

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Food allergy is an adverse food reaction arising from a specific immune response that occurs reproducibly on exposure to a certain food, including immunoglobulin E (IgE)-mediated, non-IgE-mediated, mixed, or cell-mediated reactions.1 Food allergies are more common in children than in adults.23 The prevalence of food allergies in children tends to increase gradually, and based on the data released by the American Centers for Disease Control in 2013, the prevalence rate of food allergy in children aged 0–17 years was 3.4% from 1997 to 1999, which increased to 5.1% from 2009 to 2011.4 In Korea, the prevalence rate of food allergy increased from 0.6% to 3.15% in children aged 6–7 years and from 1.6% to 4.01% in children aged 12–13 years between 2010 and 2015.56 IgE-mediated food allergies can cause symptoms such as acute urticaria, angioedema, atopic dermatitis and asthma, as well as anaphylactic reactions. With regard to the treatment of food allergies, the intake of food that caused allergic reactions should be avoided.17 However, several food allergens are difficult to avoid because they are ingested in different forms through food processing, which can cause an accidental exposure.78
Egg is one of the most common allergens in children, accounting for 0.5%–2.5% of allergies in children.9101112 An Australian study reported that the prevalence of IgE-mediated egg allergy in infants aged 12 months is 9%.13 Egg is also the most important cause of food allergy among single foods in Korea.514 In 1995, based on the Food Allergen Cause Report, 22.7% of children with food allergy had egg allergy.15 A recent questionnaire survey on children aged 0 to 6 years was conducted in 2014, and 20% of children with food allergy complained of egg allergy.16
Most egg allergy develops in the first year of life and the overall prognosis for tolerance has been considered good.1718 However, tolerance acquisition rates have been varyingly reported as 30%–50% by age of 3 years, 59%–66% by age of 5 years and 50%–70% at age of 6 years.192021 The median time to develop tolerance has been reported to be from 3 to 9 years of age, and 5%–10% of children reported that their egg allergy persisted until 18 years of age.192122 Therefore, prediction of future tolerance is useful for planning whether to apply interventions, such as oral immunotherapy, and providing individualized insights into prognostication. The prognostic factors associated with the egg allergy tolerance acquisition have been reported to include the following: characteristics of the initial reaction at the time of egg consumption, baseline egg skin prick test wheal size, and baseline egg-specific IgE level at diagnosis.1192021
Here, we sought to compare clinical characteristics between tolerant and persistent groups of children with egg allergy, and to identify an early predictor for future tolerance in children with IgE-mediated egg allergy.
MATERIALS AND METHODS
This was a retrospective clinical study of children who underwent egg white-specific immunoglobulin E (EWsIgE) testing twice or more at Severance Children's Hospital, Seoul, Republic of Korea, between November 2005 and November 2015. Of 960 children, 430 were diagnosed as having egg allergy and were included in this study. Among them, 226 were excluded because we could not confirm whether they acquired tolerance or not until their last visit based on the medical records. The remaining 124 children were enrolled.
Egg allergy was defined as follows: reports by a guardian of allergic reaction after eating eggs and an EWsIgE level of > 0.35 kU/L.123 Other food allergies were defined as follows: reports by a guardian of allergic reaction after consumption of the relevant food and the specific IgE level of > 0.35 kU/L. The participants were divided into “tolerant” and “persistent” groups according to tolerance acquisition. Tolerance acquisition was defined as 1) a negative result from an open food challenge test conducted in the hospital using 1 whole cooked egg24 or 2) no allergic reaction after ingesting eggs at home under the direction of a physician. The open food challenge test was performed in 34 (27.4%) patients.
The patients' sex, age, allergy history (atopic dermatitis, allergic rhinitis, asthma and other food allergies), family history of allergy (atopic dermatitis, allergic rhinitis, asthma and other food allergies), and other characteristics (history of breastfeeding, pets in the home and passive smoking) were collected using medical records. In each case, total serum IgE levels at the time of diagnosis and repeated EWsIgE levels from diagnosis until the end of the observation period were determined. To calibrate the EWsIgE test performed at irregular intervals, the reduction rate of the EWsIgE level was calculated at intervals of 12 months (ΔEWsIgE12mo), and the following formula was used:
ΔEWsIgE12mo (%) = [{(First value−second value)/first value}Interval from the first to the second date (months)×12]×100
Allergen-specific IgE and total serum IgE were measured using the ImmunoCAP system (Thermo Fisher, Uppsala, Sweden). The study design was approved by the Institutional Review Board (IRB) of Severance Hospital. The requirement for informed consent was waived due to the retrospective nature of the study (No. 4-2016-0779).
