

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Anaphylaxis is a severe and life-threatening allergic reaction that affects 0.05% to 0.2% of the population worldwide.1 In the last 2 decades, there has been a significant increase in anaphylaxis worldwide, from 2- to 6-fold, especially among children and adolescents.234 In the United Kingdom, European Union and the United States, severe anaphylaxis was rare and the prevalence of the cases were only less than 0.09%.5678910 However, several studies reported that severe cases showed poor outcomes, including poor status of asthma, hypoxic-ischemic brain injury and deaths.11121314
Current treatment guidelines for anaphylaxis suggest administration of antihistamine and steroid and, the most significant method, prompt epinephrine injection.151617 Epinephrine is a powerful adrenergic agent with well-known alpha and beta agonist effects. According to guidelines, intramuscular injection of epinephrine is recommended in proper dose of 0.01 mg/kg, to a maximum of 0.3 mg in children and 0.5 mg in adolescents, during an anaphylaxis event.
It is known to have pharmacologic side effects, including hypertension, pallor, tremor, vasospasm-induced myocardial injury and ventricular dysrhythmias.118 These possible risks for adverse effects cannot exceed the beneficial effects of epinephrine administration in anaphylaxis and there are no absolute contraindications for its use. However, physicians might hesitated to prescribe epinephrine because of its side effects, possible dosing errors, and needle phobia of the patient or caregiver.192021 This inappropriate underuse of epinephrine can be a significant issue because it is the sole effective treatment option that can prevent fatal complications of anaphylaxis.
There were few studies based on Korean national cohort to find the epidemiologic characteristics of anaphylaxis. One study by Cho and Kwon22 showed increasing prevalence of anaphylaxis over the period of 2010–2014. Jeong et al.23 found that the trend of prevalence of anaphylaxis was increasing annually in all age group in 2010–2014; during the same period, almost 88.4% of anaphylactic patients visited emergency department (ED). Our study object is to find if these increasing cases of anaphylaxis were managed properly, especially with epinephrine, in pediatric patients compared to adult patients in ED.2223
MATERIALS AND METHODS
Data source
The data source was the National Health Insurance Service (NHIS)-National Sample Cohort, a population-based cohort established by the Korean NHIS. It contains claim information of 1 million individuals who were randomly sampled after stratification from the entire Korean population. It provides diagnostic codes based on the International Classification of Diseases (ICD)-10 coding system, prescription and procedure codes and related costs, as well as demographic information, such as age, sex and socioeconomic status. It also has information about disability and deaths based on national disability registration data and death certificates, respectively. We used its most recent release, which contains claim data from 2002 to 2013. Detailed descriptions of the cohort data can be found in a previous paper.24 This study was reviewed and approved by the Institutional Review Board (IRB) of Seoul National University Bundang Hospital and the requirement for written informed consent was waived (IRB No. X-1808-489-902).
Case selection and covariates
We considered that most of the epinephrine injections in anaphylaxis victims were conducted in the ED because prehospital administration of epinephrine by emergency medical technicians in the ambulance was, by law, not permitted in Korea during the study period. For the epinephrine autoinjector, it was first introduced in Korea since 2007 and was purchasable only at the Korea Orphan and Essential Drug Center with a doctor's prescription.
We included pediatric (≤ 18 years old) and adult (> 18 years old) patients in the ED with a discharge diagnosis of anaphylaxis (ICD-10 codes: T78.0x, T78.2x, T80.5x and T88.6x) from 2004 to 2013. We assessed prescription information, including epinephrine (anatomical therapeutic chemical [ATC] code: C01CA24), antihistamine (ATC code: R06) and systemic steroid (ATC code: H02), for each visit and information about disposition, including admission to ward and admission to intensive care unit (ICU), at the index visit. We also assessed the following information as covariates: previous history of anaphylaxis, any history of cardiovascular disease (ICD 10 codes: Ix), household income level, hospital size and hospital setting, which was an urban (or suburban) or a rural setting. The covariate status for previous anaphylaxis and cardiovascular disease were determined based on the claim information within 2 years prior to the index visit. Patient age was categorized into < 7 (young children), 7–12 (school age children), 13–18 (adolescents), 19–65 (adults) and > 65 (old age) intervals. Household income level was categorized into quintiles and the patients receiving medical aid from the national government were included in the first quintile. Hospital size was determined based on the number of beds and was categorized into < 100, 100–299, 300–599, 600–899 and ≥ 900 beds.
