

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Asthma affects approximately 315 million people worldwide, and 5%–10% of them are estimated to have severe or uncontrolled asthma.12 In South Korea, approximately 1.8 million people were diagnosed with asthma in 2014, with a prevalence of 36.3 per 1,000 people.3 Trends in the prevalence of asthma in South Korea are similar to those observed in Western developed countries.3 Current guidelines in South Korea recommend maintenance treatment with medium- to high-dosage inhaled corticosteroids and long-acting β2-agonists (ICS/LABA) for patients with severe asthma to control their symptoms.4 Despite the availability of ICS/LABA therapy, many patients' symptoms remain uncontrolled, resulting in more frequent hospitalizations, increased morbidity, and reduced health-related quality of life.5 Therefore, additional well-tolerated and effective treatment options are needed.
Benralizumab is an interleukin-5 receptor alpha–directed cytolytic monoclonal antibody that has recently been approved for the treatment of severe asthma in the United States, Europe, Japan, and Canada.6789 In the United States, benralizumab is indicated for the add-on maintenance treatment of patients with severe asthma aged 12 years and older, and with an eosinophilic phenotype.6 Benralizumab targets eosinophilic inflammation, which is present in about 50% of patients with asthma and is associated with decreased lung function and increased disease severity, exacerbation frequency, and symptom burden.101112 Benralizumab induces the direct, rapid, and nearly complete depletion of eosinophils via enhanced antibody-dependent cell-mediated cytotoxicity, an apoptotic process of eosinophil elimination involving natural killer cells.1314 In 2 Phase III trials, SIROCCO (NCT01928771) and CALIMA (NCT01914757), benralizumab significantly reduced asthma exacerbations and improved lung function as well as disease control for patients with severe asthma inadequately controlled with high-dosage ICS/LABA and with blood eosinophil counts ≥ 300 cells/µL vs. placebo.1516 For patients with oral corticosteroid (OCS)-dependent asthma, add-on therapy with benralizumab substantially reduced OCS dosages, and many patients receiving benralizumab were able to stop maintenance OCS treatment completely.17
In a Phase IIa dose-ranging trial conducted in South Korea and Japan, benralizumab 2, 20, and 100 mg decreased asthma exacerbation frequency and improved lung function and asthma control for Korean and Japanese patients with severe, uncontrolled eosinophilic asthma.18 The aim of this subgroup analysis was to further characterize the efficacy and safety of benralizumab for Korean patients using data obtained from the SIROCCO Phase III trial.
MATERIALS AND METHODS
Study design and patients
This was an analysis of the subgroup of Korean patients who participated in the SIROCCO trial. Full details of the SIROCCO trial have been published.15 SIROCCO was a randomized, double-blind, parallel-group, placebo-controlled Phase III trial of 1,204 patients enrolled in 17 contries, including South Korea. This study included patients aged 12-75 years with a history of physician-diagnosed asthma that required treatment with medium- to high-dosage ICS/LABA for at least 12 months before enrollment. Eligible patients had 2 or more asthma exacerbations in the 12 months before enrollment that required systemic corticosteroid treatment or a temporary increase in their usual maintenance OCS dosages. Patients also received treatment with high-dosage ICS/LABA (>500 µg/d fluticasone propionate dry powder formulation or equivalent total daily dosage) with or without OCS and additional asthma controllers for ≥3 months before enrollment. The study was conducted in accordance with the Declaration of Helsinki, International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use/Good Clinical Practice guidelines and the ethics committee at each participating site.
