

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Pregnancy has been considered as a contraindication in pulmonary arterial hypertension (PAH) patients because of the high morbidity and mortality rates of both mother and fetus.1)2)3) Even though doctors do not recommend pregnancy and provide repeated warnings and education on avoiding pregnancy in PAH women, there are always some cases of pregnancy maintained by chance or intentionally. Therefore, a doctor's recommendation has limitations in real world communication, and clinicians should be aware of pregnancy in PAH and how to help patients to achieve a better outcome.
Although the data on the pregnancies of PAH patients are limited, clinical management has been attempted to save the patients and their fetuses.4) During the past decades, the treatment of PAH has been rapidly developed with the introduction of targeted therapy for PAH and advances in intensive fetal care, and clinical experiences about maternal care in patients with PAH have been shared.5)6) Also, multidisciplinary team approach treatment with obstetricians, cardiologist, anesthesiologists, and neonatologists for pregnancy in PAH patients provided improvements to the morbidity and mortality of the patients.5) As a result, the survival of PAH patients has been improved compared with the previous era.3)
We report on a single center's successful experience in 10 cases of pregnant patients with PAH and discuss their comprehensive management.
Methods
The study was conducted as a pulmonary hypertension registry in a single center (Samsung Medical Center, Seoul, Korea) from 2011 to 2017. All pregnant women with diagnoses of PAH who decided to maintain their pregnancies after comprehensive familial consultations with physicians were included.
Clinical data were collected as follows: age, cause of PAH, underlying cardiovascular disease, and New York Heart Association (NYHA) functional classification at first visit. Laboratory tests included hemoglobin, hematocrit, creatinine, and N-terminal pro brain natriuretic peptide (NT-proBNP). The 6-minute walk test (6MWT) distance (m) and oximetry were also collected. Echocardiographic data were collected, including tricuspid annular plane systolic excursion (TAPSE), presence of pericardial effusion, right ventricular systolic pressure (RVSP) by Doppler tracing of tricuspid regurgitation, and mean pulmonary arterial pressure (PAP) by Mahan's equation. Obstetric data included gravidity and parity, gestational age at first visit and delivery, delivery methods, anesthesia during delivery, preterm labor, and any obstetrical complications. Fetal events, birth weight, and Apgar score were recorded. Medication during pregnancy and the peripartum period were described. Lengths of hospital stay and time in the intensive care unit (ICU) were also recorded. Pregnancy and peripartum complications were classified into cardiac and non-cardiac events. Cardiac events were defined as an aggravation of heart failure that required additional medication or admission, uncontrolled arrhythmia, and cardiac arrest. Non-cardiac events were defined as venous thromboembolism, major bleeding, and infection. Each patient gave informed consent to participate and the research was approved by the Institutional Review Board at Samsung medical center (IRB No. 2018-08-123).
Statistics
Baseline characteristics, obstetric data, and maternal and fetal outcomes were described as numbers and percentages for all PAH patients. Continuous variables were presented as medians and interquartile ranges. All statistical analyses were performed using SPSS Statistics 23.0 (SPSS, Chicago, IL, USA).
Results
Study population
This study enrolled 9 women, and 10 cases of labor were reviewed. Nine women maintained their pregnancies and underwent delivery. The underlying causes of PAH were as follows: 2 cases were PAH associated with atrial septal defect, 2 were Eisenmenger syndrome, another 2 were PAH associated with congenital heart disease (CHD) after surgical correction, and the others were idiopathic pulmonary arterial hypertension (IPAH), PAH associated with connective tissue disease, and hereditary PAH. CHD was surgically corrected in 2 patients at 5 (No. 3 in Table 1) and 7 (No.10 in Table 1) years old, respectively. The median maternal age was 28 (26–32) years old. The diagnosis of PAH had been established before pregnancy in 5 cases, and the others were recognized as PAH patients during pregnancy. Two women each had 2 pregnancies. One primipara (No. 9 in Table 1) was included in this study.
Table 1
Clinical characteristics at first visit during pregnancy
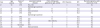
ASD = atrial septal defect; AVSD = atrioventricular septal defect; BMI = body mass index; CHD = congenital heart disease; CTD = connective tissue disease; HHT = hereditary hemorrhagic telangiectasia; IPAH = idiopathic pulmonary arterial hypertension; PDA = patent ductus arteriosus; SLE = systemic erythematosus lupus; VSD = ventricular septal defect; WHO = World Health Organization.
![]()
The timing of patients' initial visits to the PAH clinic was variable due to the time of diagnosis. At their initial visits, all of the patients were NYHA functional class II to III. Every patient had baseline oxygen saturation level above 89% at resting state, but 4 patients induced exertional hypoxia during 6MWT. While they were doing the 6MWT, the 2 patients with Eisenmenger syndrome had minimal oxygen saturation levels decrease to 69% and 78%, respectively. The median 6MWT distance was 387 (364–500) m.
