduced recurrence rate on central compartment area and prevented the inevitable increase in complication from secondary surgery.22) In this study, only 45 cases (2.57%) showed recurrence among 1754 patients and the recurrence rate was very low. Additionally, most recurrences were found in the lateral neck area of the lesion side. Only five had recurrence at the central compartment area, of these, only two patient showed recurrences in which was already dissected at initial surgery.
In regarding nodal factors, various variables were considered. Numbers of metastatic lymph node were known to be a significant risk factor for recurrences. 2324252627) Current staging system is divided nodal status into a binary form (N0 vs. N1), however, revised ATA guideline reflected the number and size of metastatic nodes at initial risk stratification.4) Park et al.24) reported the cutoff of MLN as 3 in total thyroidectomy and bilateral CCND in N1a patients and Randolph et al.28) reported the cutoff of ≥5 in based on various previous reports. In this study, we used ROC curve to determine the cutoff of MLN which could predict recurrence best in unilateral and bilateral pCCND separately. In unilateral pCCND, patient with more than one metastatic node showed significantly higher recurrence than patients without nodal metastasis. In bilateral pCCND, the highest sensitivity/specificity was achieved in cutoff of ≥5 metastatic lymph nodes. High MLN showed significant correlation on RFS in both unilateral and bilateral groups in univariate analysis, however, this correlation was no longer observed in multivariate analysis.
LNY was the total number of lymph node dissected during surgery, and it was used to assess the adequacy and completeness of node dissection.25) Many researchers tried to find optimal node yield in PTC, however, there was no relevant cutoff point for minimum value of node to be dissected, especially in pCCND.2529) Similarly, we hypophesis that high LNY might reduce local recurrences. For accurate analysis, we divided pCCND into unilateral and bilateral and set the each cutoff of LNY by ROC curve. LNY cutoff was 6 in unilateral pCCND and 11 in bilateral pCCND, but low/high LNY did not show a statistical difference in RFS. It might because the more advanced the primary tumor was, the surgeon performed node dissection more completely. In fact, LNY showed positively associated trend with MLN in this study (Data no shown). Additionally, LNY could be influenced by not only surgeon factor but also by pathologic examination and combined disease such as thyroiditis.25) Lymphadenopathy is common in autoimmune thyroiditis, it leads surgeon to perform more extensive nodal dissection when thyroiditis is accompanied with PTC.30) A total 423 (24.1%) showed combined autoimmune thyroiditis, of these 195 (34.9%) patients was bilateral pCCND groups. Thyroiditis showed a significant correlation with LNY and LNR (data not shown), but thyroiditis itself did not show a significant correlation on RFS in both unilateral and bilateral pCCND.
Regarding nodal factors, it is noteworthy that only LNR of nodal factors remains an independent variable in multivariate analysis. LNR was the ratio of numbers of proven metastatic node to dissected total lymph node (MLN/LNY). LNR has recently attracted the spotlight because it represented surgery quality in terms of adequacy of nodal dissection (LNY) and quantitative aspect in terms of the amount of metastatic lymph nodes.27) A large number of MLN or a small number of dissected nodes result in a high LNR. In previous reports, the cutoff of LNR varied between 0.11–0.86.8,24252627) These discrepancies might arise because of different surgical intent (prophylactic versus therapeutic nodal dissection), different extent of lymphadenectomy (central compartment versus lateral neck area) and different nodal status (occult versus clinical metastasis). In this study, cutoff of LNR was 0.15≤LNR in unilateral pCCND and 0.3≤LNR in bilateral pCCND, and the reason of relatively lower cutoff of LNR than previous reports might be because the study population was limited to pCCND group in clinically N0 patients.4242526)
This study has several limitations. First, it is retrospective study of single surgeon's experiences in a single tertiary institution. However, on the other hand, single-surgeon, single-institution nature of this study could limit the bias associated with surgeon and pathologist factors. Second, even though this is large scaled study, the numbers of recurrent events are relative small to assess optimal cutoff and correlation of nodal factor on RFS. A multicenter study with high volume center will increase the sample size and achieve statistical significance of various nodal factors.
In conclusion, in regarding nodal factors including MLN, LNY and LNR, high LNR was only independent risk factor to worse RFS in both unilateral and bilateral pCCND in cN0 PTC patients.





 XML Download
XML Download