The SIROCCO trial consisted of an enrollment visit (week −4), screening phase (weeks −4 to 0), randomization (week 0), treatment period (weeks 0–48), and follow-up visit (week 56). Eligible patients were randomized 1:1:1 to receive benralizumab 30 mg by subcutaneous injection every 4 weeks (Q4W) or Q4W for the first three doses then every 8 weeks thereafter (Q8W; placebo was administered at the interim visits Q4W to maintain blinding) or placebo Q4W for 48 weeks (Fig. 1). Benralizumab and placebo were provided by AstraZeneca (Gaithersburg, MD, USA). Patients in the Q4W arm received their last dose of benralizumab at week 44, and patients in the Q8W arm received their last dose of benralizumab at week 40. Patients continued to receive their background asthma controller medications without dosage modification throughout the trial. Patients with blood eosinophil counts ≥ 300 cells/µL and < 300 cells/µL were recruited in a 2:1 ratio.

Study endpoints
The primary efficacy endpoint was the annual rate of asthma exacerbations vs. placebo. An exacerbation was defined as worsening of asthma that led to: 1) the use of systemic corticosteroids (or a temporary increase in background OCS dosages) for ≥3 days or a single injection of corticosteroids, 2) an emergency department or urgent care visit for <24 hours because of asthma that required use of systemic corticosteroids, or 3) an inpatient hospitalization for ≥24 hours because of asthma. Worsening of asthma was defined as any new or increased asthma signs or symptoms that were concerning to the patient or related to an Asthma Daily Diary alert.
The key multiplicity-protected secondary endpoints in the main trial were prebronchodilator forced expiratory volume in 1 second (FEV1) and total asthma symptom score. The primary and key secondary endpoints included patients with blood eosinophil counts ≥ 300 cells/μL. Spirometry was conducted at the study centers. Patients recorded their asthma symptoms and results of peak expiratory flow measurements (taken using a handheld spirometric device) twice daily in the Asthma Daily Diary using an electronic patient-reported outcomes device. The Asthma Daily Diary was completed by patients in the morning upon waking and in the evening before going to bed. The morning and evening assessments included questions on asthma symptoms, night-time awakenings, and rescue medication use. The total daily asthma symptom score was a composite of the morning and evening responses, scored on a 0 to 6 scale. Greater scores indicated a greater burden of symptoms. The electronic patient-reported outcomes devices were programmed to alert patients and study centers when specific criteria were met for asthma worsening on ≥2 consecutive days/nights, including a decrease in morning peak expiratory flow of ≥30% compared with baseline, a ≥50% increase in rescue medication use or 1 new β2-agonist nebuliser compared with the previous 7 days, nocturnal awakening because of asthma that required rescue medication use, and an increase in total asthma symptom score of ≥2 units above the screening average (or the maximum possible daily score of 6). Safety outcomes included adverse events and serious adverse events.
Statistical analysis
The primary analysis population for this subgroup analysis comprised Korean patients with baseline blood eosinophil counts ≥ 300 cells/µL in the overall SIROCCO trial. Efficacy data are not presented for the population with eosinophil counts < 300 cells/μL because of the small sample size. Annual exacerbation rates were estimated using a negative binomial model that included treatment, number of exacerbations in the previous year, and use of maintenance OCS as covariates. Least squares mean changes from baseline in FEV1 compared with placebo were estimated using a mixed-effects model for repeated measures analysis, with adjustment for treatment, baseline prebronchodilator FEV1, use of maintenance OCS, visit, and visit by treatment interaction. Least squares mean changes from baseline in biweekly average total asthma symptom score compared with placebo were also estimated using a mixed-effects model for repeated measures analysis, with adjustment for treatment, baseline total asthma symptom score, use of maintenance OCS, visit, and visit by treatment interaction. Because these analyses were not part of the formal testing strategy, all P values were nominal. Adverse events were summarized using descriptive statistics. All data analyses were conducted using SAS system version 9.2 or later (SAS Institute Inc., Cary, NC, USA).