For the analysis in this study, we used SPSS version 23.0 for Windows (SPSS Inc., Chicago, IL, USA) and R version 3.2.2 (The R Foundation for Statistical Computing, Vienna, Austria). The Mann-Whitney and χ2 tests were used to compare the characteristics of the 2 groups. The linear mixed-model method was applied to compare EWsIgE values over time. Logistic regression analysis was used to plot receiver-operating characteristic (ROC) curves, and the predictive power of EWsIgE levels at diagnosis (EWsIgEdiag), ΔEWsIgE12mo and peak EWsIgE to predict egg allergy tolerance acquisition were analyzed. Each cutoff value in the ROC curve was calculated using the Youden index. The survival analysis using the Kaplan-Meier curve was used to determine whether the predictor could effectively predict tolerance acquisition.
RESULTS
Tolerance to egg allergy compared to persistent egg allergy
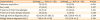
Of a total of 124 children, egg allergy resolved in 101 (81.5%) children at a median age of 34 months. Median follow-up duration was 49.0 (range, 32.0–127.0) months in the persistent group, and the median duration to acquire tolerance was 18.0 (range, 8.0–61.0) months in the tolerant group. No significant differences were found between the 2 groups in age at diagnosis and sex. Of 64 (51.6%) children with other food allergies, wheat (26.1% vs. 5.9%; P = 0.009) and peanut (34.8% vs. 11.9%; P = 0.012) allergies were more frequent in the persistent group than in the tolerant group. Of 90 (72.6%) children with other allergic diseases, the persistent group (87.0%) had more atopic dermatitis compared to the tolerant group (66.3%; P = 0.039). No significant difference was found between the 2 groups in terms of the presence of parental allergic diseases and breastfeeding (Table 1).
Table 1
Subjects' characteristics

Data were expressed as median (interquartile range) or number (%).
IgE, immunoglobulin E.
*The P < 0.05.
![]()
Baseline EWsIgE levels and their trends between the persistent and tolerant groups
The median EWsIgEdiag was higher in the persistent group (median [interquartile range; IQR], 21.12 [9.99–66.12] kU/L) than in the tolerant group (median [IQR], 7.71 [4.51–15.40] kU/L; P = 0.001; Fig. 1A). The peak EWsIgE level during the individual follow-up period was also higher in the persistent group (median [IQR], 49.45 [17.87–100.00] kU/L) than in the tolerant group (median [IQR], 7.86 [4.54–17.1] kU/L; P < 0.001; Fig. 1B). The trends of repeated EWsIgE levels showed that the EWsIgE levels in the tolerant group decreased markedly over time compared to those in the persistent group (P < 0.001; Fig. 2).
 | Fig. 1The EWsIgE level at diagnosis between persistent and tolerant groups. The EWsIgE level at diagnosis was higher in the persistent group than in the tolerant group (A) median (interquartile range), 21.12 (9.99–66.12) kU/L vs. 7.71 (4.51–15.40) kU/L; P = 0.001). The peak EWsIgE level during the individual follow-up period also was higher in the persistent group than in the tolerant group (B) 49.45 (17.87–100.00) kU/L vs. 7.86 (4.54–17.1) kU/L; P < 0.001).EWsIgE, egg white-specific IgE.
|

The ΔEWsIgE12mo as a predictor of egg allergy tolerance
When EWsIgEdiag and ΔEWsIgE12mo were compared for their predictive power for allergy tolerance acquisition, ΔEWsIgE12mo (area under the curve [AUC], 0.835; 95% confidence interval [CI], 0.763–0.907) tended to show better performance than EWsIgEdiag (AUC, 0.731; 95% CI, 0.609–0.853); however, there was no statistically significant difference (P = 0.169). The cutoff values were 16 kU/L for EWsIgEdiag and 30% for ΔEWsIgE12mo. The predictive power of using both ΔEWsIgE12mo and EWsIgEdiag (AUC, 0.805; 95% CI, 0.718–0.891) showed similar performance to using EWsIgEdiag (P = 0.192) or ΔEWsIgE12mo alone (P = 0.255; Table 2). The Kaplan-Meier curves showed more egg allergy tolerance acquisition in the group with ΔEWsIgE12mo of ≥ 30%. In addition, we performed the analysis in the subgroup with a high EWsIgEdiag of > 23.0kU/L, which was the level of 75th percentile in all participants, and confirmed that ΔEWsIgE12mo of ≥ 30% produced a similar result (Fig. 3).
