

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Over the past decade, atypical femoral fracture (AFF) has been a serious issue related to treatment of osteoporosis.[12] Although the pathomechanism of AFFs has not been elucidated, many researchers have suggested that the occurrence of AFFs is associated with the alteration of bone material, accumulation of microfractures due to mechanical stress on the femur, and suppressed bone remodeling after long-term intake of bisphosphonates (BPs).[345678910]
Prefracture lesions of AFFs originate from the lateral femoral cortex, where large tensile stress generates during the gait cycle.[611] It has been suggested that AFFs represent the dichotomous distribution in the subtrochanteric and diaphyseal regions.[1213] In addition, there are several different influential factors between subtrochanteric and diaphyseal AFFs, such as age, race, and the presence of anterolateral bowing.[13141516171819] Among these, the presence of anterolateral bowing is considered the most important factor for the location of AFFs, because it significantly changes the mechanical stress distribution on the femur. While diaphyseal AFFs are known to be more associated with anterolateral bowing than subtrochanteric AFFs, it remains unclear how anterolateral bowing affects the fracture height of AFFs. Some authors have suggested that AFFs occur more distally as the bowing angle increases [2021]; however, we encountered some cases of AFF with severe femoral bowing that occurred in the apex of the curve, which was located in the middle one-third of the diaphysis and not the distal one-third (Fig. 1D).
To elucidate the effect of anterolateral bowing on the fracture height of AFFs, we separated the AFFs into 2 groups according to the presence of anterolateral femoral bowing (straight group and bowing group), and subsequently analyzed the fracture height of AFFs for each group. The aims of this study were 1) to evaluate the clinical and radiological features of AFFs in the straight group and bowing group; and 2) to determine which factors were associated with the fracture height of AFFs in the total cohort and each subgroup. The hypothesis of this study was that the presence of anterolateral bowing itself and the level of the apex of the bowed femur would be important factors for the fracture height of AFFs.
METHODS
1. Patients
From January 2005 to July 2017, 137 patients who underwent surgery for AFFs were identified. We confirmed that all patients met the 2013 revised case definition of the American Society for Bone and Mineral Research (ASBMR).[22] We excluded patients who did not have a whole femur radiograph of the pre-injured ipsilateral side or intact contralateral side (36 patients), as well as those who had severe asymmetry of both lower limbs due to previous surgery or disease (2 patients). As a result, 38 patients were excluded, and the remaining 99 patients were included. Bilateral cases (31 patients) were considered as one case to avoid weighted false results due to unnecessary duplication. In subsequent bilateral cases (10 patients), the first AFF was selected. In simultaneous bilateral cases (21 patients), especially where one femur was a complete fracture and the other was an incomplete fracture, we selected the side of the incomplete fracture in this analysis. Therefore, we analyzed 76 complete fractures (preinjury ipsilateral femurs in 26 patients and contralateral femurs in 50 patients) and 23 incomplete fractures (99 patients in total). This retrospective study was approved by our Institutional Review Board. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
2. Presence of anterolateral bowing
We separated the 99 patients into 2 groups according to the presence of anterolateral bowing (straight group vs. bowing group) using our previously reported anterolateral bowing grading system, which classifies the degree of bowing into 3 grades according to the position of the reference line on the most curved portion of the medial cortex (Fig. 1).[23] The reference line was drawn from the tip of the greater trochanter (GT) to the center of the intercondylar notch. When the reference line passed into the medial one-third of the medullary canal or more medially, the patient was classified into the bowing group, and the femur was graded as grades I–III femoral bowing according to its severity. One author separated the patients into 2 groups and senior author confirmed it subsequently. Therefore, 43 (43%) patients were classified into the bowing group, and the remaining 56 (57%) patients were classified into the straight group.
3. Clinical and radiological assessments
The following data were collected from the electronic medical record charts and radiographs: age at the time of injury, sex, weight, height, body mass index (BMI), location of the fracture (subtrochanter or diaphysis), bilaterality, bone mineral density (BMD), and history and duration of BP use. Subtrochanteric location was defined as a fracture within 5 cm below the lesser trochanter (LT). BMD data were available in 83 (84%) patients (48 for straight group and 35 for bowing group).