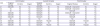
Transthoracic echocardiography (TTE) was used to diagnose and evaluate PAH at the initial visits. All patient had normal left ventricular (LV) cavity size and LV systolic function (Supplementary Table 1). The mean RVSP measure by TTE was 72 [55 – 93] mmHg, and the mean PAP was 43.7 (38.2–54.4) mmHg. Right ventricular (RV) function evaluated by TAPSE fell in the normal range in most patients, but echocardiographic results showed RV hypertrophy or RV dilatation or both findings. Half of the patients had an elevated NT-proBNP level ranging from 321 to 1,299 pg/mL. Further baseline characteristics are summarized in Tables 1 and 2.
Table 2
Laboratory findings and echocardiographic data at first visit to clinic

6MWT = 6-minute walk test; Cr = serum creatinine; Hb = hemoglobin; HCT = hematocrit; mPAP = mean pulmonary arterial pressure; NT-proBNP = N-terminal prohormone of brain natriuretic peptide; RVSP = right ventricular systolic pressure; TAPSE = tricuspid annular plane systolic excursion.
![]()
Maternal management during peripartum
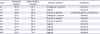
After their initial visits, the patients were strongly recommended to visit both the obstetrics clinic and the PAH clinic every month during the first trimester. They came in for a follow-up visit every 1 or 2 weeks beginning in the second trimester of pregnancy. The patients' symptoms, vital signs, NT-proBNP levels, and TTEs were regularly checked when they visited. All of the patients were treated with oral sildenafil (a phosphodiesterase type 5 inhibitor) from their initial visits until postpartum. Most of the PAH patients remained stable with sildenafil therapy alone during their first and second trimesters. However, 2 patients were treated with additional diuretics due to dyspnea and edema. Three patients were treated with additional continuous intravenous treprostinil in their third trimester periods. Only 1 patient received anticoagulation therapy during pregnancy. The 2 Eisenmenger patients who had hypoxia during the 6MWT received oxygen therapy. The patients with Eisenmenger syndrome, aggravated dyspnea, or decreased RV systolic function were considered the high-risk group. High-risk pregnant patients were admitted at the early period of the third trimester before labor pain. During their hospitalization, vital signs were monitored continuously, and TTE and NT-proBNP tests were performed every week. Detailed information is given in Table 3.
Table 3
Patient management during pregnancy
![]()
Delivery and postpartum care
Among the 10 completed pregnancies, 5 were delivered by caesarean section (C-section): 2 were emergency C-sections and 3 were elective C-sections. Each C-section was performed under general anesthesia by an anesthesiologist who is a specialist in cardiac anesthesia. The others were delivered by normal vaginal delivery under epidural anesthesia. After delivery, all of the patients stayed in the cardiac care unit for close monitoring and volume adjustment for at least 3 days. Furosemide was routinely administered intravenously for volume reduction, and spironolactone was added if furosemide had shown an insufficient diuretic effect. After delivery, most patients were treated with combination therapy for PAH in the postpartum period. Prostacyclin analogues (iloprost or treprostinil) or endothelin receptor antagonists (bosentan, ambrisentan, or macitetan) or both were added to sildenafil. Anti-embolic stockings were applied to all patients, and low-molecular-weight heparin or subcutaneous heparin was prescribed during the immediate postpartum period to prevent thromboembolism. Heparin was changed to warfarin before discharge and was continued for several months. Further data are summarized in Tables 4 and 5.
Table 4
Labor and delivery management
![]()
Table 5
Postpartum period (puerperium) care
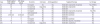
CCU = cardiac care unit; Furo = furosemide; HFNC = high flow nasal cannula; MV = mechanical ventilator; spiro = spironolactone.
![]()
Maternal and fetal outcomes
There was no maternal or fetal mortality. Cardiac events occurred in 6 cases, from significant aggravated heart failure to cardiogenic shock in a severe case. Severe complications occurred in one patient with Eisenmenger syndrome (No. 1 in Table 1), who experienced sudden cardiac arrest with ventricular fibrillation during her C-section and postpartum period. She recovered after successful cardiac resuscitation; however, because of recurrent ventricular tachycardia (VT), an implantable cardioverter defibrillator was inserted to prevent recurrent ventricular arrhythmia. Another patient with Eisenmenger syndrome (No. 4 in Table 1) had recurrent non-sustained VT episodes from 32 weeks of gestational age, and an emergency C-section was performed because of the increasing risk of fatal arrhythmia. Two patients (No. 2 and 10 in Table 1) needed inotropic support (dopamine) because of low blood pressure with high lactic acid over a day after delivery. (Table 6)
Table 6
Maternal and fetal outcomes
![]()
Non-cardiac events occurred in 3 cases. A postpartum bleeding event developed in one patient (No. 7 in Table 1). After full term spontaneous vaginal delivery at 40+6 weeks, the patient had postpartum bleeding due to uterine hypotonia. Her vital signs remained stable, but her hemoglobin level decreased from 11.2 to 9.1 g/dL. Ergonovine and fundus massage were added for the management of uterine hypotonia. Another patient (No. 4 in Table 1) suffered an uncomplicated urinary tract infection before delivery. In addition, pneumonia was suspected in one patient with Eisenmenger syndrome (No. 1 in Table 1).
