

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Osteoporotic fractures has been recognized as a major public health challenge as a result of the high prevalence and associated morbidity.[12] Substantial evidence also suggests that patients who sustained a single fragility fracture are at a significantly increased risk of having a second fracture in the future.[34] A recent study reported that an osteoporotic fracture represented the most important predictive factor for further osteoporotic fractures, so, every country in the world has been attempting to treat osteoporosis for the prevention of osteoporotic fractures and refractures.[56]
Among the osteoporotic fractures, proximal humeral fractures represent a unique subset; most of these fractures occur in patients older than 65 and are associated with female gender, making them the second most common upper-extremity fractures.[78] Like other osteoporotic fractures, a proximal humerus fracture is also a known risk factor for subsequent osteoporotic fractures.[910] However, these previous studies have limitations such as small sample size and information limited to specific institutions. Although several studies have used nationwide claim or registered database to overcome these limitations, most studies mainly focus on osteoporotic fractures following hip fractures [1112] and little is known regarding proximal humerus fractures. A better understanding of the features of refractures after proximal humerus fracture is needed for the prevention of further osteoporotic fractures.
Thus, the objectives of this study were to investigate the incidence and characteristics of osteoporotic refractures after the proximal humerus fracture in Korea based on an analysis of nationwide data acquried from Korean National Health Insurance (KNHI) service.
METHODS
The study protocol was approved by Institutional Review Board (IRB) of Wonkwang University Sanbon Hospital (IRB No. WMCSB 201706-64). Informed consent was waived by the board.
1. Study design and data collection
This study was a retrospective review of KNHI claims database, which covers 100% of the population: 97% covered by health insurance and 3% by medical aid. All clinics and hospitals submit patient data including procedure and diagnostic codes according to the International Classification of Diseases, 10th revision (ICD-10).[13]
Patients aged 50 years or older with initial proximal humerus fractures reported in 2012 were enrolled and followed up until 2016. An unique personal identifier permitted the tracking of individuals for the occurrence of osteoporotic refractures. Refractures including spine, hip, distal radius, and humerus were identified from the nationwide database provided by the KNHI service between 2012 and 2016. We selected these 4 anatomical sites because they represent the 4 most common locations of fragility fractures in older individuals and are the most strongly associated with increasing age.[3] To identify the first occurrence of a proximal humerus fracture (index fracture) in 2012, patients with a history of fractures, sustained from 2007 to 2011, were excluded from the study. We also excluded the patient who had evidence of multiple fractures within 6 months before and after the index fracture as these fractures were most likely associated with high-energy trauma.[14] The patients were categorized by sex to deterimine any differences in the incidence of osteoporotic refracture. We also analyzed patient data to identify the location of refracture after proximal humerus fracture and presented it over the follow-up period.
2. Definition of osteoporotic fracture and refracture
The KNHI data collected between January 1, 2012 and December 31, 2016 were searched to identify all claims records of outpatient visits or hospital admissions of patients aged 50 years and above. Osteoporosis-related fractures were identified using specific ICD-10 codes and site-specific physician claims for procedures. To avoid the risk of multiple counting, patients with surgically treated osteoporotic fractures were counted first based on ICD-10 and operation codes. Subsequently, patients with conservative procedure code for osteoporitc fracture and those without any of these specific codes were identified to include individuals treated conservatively.[8]
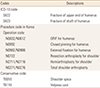
Fractures were identified on the basis of selected ICD-10 codes for humerus (ICD-10 codes S422 [fracture of upper end of humerus], S423 [fractured shaft of humerus]) with ten operative procedures and 2 conservative procedures: open reduction and internal fixation of humerus (N0602 or N0612), closed pinning for humerus (N0992), external fixation (N0982 or N0986), resection arthroplasty (N0722), arthroplasty (N2711, N2716, N0271, N0276) shoulder spica (T6010), and velpeau cast (T6110) (Table 1).[81516]
Other osteoporotic fractures including spine (S22.0 [fracture of the thoracic spine], S22.1 [multiple fractures of the thoracic spine], S32.0 [fracture of the lumbar spine], S32.7 [multiple fracture of the lumbar spine], T080 [fracture of the spine], M48.4 [fatigue fracture of vertebra], M48.5 [collapsed vertebra] and M49.5 [Collapsed vertebra]); hip (S72.0 [fracture of the femur neck] and S72.1 [trochanteric fracture]); and radius (S52.5 [fracture of lower end of radius] and S52.6 [fracture of lower end of both ulnar and radius]) were also detected based on ICD-10 and procedure codes.[1317181920]
Based on the last claim date, the refracture was classified as an osteoporotic fracture including spine, hip, distal radius and humerus 6 months after the index proximal humerus fracture (180 days).[121318] The untreated period was set at 6 months and the new event was regarded as a refracture. If an individual was diagnosed more than once within 6 months for the proximal humerus fracture, it was considered the same event. Furthermore, as described previously, if patients who had other fractures within 6 months after the index proximal humerus fracture were considered as high-energy trauma, they were excluded from the study. In all these scenarios, the refracture was defined as a case based on the same operational definition after a 6-month untreated period.
The cumulative incidence of refracture was calculated using a life table. The cumulative incidence was defined as the probability of occurrence of a particular event,such as refracture. It was calculated by dividing the number of new refractures over a period of time by the number of proximal humerus fractures at the beginning of the study.
RESULTS
The number of proximal humerus fractures in 2012 was 14,308, of whom 11,376 aged 50 years or older were included in the study. For further analysis, 2,082 patients with previous fractures reported between 2007 and 2011, and 3,707 patients with multiple fractures 6 months before and after the index fracture were also excluded. The remaining 5,587 patients (1,563 men and 4,024 women) who were diagnosed with first-time proximal humerus fracture were followed until December 2016 (Fig. 1).