Radiological measurements were performed using a picture archiving and communication system. The anterior and lateral bowing angles, neck shaft angle (NSA), and fracture height from the GT were measured. The anterior and lateral bowing angles were measured as the angle between the bisecting lines of the proximal and the distal shaft using previously published methods.[21] The NSA was measured as the angle between the neck and shaft axes. The shaft axis was drawn using 2 landmarks: (1) the bisection point of a line drawn perpendicular to the shaft of the femur at the level just below the LT; and (2) 50 mm distally. These angles were measured from preinjury radiographs of ipsilateral or contralateral intact femur.
4. Measurement of the fracture height
Fracture height was assessed using the prefracture lesion on the preinjured ipsilateral standard anterior-posterior femur radiograph (49 patients). If this radiograph was unavailable, the postoperative ipsilateral standard anterior-posterior femur radiograph was used (50 patients). First, a reference line was drawn from the tip of the GT to the center of the trochlea, as in the aforementioned anterolateral bowing grading system. Two perpendicular lines to the reference line were then drawn at the tip of the GT and the distal end of the medial femoral condyle. The distance between these 2 perpendicular lines was considered as the entire femur length. A third perpendicular line was drawn at the fracture site. The distance from the tip of the GT to the third perpendicular line was considered as the fracture height. For an objective comparison of the distance, the measured distances were converted to a standardized ratio of the entire femur length, which has been used in previous studies (Fig. 2A, B).
5. Measurement of the estimated apex height
In the bowing group only, the estimated apex height was also measured on a standard anterior-posterior radiograph. The reference line used to grade the femoral bowing was moved parallel in order to touch the most curved (concave) site of the medial femoral cortex. Then, a perpendicular line to the reference line was drawn at the most curved site. The lateral cortex point where this perpendicular line reached was defined as the estimated apex. The estimated apex height was drawn using the same method to calculate the fracture height (Fig. 2C, D).
6. Statistical analysis
The clinical and radiological parameters were compared between the straight and bowing groups. For continuous variables, an independent 2-sample t-test was performed after assessing for normality, whereas for categorical variables, a χ2 test or the Fisher's exact test was conducted.
Linear regression models were used to estimate the association between fracture height (ratio) and all clinical and radiological variables. Exploratory univariable analysis was conducted using Pearson's correlation coefficient for continuous variables and the independent 2-sample t-test for dichotomous variables. Then multivariable linear regression analysis was performed and included the explanatory variables that were significant in the univariable analysis. The explanatory variables were height, presence of anterolateral bowing, and lateral bowing angles for the total cohort; weight and lateral bowing angle were included for the straight group; anterior bowing angle, lateral bowing angles, and the estimated apex height (ratio) were included for the bowing group. Multicollinearity was used to explore post-regression with the variance inflation factor. Significance for all tests was set at a P-value <0.05. All statistical analyses were performed using SPSS Statistics, version 23 (IBM Corp., Armonk, NY, USA).
RESULTS
1. Distribution of the fracture height of AFFs
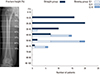
In the straight group, 64% of AFFs occurred at the level of the LT and subtrochanteric area (within the range from 10% to <30% of the femoral length from the GT). The remaining 36% of AFFs were distributed throughout the diaphysis, with decreasing prevalence from the proximal to distal diaphysis. However, all locations of AFFs in the bowing group were in the diaphyseal area, mostly within the range from 40% to <60% of femoral length from the GT (Fig. 3). The anterolateral bowing grade was not related with the fracture height of AFFs in the bowing group (Kruskal-Wallis test, P=0.540).
2. Comparison of clinical and radiological characteristics between the straight group and bowing group
The patients in the straight group were younger, heavier, and taller, and had a higher BMD than those in the bowing group. Additionally, the location of the fracture (subtrochanter or diaphysis) was significantly different between the groups. There were no significant differences in sex, BMI, bilaterality, history of BP use, and duration of BP use between the groups (Table 1).
