

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Rheumatoid arthritis (RA) is the most common form of inflammatory arthritis. It changes biomechanical properties of bones and leads to alterations in bone components.[1] Bone loss due to pharmacologic treatment and physical impairment in RA patients can result in osteoporosis and related fractures.[23]
Although the prevalence of osteoporosis in patients with RA depends on patient characteristics, the prevalence of osteoporosis usually ranges from 15% to 59%.[456] It has been reported that the prevalence of osteoporosis in RA is generally higher than that in the general populations.[7] Although several studies have persistently reported that incidences and risk factors of osteoporotic fractures in patients with RA are higher than those in the general population, only a few studies have investigated the proportion and prognosis of RA patients among osteoporotic fractures in the general population.
Since February 2009, RA has been classified as a rare disease with insurance coverage by National Health Insurance (NHI) of Korea. Patients with RA are reimursement for 90% of the total cost. However, patients with RA should be confirmed by hematology (seropostive RA facter or anti-cyclic citrullinated peptide antibody). They should receive specific code of rare disease to have insurance coverage.
This retrospective observational study was designed as a nationwide population study using database from NHI Service (NHIS) of Korea. The purpose of this study was to investigate incidence and mortaltiy of osteoporotic fractures (including hip, spine, distal radius, and proximal humerus) in RA patients and compare them with those in the genearal population.
METHODS
This retrospective study was approved by ethics committee and weaved informed consents (NHIS-2018-4-007).
1. Subjects
Patients aged 50 years or older with osteoporotic fractures including spine, hip, distal radius, and humerus were identified from the nationwide database provided by NHIS of South Korea between 2010 and 2012.
The Korean NHI program covers 100% of the population with exception of cosmetic surgery and services for traffic accident. All clinics and hospitals submit patient's data including the diagnosis (as defined by the International Classification of Diseases, 10th revision [ICD-10]) and medical costs for claims to the NHIS. NHIS database has advantage for studying non-traumatic osteoporotic fractures because it does not include high energy injuries such as traffic and industrial accident. All information about the patient and disease is available from NHIS data. These data have been used in several epidemiologic studies in Korea.[8]
In this study, diagnostic codes including ICD-10 code and operational definition for hip, spine, distal radius, and humerus fracture were based on previous epidemiologic studies.[910111213]
Patients with RA were identified by the specific code for seropositive RA (V.223) with confirmed hematology (seropositive RA factor or anti-cyclic citrullinated peptide antibody).
1) Incidence of osteoporotic fractures in patients with RA
From 2010 to 2012, annual incidence rates of osteoporotic fractures were calculated using the annual number of osteoporotic fractures divided by mid-year population estimate. Incidence of osteoporotic fracture during period of 2010 to 2012 was also calculated.
2) Mortality and standardized mortality ratio (SMR) after osteoporotic fractures in patients with RA
NHIS data were merged with national mortality data from the National Statistical Office to determine the survival of each patient in the first year after osteoporotic fracture. One-year mortality rate of patients with osteoporotic fractures during the study period was calculated and presented in 10-year age intervals. In order to find excess mortality after osteoporotic fracture, SMR was calculated and presented in 10-year age interval.[1014] Age and gender distribution as well as mortality data of the Korean population in 2010 to 2012 were used as standard. They were obtained from the Korean Statistical Information Service. Excess mortality was considered when SMR was greater than one.
2. Statistical analyses
Average incidence rates, mortality rates, and SMRs of osteoporotic fractures and patients with RA considering age and gender in 10 year interval were calculated. All database management and analyses were performed using SAS statistical package version 9.4 (SAS Institute, Cary, NC, USA).
RESULTS
1. Incidence of osteoporotic fractures in patents with RA
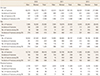
Osteopororic fractures in the general population and RA patients were increased by 11.6% and 17.4%, respetively, from 2010 to 2012 (195,271 and 1,356 in 2010; 217,985 and 1,592 in 2012, respectively) (Table 1 and Fig. 1). In terms of gender-specific distribution of osteoporotic fractures, similarly to osteoporotic fractures in the general population, incidence of osteoporotic fractures in men with RA was lower than that in women with RA. However, mean incidence of osteoporotic fractures in RA patients was 2.3 times higher in men and 1.4 times in women than that in the general population during 2010 to 2012 period (Table 1). Considering anatomical distribution of osteoporotic fractures in RA patients, incidence rates of hip, spine, and proximal humerus fracture in RA patients were higher than those in the general population. However, incidence of distal radius fractures in RA patients was similar to or lower than that in the general population.
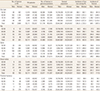
The mean age-specific incidence of osteoporotic fracture in RA patients increased from 932.1/100,000 for those aged 50 to 59 years to 9,377.0/100,000 for those aged ≥80 years in women and from 306.1/100,000 for those aged 50 to 59 years to 3,700.9/100,000 for those aged ≥80 years in men (Table 2). Osteoporotic fracture rates of both genders showed similar patterns. They were increased substantially for those older than 70 years. The incidence of osteoporotic fractures in women was increased more rapidly than that in men (Table 2). Regarding anatomical distribution of osteoporotic fracture in RA patients, although age-specific incidence rates of hip, spine, and proximal humerus fracture showed increasing trends in both genders, wrist fractures in women was decresased for those aged ≥80 years (Fig. 1).