Statistical analysis
Categorical variables were reported as the frequency and proportion, while continuous variables were reported as the median and interquartile ranges. Wilcoxon's rank-sum test, the χ2 test, and Fisher's exact test were performed, as appropriate, for comparisons between groups.
We first compared the overall chance of using epinephrine between the pediatric and adult populations and assessed the association between age groups and the use of epinephrine using the χ2 test for trends. We constructed a multivariable logistic regression model to adjust for possible confounding effects of covariates. Finally, because it was impossible to know the availability of epinephrine autoinjectors for each patient, we performed sensitivity analysis excluding the patients with a previous history of anaphylaxis.
The goodness-of-fit of the logistic regression models was assessed using the Hosmer-Lemeshow goodness-of-fit test. The results of the multivariable analyses are presented as the odds ratio (OR) and 95% confidence interval (CI). The P values < 0.05 were considered significant. All data handling and statistical analyses were performed using R package version 3.3.2 (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
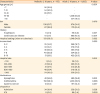
From 2004 to 2013, a total of 175 and 1,605 ED visits with a discharge diagnosis of anaphylaxis were identified from the pediatric and adult populations, respectively (Table 1). A total of 42 (24%) of pediatric patients were treated with epinephrine, while 592 (36.9%) of the adult patients were treated with epinephrine, and this difference was statistically significant (P = 0.001). For the other covariates, the pediatric patients had lower chance of having a previous history of any cardiovascular diseases (5.7% vs. 42.5%, P < 0.001), were more likely to be treated in a larger hospital (number of beds ≥ 300; 76.0% vs. 66.9%; P < 0.018) located in cities (90.9% vs. 84.0%, P = 0.002) and were less likely to be treated with systemic steroid (6.9% vs. 12.3%, P = 0.047). For the disposition, there was no significant difference in admission to the general ward (19.4% vs. 21.8%, P = 0.529); however, admission to the ICU was significantly lower in the pediatric population (0% vs. 5.4%, P = 0.003).
Table 1
Patient characteristics
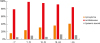
The study population was categorized based on age at index visit (< 7, 7–12, 13–18, 19–65 and > 65), and the associations between age group and medication use as well as between patient disposition are assessed in Table 2. The chance of using epinephrine or antihistamine as well as admission to the general ward or ICU was significantly different according to age groups (P = 0.003, P < 0.001, P < 0.001 and P < 0.001, respectively). Additional trend analysis showed a significantly lower chance of using epinephrine in the younger age group with P trend value of <0.001 (Figure).
Table 2
Medication use and patient disposition by age group

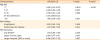
We constructed a multivariable logistic regression model to assess the association between age and chance of using epinephrine (Table 3). The ORs for administration of epinephrine in the pediatric population relative to baseline (age group: 19–65) were 0.34 (95% CI, 0.15–0.67), 0.56 (95% CI, 0.28–1.03) and 0.79 (95% CI, 0.45–1.33) in the < 7, 7–12 and 13–18 age groups, respectively, with a decreasing trend of epinephrine with decreasing age (P trend < 0.001).
Table 3
Logistic regression model for the use of epinephrine for anaphylaxis
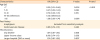
We conducted a sensitivity analysis excluding patients with a previous history of anaphylaxis. The chance of using epinephrine was still low in the pediatric population (23.7% vs. 37.2%, P = 0.001). Logistic regression model using the same covariate set, except inclusion of history of anaphylaxis, showed similar association between age group and epinephrine use, with ORs relative to baseline (age group: 19–65) of 0.33 (95% CI, 0.15–0.66), 0.57 (95% CI, 0.29–1.05) and 0.70 (95% CI, 0.39–1.21) in the < 7, 7–12 and 13–18 age groups, respectively (Table 4), with a decreasing trend of epinephrine use with decreasing age (P trend < 0.001).