Premature birth was the most common neonatal complication. The median gestational period was about 34 (32–38) weeks, and preterm labor occurred in 6 cases. Three cases were delivered at gestational age of 34 weeks considering the higher risk factor for fetal mortality, and the other 3 were unexpected preterm labor. They were delivered by emergency C-section. There was no fetal distress during delivery. There were 4 patients with severe hypoxia induced by the 6MWT (oxygen saturation under 90%); among them, 3 patients gave premature birth before 34 weeks of pregnancy, prior to completed fetal lung maturation. As mentioned earlier, there were no stillbirths in these series. During pregnancy, fetal growth was impaired in 4 pregnancies, and out of these 4, 3 neonates were low birth weight (<2,500 g) and 1 neonate was very low birth weight (1,500 g). In total, there were 6 low birth weight babies (<2,500 g). The median birth weight was 2.12 (1.74–2.79) kg. Further information is given in Table 5. Four neonates who were small for gestational age were treated in the neonatal ICU after delivery. The median number of admission days was 14.5 (minimum–maximum: 11–33 days). As in the present study, intrauterine growth restriction (IUGR) was significantly associated with preterm labor, low birth weight, and neonatal ICU care. Therefore, IUGR is considered a highly important predictor for fetal outcome. One neonate was reported to have non-cardiac anomalies of renal pelviectasia and an umbilical vein anomaly. Further information was summarized in Table 6.
The median follow-up duration after delivery was 3.2 (1.9–4.8) years. There was also no long-term mortality after delivery. However, heart failure which was associated aggravated pulmonary hypertension, was occurred in 2 of the patient (No. 3 and 6 in Table 1). Two women were admitted PAH clinic at 1 and 2 years after delivery, respectively. After received prostacyclin analogues or endothelin receptor antagonists, dyspnea was relieved. Finally, NYHA dyspnea class of all patient were remained in II–III at the same level as that in prepartum period.
Discussion
In this retrospective study from a single center registry, 9 pregnant women with PAH were included. Because PAH is a rare disease, this is a relatively large study of pregnancy in patients with PAH. Although 10 cases of pregnancy have been reviewed, our study included a broad spectrum of PAH patients in terms of the PAH cause and severity. Moreover, reporting on successful pregnancy outcomes in PAH patients in the current era of PAH-specific therapies has important significance.
Previous systematic reviews showed that pregnancy in women with pulmonary hypertension is associated with a high maternal mortality, estimated at between 30% and 56%.7) After the induction of the target therapy, maternal mortality for parturients with PAH has decreased over the past decades as compared with the previous era. Bedard et al. reported a systematic review of all cases of parturients with PAH published in a past decade (1997–2007), in which mortality decreased to 17–33% according to cause or type of PAH.8) Moreover, data from the Registry of Pregnancy and Cardiac Disease of the European Society of Cardiology was published in 2016. This cohort study included 151 women with pulmonary hypertension. Of these women, 39 (26%) had PAH, categorized into 3 subgroups: IPAH, PAH associated with CHD, or PAH associated with other diseases. No patients died during pregnancy, only 5 women (3.3%) died peripartum up to 1 week after delivery, and 2 additional deaths (2.6%) occurred within 6 months after delivery. Death occurred most frequently in the IPAH group.6) Because there were 7 patients in the IPAH group, and 3 deaths occurred in that group, the maternal mortality of IPAH was approximately 35%. Only 9 of 39 patients were treated with targeted therapy for PAH. It is not clear that maternal death occurred among those patients who were treated with targeted therapy. In our study population, all of the patients were group 1 PAH, and all of the patients were treated with PAH-specific drugs (8 of them before their peripartum periods and one of them immediately after delivery and in the postpartum period). The better outcomes of our patients were possibly related with targeted therapy.
