

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The global prevalence of clinical asthma is 4.5%, translating to 315 million individuals affected with asthma.1 In China, the clinical asthma prevalence from 2010 to 2011 was 1.24%,2 which equalled to approximately 30 million patients. Among these, only 40.5% were assessed by clinicians to have their clinical symptoms adequately controlled.2
Based on the recommendations in the Global Initiative for Asthma (GINA),3 for patients with moderate asthma who are symptomatic despite the use of inhaled corticosteroids (ICS), the preferred stepwise options are to increase the dose of corticosteroids or add a long-acting bronchodilator (presently a long-acting β2 agonist [LABA]) to the maintenance treatment regimen, or both. If patients still remain symptomatic, then the dose of ICS should be increased or anti-immunoglobulin E (IgE) and anti-interleukin (IL)-5 should be added. However, these options may not be beneficial to all patients and can increase the occurrence of side effects, especially with the long-term use of ICS.4
Under such circumstances, it is of great interest to explore other options for patients such as an add-on therapy with another long-acting bronchodilator tiotropium. In one of the earlier studies on patients with poorly controlled asthma, Peters et al.5 found that tiotropium, when added on to inhaled glucocorticoid, showed superior clinical efficacy in lung function compared with just doubling of the dose of the inhaled glucocorticoid. Until now, tiotropium, as a treatment option for asthma, has been investigated in systematic clinical trials by Bateman et al.,6 Kerstjens et al.,78 and Paggiaro et al.9 on symptomatic patients with asthma of varying severity under various doses of ICS with or without LABA. The results of these studies have influenced guidelines such as GINA to include tiotropium in the stepwise approach for treating severe asthma. Tiotropium is recommended by GINA as add-on therapy for patients with a history of exacerbations based on a systematic meta-analysis review of tiotropium in asthma.10
Previous studies indicated that tiotropium, as add-on therapy, might benefit patients with moderate symptomatic asthma and appeared comparable with add-on LABA.56 These studies had a short trial duration due to the absence of an active LABA treatment arm or inadequate power. Kerstjens and colleagues11 addressed these limitations, and assessed the efficacy and safety of tiotropium with salmeterol as an active comparator as add-on to medium-dose ICS in patients with moderate asthma in a twin study with a 24-week duration. These results have previously been published and reported comparability between tiotropium and salmeterol.11 This pooled analysis reported the efficacy and safety of tiotropium in Chinese patients with moderate persistent asthma on top of ICS and made comparisons with the results of the overall study population.
MATERIALS AND METHODS
Study design
This was a Chinese subgroup analysis of two 24-week, multicenter, replicate, randomized, double-blind, double-dummy, active and placebo-controlled, parallel-group phase 3 studies (Clinicaltrials.gov: NCT01172808 and NCT01172821) including Chinese patients at 32 sites in China (15 sites for MezzoTinA-asthma 1 [trial 1] and 17 sites for MezzoTinA-asthma 2 [trial 2]). The aim of the study was to evaluate the efficacy and safety of 2 doses of tiotropium (2.5 and 5 µg; Tio R2.5 and Tio R5, respectively) compared with placebo and LABA (salmeterol) on top of medium-dose ICS maintenance therapy in adult patients with not fully controlled, moderate, persistent asthma.
After a 28-day screening period, eligible patients randomized to the treatment period received either Tio R5 or Tio R2.5 solution for inhalation via the Respimat inhaler, 50 µg salmeterol (Sal 50) via the metered-dose inhaler (MDI), or placebo (tiotropium matching placebo administered via the Respimat inhaler and salmeterol matching placebo administered via the MDI). The patients had to inhale 2 puffs from the MDI (salmeterol or placebo) every morning and every evening and 2 puffs from the Respimat inhaler (tiotropium or placebo) every evening. The trial medication was given on top of medium-dose ICS maintenance therapy in patients who were not optimally controlled with their current asthma medication. Usual maintenance therapy included medium-dose ICS, alone or in a fixed combination with a LABA or a short-acting β2 adrenergic agonist (SABA). The patients on combination therapy were to be switched to the inhaled steroid mono-product without changing the steroid dose at least 24 hours prior to screening. Salbutamol (also known as albuterol), a SABA, was provided as rescue medication for use as necessary throughout the trials. After the 24-week treatment period, the patients were followed up for 21 days (Fig. 1). The study was conducted in accordance with the Declaration of Helsinki and the International Conference on Harmonisation Harmonised Tripartite Guideline for Good Clinical Practice. Prior to the start of the study, the trial protocols, patient information sheet, and written informed consent were reviewed and approved by the independent ethics committees and/or Institutional Review Boards and competent authority, according to the national and international regulations. Independent ethics committees of the China-Japan Friendship Hospital (approval No.: 2011-18) and Ruijin Hospital (approval No.: 2011-26-3) granted ethics approvals.

