

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Size matching of the portal vein (PV) between the recipient and liver graft is important in preventing anastomotic stenosis in living donor liver transplantation (LDLT). In LDLT using a right liver graft, the diameter of right liver graft PV is usually >10 mm, thus PV size matching does not become a critical problem in adult recipients. If the recipient PV is small, unification venoplasty of two PV braches can be applied.1 If the recipient PV is very large, a funneling fence can be attached to the graft PV for easy anastomosis.2 However, if the diameter of graft PV is <8 mm, it can induce anastomotic stenosis even though a growth factor is fully given at the suture material. We have experienced a few cases of PV anastomotic stenosis so far due to small-sized graft PV in >5000 LDLT cases, but graft PV widening was not performed because graft PV is considered as being a no-touch area.
In thinking out of the box, we performed wedged-patch venoplasty to an exceptionally narrow graft PV to cope with PV size mismatching in LDLT. We herein present the case and describe the surgical technique of wedged-patch venoplasty.
CASE
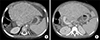
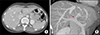
A 14 kg-weighing 4 year-old female patient underwent second LDLT due to progressive deterioration of graft function for 3 years (Fig. 1). The first LDLT operation was performed due to biliary stresia at age of 11 months and the donor was her mother. At the second LDLT, the donor was the 35 year-old sister of her mother and a 350 g-weighing whole left liver with middle hepatic vein trunk was harvested. The left liver graft PV was only 6 mm, because the left PV was waisted at the first-order PV (Fig. 2).
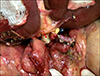
In contrast, the diameter of the recipient PV was 12 mm because an iliac vein conduit was interposed to cope with portal hypoplasia at the first LDLT operation (Fig. 1). To resolve this graft PV waist-associated size mismatching, a longitudinal incision was made at the graft PV stump to release the waist. A small cold-preserved fresh iliac vein patch was attached to widen the graft PV orifice (Fig. 3). The size of patch was adjusted to match with the size of the recipient PV.
In addition to the PV venoplasty, the left and middle hepatic vein orifices were unified, and a vein patch was attached to the middle hepatic vein side to widen the conjoined outflow orifice according to our standardized LDLT procedures (Fig. 4).
Graft implantation was uneventful, along the orders of hepatic vein anastomosis under total occlusion of the inferior vena cava, end-to-end portal vein anastomosis, portal reperfusion, hepatic artery anastomosis under surgical microscopy and hepaticojejunostomy using the previously made jejunal limb (Fig. 5). For hepatic vein and PV reconstruction, we used continuous running sutures using 5-0 and 6-0 polydioxanone (PDS) respectively. We have do not applied interrupted sutures combined with continuous running sutures using polypropylene (Prolene).
The patient recovered uneventfully and is doing well to date for 6 months. The portal vein showed a streamlined configuration without anastomotic stenosis after the second LDLT operation (Fig. 6).
DISCUSSION
In pediatric LDLT, PV stenosis is one of the most common and most critical complications. Patients with biliary atresia have suffered from periportal inflammation and fibrosis due to recurrent cholangitis, by which the recipient PV becomes hypoplastic and sclerotic PV.34 To cope with such an intractable PV anatomy, we adopted an interposition graft for PV reconstruction.5 The favorable long-term result of PV interposition graft was shown at the time of retransplantation operation in this case.
In this case, graft PV was smaller than the recipient PV. Such size mismatching of PV is often encountered in adult LDLT because of aneurysmal dilatation of recipient PV. In most cases of adult LDLT using a right liver graft, direct anastomosis of PVs is often feasible despite presence of considerable size discrepancy. If the recipient PV is too large to perform direct anastomosis, a funneling fence can be attached to the graft PV for easy anastomosis.2 However, if the diameter of right liver graft PV is <8 mm, it can induce anastomotic stenosis even though a growth factor is fully given at the suture material. We have experienced a few cases of PV anastomotic stenosis so far due to small-sized graft PV in >5000 LDLT cases, but graft PV widening was not performed because graft PV is considered as being a no-touch area.
In donor liver anatomy of this case, the native left PV has a waist at its first-order level, which is an unusual finding. Since manipulation of the single graft PV is usually unnecessary, we have considered it as a no-touch area. Meanwhile, unification of two graft PV orifices is a standard procedure.678910 In thinking out of the box, we performed wedged-patch venoplasty to exceptionally narrow graft PV. The surgical technique for wedged-patch venoplasty is intuitive and simple because we accumulated similar experience on graft hepatic vein venoplasty, as shown in this case.11 The lesson learned from this case can be applied to adult LDLT cases which has an unusually small graft PV.
In conclusion, we believe that this wedged-patch venoplasty technique can be applied to small-sized graft PV to cope with PV size mismatching in LDLT.



 XML Download
XML Download