RESULTS
Patients
Overall, 2,681 patients participated in the SIROCCO trial. Of these, 177 were Korean, with 122 randomly assigned to receive benralizumab or placebo (Fig. 2). Treatment was completed by 116 Korean patients, with 115 completing the trial. The most common reasons for treatment discontinuation (3 patients) and trial discontinuation (2 patients) were adverse events.
 | Fig. 2SIROCCO trial design: Korean patients.*Q4W, every 4 weeks; Q8W, every 8 weeks (first three doses Q4W).
*Unless indicated, values presented are for all patients regardless of blood eosinophil counts.
|
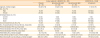
The mean (standard deviation) number of exacerbations experienced in the year before the trial was 3.6 (2.8), 3.1 (2.0), and 2.7 (1.1) for Korean patients receiving placebo, benralizumab Q4W, and benralizumab Q8W, respectively, compared with 2.9 (1.7) for the overall SIROCCO trial population (Table 1). Baseline demographics and clinical characteristics were similar between cohorts; however, the placebo group had more frequent OCS use and decreased lung function compared with the other cohorts, and the placebo and benralizumab Q4W cohorts had greater blood eosinophil counts than the Q8W cohort and overall SIROCCO trial population.
Table 1
Patient demographics and baseline clinical characteristics
FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; PN, predicted normal; Q4W, every 4 weeks; Q8W, every 8 weeks (first three doses Q4W); SD, standard deviation.
*Data not available for all Korean patients.
![]()
Efficacy
This analysis included Korean patients receiving high-dosage ICS/LABA with baseline blood eosinophil counts ≥ 300 cells/µL. Benralizumab reduced the annual asthma exacerbation rate by 70% with the Q4W regimen (rate 0.79 [95% confidence interval {CI}, 0.43–1.46], rate ratio 0.30 [95% CI, 0.13–0.65], nominal P = 0.003; n = 28) and by 85% with the Q8W regimen (rate 0.40 [95% CI, 0.19–0.82], rate ratio 0.15 [95% CI, 0.06–0.36], nominal P < 0.001; n = 30) compared with placebo (rate 2.67 [95% CI, 1.61–4.42]; n = 28) (Fig. 3 and Table 2). Prebronchodilator FEV1 increased with benralizumab by 0.270 L (Q4W: 95% CI, 0.039–0.500, nominal P = 0.023; n = 28) and 0.362 L (Q8W: 95% CI, 0.143–0.582, nominal P = 0.002; n = 30) relative to placebo (n = 27) at week 48 from baseline (Fig. 4 and Table 2). Improvements in FEV1 with benralizumab vs. placebo were observed as early as 4 weeks after treatment and were maintained throughout the study (Fig. 4). Total asthma symptom score was similar for both benralizumab Q4W (−0.27 [95% CI, −0.83 to 0.30], nominal P = 0.356; n = 27) and benralizumab Q8W (0.10 [95% CI, −0.44 to 0.65], nominal P = 0.708; n = 30) compared with placebo (n = 28) at week 48 from baseline (Fig. 5 and Table 2).
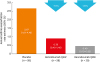 | Fig. 3Effect of benralizumab on annual asthma exacerbation rates for Korean patients with baseline blood eosinophil counts ≥ 300 cells/μL receiving high-dosage ICS/LABA.CI, confidence interval; ICS, inhaled corticosteroids; LABA, long-acting β2-agonists; Q4W, every 4 weeks; Q8W, every 8 weeks (first three doses Q4W).
*Estimates calculated via a negative binomial model with adjustment for treatment, oral corticosteroid use, and prior exacerbations.
|
Table 2
Summary of efficacy results for Korean patients in SIROCCO receiving high-dosage ICS/LABA with blood eosinophil counts ≥ 300 cells/μL

CI, confidence interval; EOT, end of treatment; FEV1, forced expiratory volume in 1 second; ICS, inhaled corticosteroids; LABA, long-acting β2-agonists; LS, least squares; Q4W, every 4 weeks; Q8W, every 8 weeks (first three doses Q4W).