Patients
The main inclusion criteria were male or female patients aged between 18 and 75 years diagnosed with asthma before the age of 40 years and at least with a 3-month asthma history prior to enrolment. The diagnosis of asthma needed to be confirmed at screening, and a forced expiratory volume in 1 second (FEV1) increase of ≥ 12% and ≥ 200 mL on the basis of bronchodilator reversibility was required. The inclusion criteria were as follows:
1) patients on maintenance treatment with stable medium-dose ICS (400–800 µg budesonide or equivalent) (alone or in a fixed combination with a LABA or SABA) for at least 4 weeks prior to screening; 2) patients symptomatic at screening with a mean Asthma Control Questionnaire (ACQ) score of ≥1.5; 3) patients with a pre-bronchodilator FEV1 ≥ 60% and ≤ 90% of predicted; 4) absolute FEV1 variation at randomization within ± 30% of the screening value; 5) nonsmokers or ex-smokers with less than 10 pack-years for at least 1 year prior to enrolment; and 6) no asthma exacerbation or acute respiratory tract infection in the 4 weeks prior to screening.
The main exclusion criteria were chronic obstructive pulmonary disease and other significant concomitant diseases, concurrent use of β-blockers or long-acting anticholinergic bronchodilators or β2-adrenergics within 4 weeks prior to and/or during the screening, or anti-IgE antibodies within 6 months prior to and/or during the screening.
Randomization and blinding
After final assessment of all inclusion and exclusion criteria, eligible patients were randomly assigned in a 1:1:1:1 ratio to receive once-daily Tio R2.5 or Tio R5 inhaled solution, twice-daily salmeterol 50 µg HFA-MDI, or placebo. Boehringer Ingelheim Pharma GmbH & Co KG (Biberach an der Riss, Germany) generated the randomization list using a validated system involving a pseudorandom number generator with a supplied seed number to ensure reproducible and unpredictable treatment allocation. A block size of 4 was used to ensure a balanced allocation of patients. Tiotropium, salmeterol, and placebo were administered in a double-blind, double-dummy manner. Neither patients nor investigators were aware of the identity of their treatment.
Outcomes and assessments
The 2 co-primary endpoints for lung function were peak FEV1 defined as the highest FEV1 within 3 hours after dosing and trough FEV1 defined as FEV1 measured within 10 minutes before administering randomized treatment. Peak and trough FEV1 responses were both defined as the change from baseline and determined at the end of the 24-week treatment period. The third co-primary endpoint was the responder assessed by the ACQ at the end of the 24-week treatment period, using combined data from both trials. A responder was defined as a patient who had an improvement of at least 0.5 (minimum clinically important difference) for the ACQ score.
Secondary endpoints included peak (within 3 hours after dosing) and trough forced vital capacity (FVC) and mean weekly pre-dose morning and evening peak expiratory flow (PEF) (home assessed by patients in the last week of the 24-week treatment period). The PEF AM/PM response was defined as the change from the baseline (measured during the last week before randomization). The secondary endpoints on combined data from 2 trials included Asthma Quality of Life Questionnaire score response, time to the first severe asthma exacerbation, time to the first asthma exacerbation, and the ACQ value at each visit, all during the 24-week treatment period.
For the Chinese subpopulations, the following efficacy variables were analyzed using combined data from both trials: FEV1 peak0–3h, trough FEV1, FVC peak0–3h, trough FVC, trough PEF, and ACQ responder rates.
Spirometry measurements were in accordance with the ATS/ERS criteria. Pulmonary function tests (PFTs) were performed at approximately the same time between 18:00 and 20:00. PFTs were conducted 10 minutes before and for up to 3 hours (after 30 minutes, 1 hour, 2 hours, and 3 hours) following the inhalation of trial medication. Trial medication started with the administration of ICS followed immediately by the investigational drug. The highest FEV1 and FVC from 3 acceptable manoeuvres were recorded.
PFT home assessments (PEF and FEV1) were performed with AM3 (eResearch Technology, Hoechberg, Germany) at approximately the same time of the day, 6:00-8:00 for morning measurements and 18:00-0:00 for evening measurements, both prior to administering trial medication. The highest PEF and FEV1 out of 3 acceptable blows were used for evaluation. Patients' self-administered ACQ 1-6 questions prior to PFT, and the clinic staff completed question 7 after PFT.