Table 2
Prediction model of egg allergy tolerance acquisition

AUC, area under the curve; CI, confidence interval; EWsIgEdiag, egg white-specific IgE level at diagnosis; ΔEWsIgE12mo, reduction rate of egg white-specific IgE level after 12 months from diagnosis.
![]()
 | Fig. 3Comparison of the incidence of egg allergy tolerance acquisition according to ΔEWsIgE12mo using the Kaplan-Meier curve. More children with ΔEWsIgE12mo of ≥ 30% acquired tolerance than those with ΔEWsIgE12mo of < 30% among all the participants (A) and in the subgroup with high EWsIgE levels (> 23.0 kU/L) at diagnosis (B).ΔEWsIgE12mo, reduction rate of EWsIgE level after 12 months from diagnosis; EWsIgE, egg white-specific IgE.
|
The patients were further divided based on the cutoff ΔEWsIgE12mo value of 30% to perform additional analysis; 86 (69.4%) had a ΔEWsIgE12mo of ≥ 30% and 38 (30.6%) had a ΔEWsIgE12mo of < 30%. Of the children with a ΔEWsIgE12mo of ≥ 30%, 79 (91.9%) had acquired egg allergy tolerance, whereas of the children with a ΔEWsIgE12mo of < 30%, only 22 (57.9%) had acquired tolerance (P < 0.001; Table 3).
Table 3
Subjects' characteristics divided by the cutoff of ΔEWsIgE12mo
Data were expressed as median (interquartile range) or number (%).
ΔEWsIgE12mo, reduction rate of EWsIgE level after 12 months from diagnosis; IgE, immunoglobulin E; EWsIgE, egg white-specific IgE.
![]()
DISCUSSION
This study compared clinical characteristics between groups of children with tolerance to egg allergy and persistent egg allergy, and suggested an early predictor for future tolerance in children with IgE-mediated egg allergy. The group with persistent egg allergy had more other food allergies and more atopic dermatitis compared to the tolerant group. The EWsIgEdiag and the peak EWsIgE were higher in the persistent group than in the tolerant group. The trend of the EWsIgE levels over time in the tolerant group decreased markedly compared to that in the persistent group. We propose ΔEWsIgE12mo as an early predictor for future tolerance. It tended to show better performance than the EWsIgEdiag and the peak EWsIgE, and comparable performance to the combination of ΔEWsIgE12mo and EWsIgEdiag.
Egg allergy resolved in half of the children at the median age of 6 years; however, a wide range from 2 to 9 years has been reported for the age at resolution. The review by Savage et al.18 revealed that the differences in resolution rates and ages in each study were due to the different study designs, and definitions of egg allergy and development of tolerance. The resolution rate most likely depended on the definition of development of tolerance including the method of food challenge test.212225 In this study, 81.5% of children developed tolerance to egg by the median age of 3 years. The resolution rate was much higher compared to the previous study, a retrospective study in a tertiary referral clinic with similar criteria of egg allergy and development of tolerance, which reported that only 19% of children acquired tolerance to egg allergy by age 4 years.22 Forty percent of Korean children with atopic dermatitis26 and 30% of Japanese children20 had tolerance to egg by the age of 3 years. These Asian studies reported favorable resolution rates of 70% by the age of 6 years and 85% by the age of 10 years compared to the previous Western studies.212225 The differences may be due not only to different populations but also different lifestyles including dietary habits.