The average anterior and lateral bowing angles were significantly higher in the bowing group than in the straight group (P<0.001, both). The average fracture height from the GT (mm) was significantly more proximal in the straight group than in the bowing group (P<0.001). The NSA was not significantly different between the groups. Of note, in the bowing group, the average ratio of the distance between the estimated apex and fracture site to the entire femur length was 4.3%±3.3%. Radiological characteristics, including the estimated apex height data in the bowing group, are presented in Table 2.
3. Factors affecting the fracture height of AFFs
Multivariable linear regression analysis of the total cohort showed that the presence of anterolateral bowing was the most important factor associated with the fracture height (β=0.542; 95% confidence interval [CI], 0.311–0.772; P<0.001). Height was also associated with the fracture height in total cohort (β=−0.149; 95% CI, −0.277~−0.020; P=0.023). In the straight group, the lateral bowing angle was associated with the fracture height (β=0.271; 95% CI, 0.008-0.528; P=0.042). In the bowing group, the estimated apex height was the only factor associated with the fracture height (β=0.654; 95% CI, 0.415–0.892; P<0.001).
DISCUSSION
Our results show important findings regarding the fracture height of AFFs: (1) in the total cohort, the presence of anterolateral bowing itself was most important factor associated with the fracture height; (2) in the bowed femur, the estimated apex height was the only decisive factor associated with fracture height; and (3) the degree of the lateral bowing angle was not significantly associated with fracture height in the total cohort and the bowing group, but it was significant in the straight group. These findings are helpful in understanding the role of anterolateral bowing as the femoral geometry in the development of AFFs and early identification of the location of suspicious AFF. A second AFF task force report from the ASBMR also stated that lower limb geometry could be considered as a potential contributor and that more work is needed in this area.[22]
Currently, AFF is often classified into 2 groups: subtrochanteric and diaphyseal fractures. This dichotomous classification is useful for deciding treatment options and comparing their outcomes, but it is inappropriate for predicting the location of the prefracture lesions. Thus, the current study used a different approach in order to elucidate the correct localization of the early AFFs. We focused on the mechanical causes of the fracture (straight or bowed femur) rather than on the fracture results (subtrochanteric and diaphyseal fractures). Additionally, we confirmed that the 2 groups in the present study had their own characteristics and different distribution patterns of AFFs, based solely on the presence of anterolateral bowing.
Until now, several studies have attempted to identify the effect of anterolateral bowing on the location of AFFs. Both Chen et al.[20] and Soh et al.[21] reported that the degree of lateral bowing angle is associated with the location of AFFs and that more distal AFFs occurred with a larger degree of lateral bowing angle. These previous results are inconsistent with ours, as previous studies had small, heterogeneous cohorts (regardless of the presence of anterolateral bowing), and statistical analysis was restricted to univariable analysis. Actually, in the univariable analysis (Pearson's correlation coefficient) of the present study, the lateral bowing angle was correlated with the fracture height in the total cohort. However, in the multivariable linear regression analysis, the lateral bowing angle was no longer significantly associated with the fracture height. Interestingly, in the straight group, the lateral bowing angle was associated with the fracture height. Our study had several strengths compared with previous studies. Our cohort was relatively large, and multivariable analysis was performed to determine the factors associated with the fracture height of AFFs. In addition, we performed subgroup analysis to identify the effect of anterolateral bowing on the fracture height.
From the mechanical perspective, the estimated apex point is usually located at the most lateral part of the femoral shaft where high tensile stress is generated during the gait cycle.[24] Since an AFF is regarded as a type of insufficiency fracture, we speculate that the microcrack begins at the point where the stress concentrates on the apex of the curve from daily stress. In the straight group, 64% of AFFs occurred in the subtrochanteric area where the highest tensile stress is generated during gait in normal limb alignment.[11] However, remaining 36% of AFFs in straight group occurred in diaphysis. Although the lateral bowing angle in the straight group was minimal, ranging from −3.2° to 7.5°, it was significantly associated with increases in fracture height. This might serve as a clue to precisely predict the fracture height in the straight femur. The other factors, such as biologic factors, should be considered and further studies on this topic are necessary.