2. Mortality and SMRs after osteoporotic fractures in patients with RA
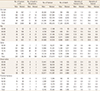
Cumulative mortality rate at first year after osteoporotic fracture in patients with RA was higher than that in the general population (7.8% in RA and 6.6% in the general population). Regarding gender specific distribution, average 1-year mortality rates in the general population and RA patients were 14.2% and 19.7% in men and 4.6% and 6.2% in women, respectively. Mortality rates of RA patients were 1.2 times higher in men and 1.3 times higher in women than those in the general population. Although cumulative 1-year mortality rates of all types of osteoporotic and spine fractures in both genders of RA patients were higher than those in the general population, those of hip, humerus, and distal radius fractures in RA patients were similar to or slightly lower than mortality rates in the general population (Table 3).
Average SMRs of osteoporotic fractures in those who aged 50 years or more in both groups were higher than general population. SMRs of osteoporotic fractures in RA patients for those in their 60s were the highest in both genders. SMR of osteoporotic fracture in RA patients was 1.4 times higher in men and 1.3 times higher in women. In assessment of gender-specific differences, SMR in men with RA was higher than that in women with RA (Table 4).
DISCUSSION
The objective of the current study was to invsestigate the incidence and mortaltiy of RA patients with osteoporotic fractures, including hip, spine, distal radius, and proximal humerus, and compare them with those in the genearal population (matched for gender and age) from 2010 to 2012. Using data from KNHIS, our results demonstrated that the number of osteopororic fracture in RA patients was increased by 17.4% over 2010 to 2012 period. Incidence of osteoporotic fracture in RA patients was 2.3 times higher in men and 1.4 times higher in women than that in the general population for the period of 2010 to 2012. Although crude mortality and SMR of osteoporotic fracture in RA patients were higher than crude mortality and SMR of osteoporotic fracture in the general population, those of individualized type of fractures (including hip, distal radius, and proximal humeurs) were diverse compared to those in the general population.
Although many studies have reported the high risk of osteoporosis and related fracture in patients with RA, comprehensive studies on the incidence and mortality of osteoporotic fracture in patients with RA are limited due to relatively small number of RA patients.[7151617] In this retrospective observational study, mean incidence of osteoporotic fractures in those aged 50 years and older was 2,453.8/100,000 (1,363.5 in men and 2,733.3/100,000 in women) in RA patients and 1,287.4/100,000 (584.1/100,000 in men and 1,897.5/100,000 in women) in the general population. Most fracture studies regarding the incidence of fractures in RA patients have reported reults with short-term or long-tern follow-up.[1181920] Kim et al.[21] have reported that, of 3,557 RA patients with a mean follow-up of 18 months, there are 152 osteoporotic fractures, including vertebrae, clavicle, humerus, wrist, femur, and ankle fractures. The estimated incidence of osteoporotic fracture was 2,926.3/100,000 person-year. Female RA patients had higher incidence of fractures than male RA patients (3,061.9 in females vs. 2,125.7 in males per 100,000 person-years).[21] Kim et al.[1] have performed a retrospective cohort study using a health care utilization database and reported that the incidence of osteoporotic fractures (including hip, pelvis, wrist, and humerus) is 9.6/1,000 (5.2/1,000 in men and 11.1/1,000 in women), which is 1.5 times higher than the rate in non-RA patients. Direct comparison for incidence of osteoporotic fracture between studies is difficult due to divergence in cohort characteristics, including age, gender, type of study, difference in follow-up periods, and various definitions of osteoporotic fracture.[118192021] In this study, incidence of wrist fracture in RA patients was lower than general population and it might be related with lower activity in RA patients. Despite these limitations, the incidence of osteoporotic fracture in RA patients is generally higher than that in the general population. In addition, women have higher incidence of osteoporotic fracture than men. These gender specific characteristics in RA patients are similar to those in the general populations.
Studies regarding mortality rate after osteoporotic fracture in RA patients are rare. Lin et al.[16] have reported that cumulative mortality rates at 6-month and 1-year follow-up are significantly higher among patients with RA (9.47% and 18.47%, respectively) compared to those in the control (8.47% and 13.62%, respectively). It is difficult to assess cumulative mortality after osteoporotic fracture in RA patients due to the small number of death. In this study, we calculated mean mortality rate of 3 years (2010–2012) due to a small number of mortality. Cumulative mortality rate after osteoporotic fracture in RA patients at 1 year follow-up was 19.7% in men and 6.2% in women. They were higher than those in the general population (14.2% in men and 4.6% in women). Although cumulative mortality after spine fracture in RA patients had similar pattern (higher than that in the generation pouplation), cumulative mortalities after hip, distal radius, and proxmial humerus in RA patients were similar to or slightly lower than those in the general population. Among osteoporotic fractures in both groups (RA patients and general population), mortality rate after hip fracture was the highest, followed by that after spine, proximal humerus, and distal radius fractures in order.[13142223] Mortality after spine fracture in RA patients was higher than mortality after hip fracture. This finding is different from mortality after osteoporotic fractures in general populations. It is possible to explain relatively young ages of RA patients and characteristics of cohorts.
This study has some limitations. First, this was a retrospecitve and cross-sectional study using nationwide claim database with possible selection bias. Second, this study defined RA patients as those who received specific code of rare disease while seronegative RA patients were excluded. Therefore, the incidence of fracture might have been underestimated. Finally, mortality rates of osteoporotic fracture in RA patients were compared to mortality rates of an age matched general population which included some osteoporotic fracture patients. This might potentially cause underestimation of excess mortality.


 XML Download
XML Download