*Estimates calculated via a negative binomial model with adjustment for treatment, oral corticosteroid use, and prior exacerbations. All P values are nominal; †Estimates calculated using a mixed-effects model for repeated measures analysis, with adjustment for treatment, baseline value, oral corticosteroid use at time of randomization, visit, and visit × treatment.
![]()
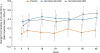 | Fig. 4Effect of benralizumab on prebronchodilator FEV1 for Korean patients with baseline blood eosinophil counts ≥ 300 cells/µL receiving high-dosage ICS/LABA.BD, bronchodilator; CI, confidence interval; FEV1, forced expiratory volume in 1 second; ICS, inhaled corticosteroids; LABA, long-acting β2-agonists; Q4W, every 4 weeks; Q8W, every 8 weeks (first three doses Q4W).
*Estimates calculated using a mixed-effects model for repeated measures analysis, with adjustment for treatment, baseline value, oral corticosteroid use at time of randomization, visit, and visit × treatment.
|
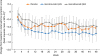 | Fig. 5Effect of benralizumab on total asthma symptom score for Korean patients with baseline blood eosinophil counts ≥ 300 cells/μL receiving high-dosage ICS/LABA.CI, confidence interval; ICS, inhaled corticosteroids; LABA, long-acting β2-agonists; Q4W, every 4 weeks; Q8W, every 8 weeks (first three doses Q4W).
*Estimates calculated using a mixed-effects model for repeated measures analysis, with adjustment for treatment, baseline value, oral corticosteroid use at time of randomization, visit, and visit × treatment; †Scored 0–6; decreasing score indicates improvement in symptoms.
|
Safety
Overall, 100 of the 122 (82%) Korean patients experienced 1 or more adverse events (Table 3). The most common adverse events were upper respiratory tract infection (38 patients) and nasopharyngitis (26 patients). The majority of adverse events were not considered related to benralizumab treatment. Adverse events resulting in discontinuation of treatment occurred in 2 patients who received benralizumab (both Q4W, asthenia and cerebral hemorrhage) and 1 patient who received placebo (injection site erythema). Serious adverse events were reported for 9 patients who received benralizumab compared with 11 who received placebo. One patient who received benralizumab Q4W died from cerebral hemorrhage, which was considered to be not related to treatment.
Table 3
Summary of adverse events (safety analysis set)
Values are presented as number (%).
AE, adverse event; Q4W, every 4 weeks; Q8W, every 8 weeks (first three doses Q4W).
*One discontinuation was considered treatment related by the principal investigator (asthenia); †Death (cerebral hemorrhage) was considered not treatment related.
![]()
DISCUSSION
This subgroup analysis evaluated the efficacy and safety of benralizumab 30 mg for Korean patients who participated in the Phase III SIROCCO trial. We found that 48 weeks of benralizumab treatment substantially decreased asthma exacerbations and increased lung function for Korean patients with baseline blood eosinophil counts ≥ 300 cells/µL receiving high-dosage ICS/LABA. For FEV1, improvements relative to placebo were observed by week 4 of treatment. Asthma symptom improvements with benralizumab treatment were variable, potentially related to the small sample size.
The 85% reduction in exacerbation rate and 0.362-L improvement in lung function with benralizumab Q8W for Korean patients relative to placebo were consistent with those reported for the overall SIROCCO population with blood eosinophil counts ≥ 300 cells/μL (Table 4).15 In the overall trial population, annual asthma exacerbation rates improved by 45% and 51% with benralizumab Q4W and Q8W, respectively, compared with placebo. Prebronchodilator FEV1 was increased with benralizumab Q4W and Q8W in the overall trial population by 0.106 L and 0.159 L, respectively, compared with placebo at week 48 relative to baseline. Improvements in FEV1 with benralizumab relative to placebo occurred by week 4 of treatment. Total asthma symptom score improved with both dosages of benralizumab relative to placebo by −0.08 (Q4W) and −0.25 (Q8W).