Persistence of egg allergy has been associated with more severe symptoms,1921 the presence of other allergic diseases and their severity.2122 The clinical characteristics associated with the natural history of egg allergy in this study were presence of other food allergies and atopic dermatitis. More than half of the children had other food allergies and children with comorbid peanut or wheat allergies had persistent egg allergy. Eighty percent of children had other comorbid allergic diseases and the majority was atopic dermatitis. Our results showed that comorbid atopic dermatitis in children with egg allergy was an indicator of poor prognosis, which is consistent with other studies, while the resolution rate in our study was much higher compared to that of previous studies that reported lower resolution rates in children with atopic dermatitis.2122 We collected participants’ information using only medical records and excluded more than half of the children due to insufficient information on tolerance acquisition, which might have skewed the resolution rate.
Larger skin prick test wheal size1921 or high egg-specific IgE levels21222728 were associated with persistent egg allergy. Moreover, we showed that the EWsIgEdiag and the peak EWsIgE were higher in the persistent group than in the tolerant group. The EWsIgEdiag has been suggested as a predictor of tolerance acquisition. Tolerance acquisition was reported to be significantly delayed when the baseline egg-specific IgE level was ≥ 6.2 kU/L29 or ≥ 10 kU/L,21 and failed in almost all children when the peak egg-specific IgE level was ≥ 50 kU/L.22 In this study, the EWsIgEdiag level of ≥ 16 kU/L was less likely to resolve egg allergy by the age of 3 years, and with a relatively insufficient AUC, it cannot be used as a predictor. There were 24 (19.4%) children with peak egg-specific IgE level ≥ 50 kU/L; however, only half had persistent egg allergy. For the next step, we compared the trends of EWsIgE between the tolerant and persistent groups and found that the EWsIgE levels decreased markedly over time in the tolerant group compared to those in the persistent group. Therefore, we tested ΔEWsIgE12mo as an early predictor for future tolerance and confirmed that its performance tended to be better than the EWsIgEdiag based on the cutoff ΔEWsIgE12mo value of 30% with a sufficient AUC regardless of the EWsIgEdiag. Small sample size, a limitation of this study, might be attributed to the failure in reaching statistical significance. Our results were consistent with those of Shek et al.30 who reported that the rate of decrease in EWsIgE over time was significantly related to the probability of developing egg allergy tolerance, and the probability of developing tolerance due to decreased EWsIgE level was 52% for a 50% reduction and 78% for a 90% reduction. However, the ΔEWsIgE12mo value of 30% would be easy to use by applying simple mathematics in clinics.
It is important to predict which children with egg allergy are likely to have persistent allergy because it is necessary to identify the candidates for emerging food allergy therapies including oral immunotherapy, which can carry risks and be costly. If we predict tolerance to egg, then regular consumption of baked egg, if tolerated, can be recommended to accelerate the development of tolerance to less cooked egg.25 Thus, IgE epitope specificity,31 IgE/IgG4 ratio,32 and specific IgA and IgA233 have been associated with the development of tolerance; however, assays for these are less readily available. Allergen component-resolved diagnostics34 and cellular-based assays353637 may be candidates in predicting the natural course of food allergy.
This study had a few limitations. Firstly, this study was conducted retrospectively in a single tertiary clinic; thus, the children did not participate in the study at a similar time, and each medical observation schedule varied. Therefore, we reinforced this by using more effective statistical methods stepwise and by conducting an additional subgroup analysis. Secondly, we did not perform double-blind, placebo-controlled food challenges for all subjects to diagnose egg allergy and check for tolerance acquisition, which is the gold standard. To overcome these limitations, the criteria for diagnosis and tolerance acquisition proposed in this study were applied more strictly to the medical record review, and the open challenge test was used as a tolerance acquisition confirmation method. Therefore, we excluded more than half of the children due to insufficient information on tolerance acquisition, which might have led to overestimating the egg allergy resolution rate. However, this is a real-world practical study, which on the other hand, can be a strength of this study. Another limitation was a variable and relatively short follow-up period. For example, the shortest follow-up duration was 29 months in the persistent group, which is an insufficient time to confirm a persistent egg allergy, and can be a factor in underestimating the egg allergy resolution rate.
In conclusion, children with egg allergy are less likely to have tolerance to egg when they show concomitant allergies to other food, atopic dermatitis, or EWsIgE level of ≥ 16 kU/L at diagnosis. We suggest ΔEWsIgE12mo as a good independent predictor for future tolerance in children with IgE-mediated egg allergy.
 XML Download
XML Download