Although there are several methods of evaluating femoral bowing, the bowing angle assessment is subject to large margins of error.[142021] Most of the available simple methods measure the angle between 2 bisecting lines of the proximal and distal shaft, respectively. However, there is a possibility of underestimation or overestimation, because the shape of bowing and the length of the femur within each AFF are different. In addition, the bowing of the femur is not simply an angular deformity at one point. Therefore, we previously developed a simple grading system for evaluating anterolateral bowing using a reference line. Although the degree of bowing is roughly evaluated using 3 grades rather than a numerical value, the grading system is still useful because we can analyze both the degree and the shape of bowing simultaneously, with high inter-observer and intra-observer reliability (kappainter=0.893 and kappaintra=0.883, respectively, in our previous study).
We found that the curve apex was close to the fracture site (Fig. 1); thus, we could speculate that the shape of the bowing affects the location of AFFs with anterolateral bowing. The mean distance between the estimated apex and fracture site was only 4.3% (ratio). We illustrated the estimated apex in the lateral cortex by parallel migration of the reference line to the medial cortex, because the curvature of the medial cortex is more acute than that of the lateral cortex. The diameter of the femur widens as it moves from the middle of the diaphysis to either the proximal or distal metaphysis, which makes the apex in the lateral cortex less prominent. Although the anterolaterally bowed femur has no anatomical axis, the reference line is similar to the anatomical axis of the straight femur. Therefore, the reference line seems to properly reflect the alteration of the shape of the bowed femur, because the bowing deformity mainly occurs in the diaphysis rather than in the metaphysis.
The current study had a few limitations. First, this investigation was a retrospective study because of the rare occurrence of AFFs. For example, only 49 (49%) patients (27 in the straight group and 22 in the bowing group) had available preinjured ipsilateral radiographs for the radiographic analysis, and contralateral radiographs were inevitably used under the assumption that both femora were symmetrical. Second, the presence of anterolateral bowing and the estimated apex height using our method could be inaccurate because we estimated them from a 2-dimensional (D) anterior-posterior radiograph, which may not rereflect the true 3D deformity. If the patient had severe anterior bowing but minimal lateral bowing, the patient might be classified into the straight group. However, anterolateral bowing is usually associated with femoral anteversion and is perpendicular to femoral neck anteversion plane.[25] Third, we could not evaluate the effect of lower limb alignment on the location of AFF in current study because only a small number of patients had preinjured standing full-length lower limb radiographs. Lower limb alignment could be influenced on the location of AFFs by change of mechanical stress distribution on the femur.[26]
Early awareness of AFFs is clinically beneficial because the treatments for complete AFFs are challenging.[27] Once AFF is diagnosed in the early phase of incomplete fracture, clinicians and patients can make the effort to prevent the incomplete fracture from progressing into a complete fracture. We demonstrated that the presence of anterolateral femoral bowing itself is important for the fracture height of AFFs. In the straight femur, the incidence was higher in the subtrochanteric area and decreased gradually toward the distal part of the diaphysis. In the bowed femur, all AFFs occurred in the diaphysis, and only the estimated apex height was associated with the fracture height of AFFs. In addition, the estimation of the apex height using a reference line can increase the accuracy of predicting the prefracture lesion in a bowed femur. Recent studies have reported that an extended femur scan via dual energy X-ray absorptiometry may be used as a good screening tool for the early detection of prefracture lesions of AFFs.[28] On the basis of our study, we suggest that an extended femur scan should be performed on the entire femur,[29] including the femoral condyle, to evaluate the presence of anterolateral bowing and estimate the apex of the bowed femur using a reference line.




 XML Download
XML Download