Table 4
Sensitivity analysis (excluding patients with a previous history of anaphylaxis)
DISCUSSION
In this population-based study, we assessed whether there was decreased epinephrine use in the pediatric population. The use of epinephrine was lower in the pediatric population, especially in those younger than 7 years. This finding was still observed in the sensitivity analysis, in which patients with possible use of prehospital epinephrine autoinjector use were excluded. We think this finding suggests that physicians working in the ED are reluctant to use epinephrine for treating pediatric patients with anaphylaxis, especially when the victims are very young.
Several studies have reported low rates of epinephrine injection for patients with anaphylaxis. Ninchoji et al.25 retrospectively reviewed medical records for anaphylaxis at 1 children's primary medical center in Japan, and they found that only 8% of the victims were treated with epinephrine. Another study Sidhu et al.26 reported that 47% of the pediatric patients (<18 years old) with anaphylaxis received epinephrine in the ED, while our study showed that 24% of the same age group received the treatment. The reason why there is a marked decrease in the use of epinephrine in the pediatric population is not clear. It is possible that a new allergen exposure, such as food, was the major cause of pediatric anaphylaxis so that it is difficult to be suspected from previous allergic history. This could have influenced the lack of confidence of physicians in making a diagnosis of anaphylaxis, especially when patients are young. Samady et al.27 reported that infants experience new foods as frequently as every week and that their food-induced allergies are initially misdiagnosed as respiratory infections. Additionally, physicians need to have high suspicion when diagnosing anaphylaxis in infants because it is hard to recognize due to its signs such as regurgitation after feeding or crying, which commonly occur in the healthy population.28 If physicians are not confident with their diagnosis, they could be more reluctant to use epinephrine, which is well known for both its powerful adrenergic effect and its potential side effects.
However, it is also possible that the symptoms or physical findings of children are different from those of adults, leading healthcare providers to make a misdiagnosis. Thomson et al.29 reported that most of the children who did not receive epinephrine showed improvement of symptoms when they arrived at the ED. Braganza et al.30 found that children with anaphylaxis predominantly have respiratory symptoms and that the prevalence of asthma in this population is significantly higher than that of adults, while the latter population has more common cardiovascular instability during anaphylactic reaction. They also reported that the cutaneous features of anaphylaxis are not identified in up to 20% of patients or that they are masked by antihistamines. These findings could also affect the uncertainty of a diagnostic decision.
However, there are some studies that improve anaphylaxis diagnosis and treatment by protocol-based management. One pediatric emergency unit in a Spanish tertiary hospital initiated a protocol for the management of anaphylaxis in 2008, and they found a significant improvement in epinephrine administration, from 27% to 57.6%, in the pre- and post-groups after 2 years.31 Rueter et al.32 compared the management of anaphylaxis in children before and after the introduction of allergy training programs for physicians at a tertiary hospital of Australia, and they concluded that adrenaline mismanagement decreased by approximately 88% after 10 years. However, only 28.3% of the victims received proper epinephrine during the after-study period.32 Because it is rare to introduce these effective educational programs and treatment protocols in EDs in South Korea, we need further studies to develop a Korean protocol that can be adopted to provide proper treatment of anaphylaxis.
This study has several limitations. First, misclassification is a potential cause of bias in a population-based study using claims records. Secondly, we could not adjust for the severity of anaphylaxis, which will influence the decision for epinephrine use in the ER. Thirdly, we could not adjust for the prehospital use of epinephrine. However, it is almost certain that prehospital use of epinephrine by EMTs would be almost nonexistent because it was not allowed during the study period, but, personal use of epinephrine autoinjectors was available to some patients with a previous history of anaphylaxis. These patients could have used these injectors if they were previously prescribed them. However, our sensitivity analysis showed a similar association regardless of the inclusion of patients with a previous diagnosis of anaphylaxis.
In conclusion, almost more than 70% of the pediatric victims of anaphylaxis experience improper treatment including the underuse of epinephrine injection in Korea. We suggest that a nationwide anaphylaxis campaign or a certain protocol-based treatment approach is needed to reduce a knowledge-to-action gap of health care professionals in giving the correct treatment of anaphylaxis in children.
 XML Download
XML Download