Safety variables analyzed in the Chinese subpopulation were adverse events (AEs), which were recorded in the electronic case report forms. Safety data analyzed for the Chinese subpopulation were pooled ones from both trials to provide robust AE frequencies and to draw concrete safety conclusions.
Statistical analysis
For the overall study population, the 2 co-primary endpoints FEV1 peak0–3h response and trough FEV1 response were analyzed using a restricted maximum likelihood-based mixed-effects model with repeated measures (MMRM). The ACQ responses were provided as odds ratios for the probability of response. Comparisons of salmeterol versus placebo and tiotropium versus salmeterol were included as exploratory analyses. Details of the endpoint analyses have been previously described.11 The subgroup analyses of Chinese patients were based on the pooled data.
The full analysis set (FAS) was used for the co-primary and secondary efficacy evaluations. The treated set was used for all safety evaluations.
The overall sample size was originally calculated to detect statistical significance on efficacy for the individual main studies.11 The statistical analyses presented for this subgroup were therefore descriptive in nature and not for inferential purposes, although including at least 100 Chinese patients per treatment group was pre-planned in the pooled trials, translating to approximately 50 per treatment group in each study.
RESULTS
Patient characteristics
A total of 820 Chinese patients were enrolled and 432 were randomized. Two Chinese patients randomized to Tio R5 were not treated. Furthermore, 430 patients were treated, and 413 (96%) of them completed the study (Fig. 2). The percentages of prematurely discontinued patients were low across treatment groups. No patient prematurely discontinued the treatment due to noncompliance with the protocol. Demographics and baseline characteristics were similar among the 4 treatment groups (Table 1).

Table 1
Baseline characteristics
FEV1 peak0–3h and trough FEV1
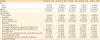
The first co-primary endpoint FEV1 peak0–3h response at 24 weeks significantly improved in the Tio R2.5 and Tio R5 treatment groups compared with the placebo group. The adjusted mean treatment difference versus placebo for the Tio R2.5, Tio R5, and salmeterol groups was 0.249 L, 0.234 L, and 0.284 L, respectively (all P < 0.0001) (Table 2).
Table 2
Adjusted mean (SE) FEV1 peak0–3 h response and trough FEV1 response at 24 weeks for pooled trials MezzoTinA-asthma 1 and -2: Chinese patients (FAS, MMRM)

SE, standard error; FEV1, forced expiratory volume in 1 second; FAS, full analysis set; MMRM, mixed-effects model with repeated measures; CI, confidence interval; FVC, forced vital capacity; Tio R2.5, tiotropium 2.5 μg once-daily; Tio R5, tiotropium 5 μg once-daily; Sal 50, salmeterol 50 μg twice-daily.
*Adjusted for trial treatment, center, visit, baseline, visit-by-treatment, and baseline-by-visit (center was replaced with a trial for the combined model). The patient was considered random, and a spatial power covariance structure was used. †Change from trial baseline; ‡Number of patients with measurements in week 24.
The second co-primary endpoint trough FEV1 responses at 24 weeks also significantly improved in the Tio R2.5 and Tio R5 treatment groups compared with the placebo group. The adjusted mean treatment difference versus placebo for the Tio R2.5, Tio R5, and salmeterol groups was 0.172 L, 0.180 L, and 0.164 L, respectively (all P ≤ 0.001) (Table 2).
ACQ responder analysis
The ACQ responder rate for placebo, Tio R2.5 and Tio R5, and salmeterol at 24 weeks was 58.7%, 62.3%, 59.3%, and 69.1%, respectively. The odds of a patient being an ACQ responder after 24 weeks increased by 1.16-fold (P = 0.6937) and 1.03-fold (P = 1.0000) with tiotropium 2.5 µg and 5 µg, respectively, compared with placebo (Table 3).
Table 3
ACQ responder rate in week 24 for pooled trials MezzoTinA-asthma 1 and asthma 2: Chinese patients (FAS, fisher's exact test)

ACQ, Asthma Control Questionnaire; FAS, full analysis set; Tio R2.5, tiotropium 2.5μg once-daily; Tio R5, tiotropium 5μg once-daily; Sal 50, salmeterol 50μg twice-daily; CI, confidence interval.
*Responder: an improvement in the ACQ total score (i.e., a decrease in the score) from trial baseline of ≥ 0.5; †calculated as a minimum (2*1-sided P value; 1.0) using the 1-sided P value for the superiority of tiotropium.