The high maternal and fetal mortality in PAH patients is related to changes in cardiovascular physiology during pregnancy. The most remarkable hemodynamic change is expanded plasma volume.5) The plasma volume progressively increases starting at the early phase of pregnancy (6–8 weeks).9) Until the third trimester of pregnancy, blood volume increases to reach a maximum level of 50–70% above the patient's pre-pregnancy level.10)11)12) In addition, cardiac output (CO) increases in the first trimester and then gradually rises to peak values of 30–50% above the pre-pregnancy level.13) Multifactorial effects including expanded plasma volume, decreased afterload, eccentric hypertrophy, increased contractility, and heart rate are related to rising CO during pregnancy.2)14)15) To compensate for this blood flow requirement, pregnancy-related hormonal changes cause vasodilation. As a result, systemic vascular resistance and pulmonary vascular resistance (PVR) are decreased.1)2) Generally, the increase in plasma volume and CO and the decrease in PVR result in a grossly unchanged mean PAP. However, in the pregnant patients with PAH, these compensatory mechanisms have already been destroyed, resulting in a significant afterload stress on the right ventricle.5) Therefore, for women with PAH, the causes of poor maternal outcomes are variable, from worsening PAH and right heart failure to cardiogenic shock.2)16) Furthermore, the risk of these cardiac events is particularly high not only during the third trimester of pregnancy, but also in the delivery and postpartum period. During labor, additional blood volume is diverted from the uterus to the maternal circulation at each contraction, while blood loss due to hemorrhage and vasovagal response may lower the venous return.16) These opposing physiological changes cause significant, acute increases in CO (15–80%).17) In addition, anesthesia, infection, and thromboembolism in the postpartum period may put considerable stress on the maternal cardiovascular system. Therefore, postpartum care should be carefully performed under a multidisciplinary approach, and it would be better to share the patient's information before delivery. In our center, the cardiologist and obstetrician had a discussion immediately after each patient's decision to maintain the pregnancy, and this was shared with the anesthesiologist after 20 weeks of gestational age.
Current guidelines have declared that PAH patients should be counselled against pregnancy and therapeutic abortion should be recommended.3) However, pregnancy in the real world cannot be completely avoided, because patients do not always follow medical guidelines. As for inevitable case of continuing pregnancy, the medical team should do their best to reduce the morbidity and mortality. It would better than to leave the patients from clinics and returns at almost full term. The clinical outcomes of our center are remarkable results in consideration of previously reported studies in which the mortality rate of pregnant patients with PAH reached 28–56%.7)18)
The improvement of the clinical outcomes of our patients with PAH may be explained in several ways. First, 9 pregnancies received advanced pulmonary hypertension medication. A phosphodiesterase type 5 inhibitor (sildenafil) was given in all patients. Moreover, 3 of these 9 pregnant patients were administered a prostacyclin analogue (treprostinil). All of the patients were treated with dual therapy during the postpartum period. Second, a multidisciplinary team approach was applied during the peripartum period. Before delivery, the cardiologist, anesthesiologists, and obstetricians discussed the appropriate surgical procedure and anesthetic methods. In the case of high-risk pregnancy, invasive hemodynamic monitoring was performed. Defibrillator and percutaneous cardiopulmonary support were prepared for hemodynamic instability during operation. Third, the ICU was aggressively used for the management of high-risk pregnant patients with PAH. High risk patients were admitted to hospital in the third trimester for monitoring until postpartum and were sent to the critical care unit immediately after delivery for postpartum care.
However, there are several limitations in this study. First, this study was conducted in a single center, so the number of pregnant patients with PAH was relatively small. Second it is also notable that our patients were mostly NYHA functional class II, and had NT-proBNP levels less than 1,400. Low to intermediate risk patients, according to European Society of Cardiology guidelines, were the majority of this study. Pregnancy in more severely symptomatic PAH patients could have led to completely different consequences.
Although it is remarkable that no mortality occurred in the mothers or fetuses, more than half of patients were underwent cardiac events. Severe cardiac complications including cardiac arrest and recurrent VT also occurred in 2 cases of patients with Eisenmenger syndrome. Also, prematurity and low birth weight still remained significant neonatal complications. Therefore, pregnancy of patients with PAH should still not be allowed because of the high risk to mother and fetus. However, there is a possibility to improve the prognosis when applying maximal PAH targeted treatment in advance, multidisciplinary team management, and intensive care during the peripartum period in case of unavoidable pregnancy. Also, this management should be performed in the PAH specialized expert center.
In conclusion, the outcomes of pregnant patients with PAH have a possibility to be improved with PAH targeted therapy when compared to the previous era of hopelessness without treatment methods. However, it is remained unchanged that the women with PAH should be advice against pregnancy and therapeutic abortion should be recommended. The best medical support should be provided on an individual basis, only if a patient is determined to maintain her pregnancy in spite of medical advice. Multidisciplinary team approach management and intensive care were strongly recommended in case of inevitable pregnancy. Further experiences should be shared to improve the survival of mother and fetus.
 XML Download
XML Download