Between 2012 and 2016, a total number of 1,018 osteoporotic refractures occured. The total cumulative incidence of osteoporotic refractures was 4.85% (271/5,587) at 1 year, 9.61% (537/5,587) at 2 years, 14.21% (794/5,587) at 3 years, and 18.22% (1,018/5,587) at 4 years. The total cumulative incidence in women was higher than in men during the follow-up period (Fig. 2A). The cumulative incidence of second proximal humerus fractures was 0.47% (26/5,587) at 1 year, 0.93% (52/5,587) at 2 years, 1.11% (62/5,587) at 3 years, and 1.27% (71/5,587) at 4 years. By contrast, the cumulative incidence of second proximal humerus fracture in men was higher than in women during the follow-up period (Fig. 2B).
In terms of the site of refracture by year, the proportion of refractures associated with spine was the highest, followed by hip, wrist, and humerus during all the follow-up periods. A total number of 1,018 refractures occured in spine 495 (48.62%), hip 263 (25.83%), wrist 189 (18.57%), and humerus 71 (6.97%) (Fig. 3).
DISCUSSION
To our knowledge, this is the first study reporting the incidence and the location of osteoporotic refractures after the proximal humerus fracture in Korean adults based on an analysis of nationwide data acquired from the KNHI service. In this study, the cumulative incidence of osteoporotic refractures after the proximal humerus fractures was 18.22% for 4 years, and was higher in women than in men during the follow-up period. Although no long-term follow-up study was conducted, the cumulative incidence of osteoporotic refracture showed ever-increasing pattern.
Several previous studies reported osteoporotic refractures after proximal humerus fractures, but most of them focused on subsequent hip fractures. Lauritzen et al.[10] reported that women aged between 60 and 69 years, who had previously sustained a proximal humerus fracture had a relative risk of 2.5 for subsequent hip fracture. Johnell et al.[21] found an increased risk of hip fractures after a humeral fracture, with the increased risk persisting for up to 5 years after the index fracture. Clinton et al.[9] also reported that a proximal humeral fracture independently increased the risk of a subsequent hip fracture more than 5-fold in the first year after the humeral fracture. They reported that among patients diagnosed with proximal humerus fractures, immobilization after the typical osteoporotic fractures weakened the quality of bone and muscle, which further affected the patient's ability to walk and perform activities of daily living safely, and increased the possibility of various refractures. Therefore, limiting the immobilization period and promoting a rapid return to pre-fracture physical performance and functional status must be the goal of rehabilitation to prevent refracture.[2223]
Although the mortality associated with osteoporotic refractures was not investigated in the study, it has been well estabilished in many studies that osteoporotic refractures were related to increased risk of mortality. Bliuc et al.[24] reported that refracture was associated with an increased mortality hazard ratio of 1.91 in women and 2.99 in men. The mortality risk following a refracture declined eventually but beyond 5 years still remained higher than in the general population. Another study also found that mortality following refracture occured predominantly in the first 5 years after the initial fracture and the total mortality was increased for 10 years.[1] In addition, Park et al.[15] reported that the 1-year mortality rate after proximal humerus fracture was also substantially higher than in the general population. Proximal humerus fractures are associated with several factors indicating poor health and high mortality.[9] In fact, any osteoporotic fractures, including proximal humerus fractures that occur in frail individuals are sentinel events that contribute to increased risk of morbidity and mortality.[25] As such, patients sustaining refractures after the proximal humerus fracture might be in a poor general condition and associated with a significantly high mortality rate.
As refractures after the proximal humerus fracture were also associated with the incidence of osteoporotic fractures, refractures after a proximal humerus fracture most commonly involved the spine and total cumulative incidence in women was higher than in men in the study. Several previous studies showed that the incidence of osteoporitc fractures was higher in women than in men [14] and vertebral fractures are the most common single osteoporotic fractures worldwide, constituting an integral component of the osteoporotic syndrome in 30% to 50% of adults over the age of 50.[26] However, the cumulative incidence of second proximal humerus fracture in men was higher than in women in the study; this atypical finding might be related to uneven gender ratio of intial osteroportic humers fractures. The female to male ratio of initial osteoporotic fractures was 2.6; this female dominance was less prominent in second humerus fractures, which might have resulted in higher cumulatative incidence of second proximal humerus fractures in men.
This study has a number of limitations. First, the exclusion of patients with multiple fractures and a history of fractures may skew the overall results, leading to a possible underestimation of the refracture rates and volumes. Second, we did not investigate the type of treatment for a proximal humerus fracture, which affected the refracture incidence. Surgical interventions for the management of proximal humerus fracture have increased recently, and included procedures such as plate fixation, intramedullary nails, and arthroplasty. The incidence of refracture may be affected by operative and non-operative treatments, and the extent of rehabilitation was determined by the type of operationcause. Third, pathologic fractures due to tumors were not excluded. Therefore, fracture incidence may have been overestimated. Fourth, data related to bone mineral density, lifestyle, comorbidity, and treatments, including vitamin D and anti-osteoporotic drugs were not available because this study was based on the National Claims Registry. Finally, the follow-up period was relatively short compared to the previous stuidies. However Bliuc et al.[1] reported that the majority of refractures occured in the first 5 years following the inital fracture. Although the overall incidence of secondary fractures depended on the follow-up period, 50% of all the cases occurred within 3 years after the primary event.[2728]
In conclusion, our study based on the National Claims Registry showed that the cumulative incidence of osteoporotic refractures following proximal humerus fracture in elderly has been increasing over the years. Considering that osteoporotic refractures are associated with an increased mortality risk, a strong public health strategy to prevent refractures following proximal humerus fractures in the elderly population is imperative.



 XML Download
XML Download