Table 4
Summary of efficacy results for patients receiving high-dosage ICS/LABA with baseline blood eosinophil counts ≥ 300 cells/μL in the Korean and overall SIROCCO trial populations (benralizumab vs. placebo)

| Korean patients in SIROCCO* | SIROCCO overall patient population15 | |||
|---|---|---|---|---|
| Benralizumab Q4W (n = 28) | Benralizumab Q8W (n = 30) | Benralizumab Q4W (n = 275) | Benralizumab Q8W (n = 267) | |
| Reduction in annual exacerbation rate (%) | ↓70‡ | ↓85† | ↓45† | ↓51† |
| Increase in prebronchodilator FEV1 (L) | ↑0.270§ | ↑0.362‡ | ↑0.106§ | ↑0.159† |
| Change in total asthma symptom score | ↓0.28 | ↑0.07 | ↓0.08 | ↓0.25§ |
FEV1, forced expiratory volume in 1 second; ICS, inhaled corticosteroids; LABA, long-acting β2-agonists; Q4W, every 4 weeks; Q8W, every 8 weeks (first three doses Q4W).
*All P values are nominal; †P value < 0.001; ‡P value ≥ 0.001 to ≤ 0.01; §P value > 0.01 to ≤ 0.05.
![]()
The results of this analysis build on previous benralizumab studies with Asian patients.1819 In a Phase IIa dose-ranging study conducted with Korean and Japanese patients, asthma exacerbations were reduced by 61%, 61%, and 40% after 52 weeks of treatment with benralizumab 2, 20, and 100 mg, respectively, vs. placebo for patients with baseline blood eosinophil counts ≥ 300 cells/µL.18 Decreased asthma exacerbation rates also were accompanied by increased FEV1 and depletion of blood eosinophils. In an analysis of Japanese patients from the Phase III CALIMA trial, the annual rate of asthma exacerbations was reduced by 66% and 83% with benralizumab Q4W and Q8W, respectively, for patients with blood eosinophil counts ≥ 300 cells/µL relative to placebo.19 Prebronchodilator FEV1 improved for these patients by 0.334 L and 0.198 L with benralizumab Q4W and Q8W, respectively, after 56 weeks of treatment vs. placebo.
Benralizumab was well-tolerated by Korean patients with a safety profile comparable with that experienced by the overall population in the SIROCCO trial.15 The most common adverse events in SIROCCO were asthma worsening and nasopharyngitis, whereas the most common adverse events for Korean patients were upper respiratory tract infection and nasopharyngitis. One death occurred in the benralizumab Q4W cohort, which was not considered treatment related.
Overall, our findings suggest that benralizumab efficacy in reducing exacerbations and improving lung function is equal, if not better, for Korean patients than for the overall SIROCCO population with blood eosinophil counts ≥ 300 cells/μL. Because of the small sample size (86 patients) and differences in baseline clinical characteristics between cohorts, larger studies would be needed to confirm that benralizumab has greater efficacy for this patient population. Similarly, further studies are needed to explore if asthma symptoms improve with benralizumab treatment for Korean patients as reported for the overall SIROCCO population and to verify the reported safety profile. Because of the small sample size, the efficacy of benralizumab for patients with blood eosinophil counts < 300 cells/μL could not be evaluated. Benralizumab efficacy has been demonstrated for patients with blood eosinophil counts < 300 cells/μL in studies using pooled results from SIROCCO and CALIMA.2021 Studies of this Korean patient population with blood eosinophil counts < 300 cells/μL, along with additional biomarkers for eosinophilic airway inflammation, would need to be performed to confirm benralizumab efficacy for these patients.
Consistent with findings for the overall SIROCCO population, benralizumab 30 mg Q4W and Q8W decrease asthma exacerbations and improve lung function with acceptable safety profiles for Korean patients with severe, uncontrolled eosinophilic asthma.
 XML Download
XML Download