FVC (peak and trough)
Both doses of tiotropium treatment groups improved the FVC peak0–3h response and the trough FVC response after 24 weeks of treatment. For the FVC peak0–3h response, the adjusted treatment difference versus placebo for the Tio R2.5, Tio R5, and salmeterol groups was 0.126 L (P = 0.0041), 0.094 L (P = 0.0312), and 0.158 L (P = 0.0003), respectively. For the trough FVC response, the adjusted treatment difference versus placebo was 0.097 L (P = 0.0479), 0.082 L (P = 0.0919), and 0.145 L (P = 0.0029), respectively.
Trough PEF
In week 24, the adjusted mean trough PEF response significantly increased in both tiotropium treatment groups. Compared with placebo, the adjusted mean treatment difference was 34.668 L/min (P < 0.0001) for Tio R2.5, 34.278 L/min (P < 0.0001) for Tio R5, and 24.405 L/min (P = 0.0006) for salmeterol.
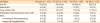
Safety
The overall safety profile was comparable across the treatment groups (Table 4), although patients reported AEs being slightly lower in the active treatment groups. Drug-related AEs were reported for a similar percentage in the 4 groups. Most AEs were of mild to moderate intensity. All serious AEs required hospitalization, and only 1 patient in Tio R5 group had immediately life-threatening serious AEs due to chemical poisoning. No patient died during the treatment period. Thirst was reported in 15 patients: 3 receiving placebo, 2 receiving Tio R2.5, 6 receiving Tio R5, and 4 receiving salmeterol. Cardiac disorders were reported in less than 2% of patients with no difference between the groups. In general, both doses of tiotropium were well tolerated in Chinese patients, with similar safety profile to placebo.
Table 4
Adverse events
DISCUSSION
This is the first trial to demonstrate that once-daily tiotropium (Tio R2.5 and Tio R5) add-on to medium-dose ICS was an efficacious treatment option and had a safety profile comparable to placebo for Chinese patients with moderate symptomatic asthma. Based on the analysis of FEV1, FVC, PEF, and ACQ variables for Chinese patients, the efficacy results on the lung function and asthma control were generally consistent with those from the MezzoTinA-asthma study population.11
In terms of peak and trough FVC and trough PEF observed in this Chinese population, both doses of tiotropium and salmeterol displayed statistically significant increases compared with placebo, except Tio R5 for trough FVC. Although the study was not designed to compare between 2 active comparators, the results for tiotropium displayed general numerical comparability with salmeterol in this subgroup. Overall, the findings in terms of lung function improvement in the Chinese patients were similar to those in the overall study population.
ACQ responder rates in this Chinese asthma patient subpopulation with both doses of tiotropium and salmeterol were not statistically different from that of placebo although a significant improvement in FEV1 was demonstrated; the differences in the overall study population were statistically significant.11 The reliability of ACQ in predicting lung function has been debated due to its nature as a patient self-reported questionnaire, where the constructs are indirectly measured and the methods for gathering information may be vulnerable to memory bias.12 For this study, the lack of differences could possibly be due to the small patient size and the known placebo effects in assessing improvement in asthma control.13
The safety profile of tiotropium for asthma in this Chinese subpopulation was, in general, consistent with that observed in the overall study population. Frequencies of drug-related AEs in the Chinese subpopulations were 13.3%, higher than the 6.2% in the overall study population. However, drug-related AEs were low for each of the preferred terms and comparable between treatment and placebo groups. Dry mouth, which is a known systemic anticholinergic effect, was the second most frequent drug-related AE (10 patients) reported in the overall study population, following thirst (15 patients). Thirteen out of the 15 patients who reported thirst were in the Chinese subpopulation, which could be interpreted with a coding/reporting issue for “dry mouth” in these Chinese sites. Hence, the among-population difference was not indicative of any new safety signals.
The GINA guidelines recommend tiotropium as an add-on therapy in steps 4 and 5.3 Subsequent reviews of tiotropium outcome trials demonstrated positive evidence for the benefits of tiotropium use in asthma across adults, children, and patients with heterogeneous asthma (phenotypes and endotypes) profiles.1415 For step 5 treatment, tiotropium has been shown to be beneficial16 and more cost-effective.14 Overall, tiotropium may be a preferred choice considering that the newer biologics therapy, that is, anti-IgE or anti-IL5, are less affordable in China in light of the lower economic status. Considering the potential ethnic and environmental differences between Chinese and other populations, further studies are warranted to investigate the use of tiotropium in Chinese patients with more severe asthma, especially as an add-on choice for patients already treated with ICS + LABA.
This subgroup analysis provided evidence for tiotropium as an effective controller treatment in Chinese patients with moderate asthma not optimally controlled with medium-dose ICS. The findings supported tiotropium as a treatment alternative to salmeterol in patients with moderate asthma.
 XML Download
XML Download