

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
More than 10% of the subjects, aged ≥75 years have moderate to severe mitral regurgitation (MR).1) From several population studies, severe MR is considered as an aging disease since the disease burden is higher in elderly subjects. Along with the prolonging of life expectancy, the trend of deaths related with valvular heart disease upstroke significantly in the past 3 decades.2) Patients with symptomatic severe MR, if left untreated, would experience progressive heart failure (HF), and the 5-year mortality rate could be as high as 50%.3) Although mitral valve repair or replacement is the standard treatment for severe MR, almost one-half of the patients were deferred to receive surgery in Euro Heart Survey.4) Moreover, up to 85% of the octogenarians refused or declined to receive open-heart surgery mainly because of advanced age. The expected number of underutilizations in mitral valve surgery could be higher in Asians due to culture differences between East and West. There is a clinical unmet need in treating severe MR properly especially in elderly subjects.
The transcatheter edge-to-edge mitral valve repair, using MitraClip (Abbott Vascular, Menlo Park, CA, USA), has been suggested as an alternative of mitral valve therapy for patient with severe symptomatic MR who carries high or prohibitive surgical risk.5) In the Endovascular Valve Edge-to-Edge Repair Study (EVEREST II), MitraClip has shown superior safety and acceptable durability up to 5-years in surgical eligible patients with severe MR.6)7) The safety and feasibility of MitraClip regarding to the improvements of clinical symptoms and exercise capacities as well as reverse remodeling effect has also been reported in the initial first 20 Taiwanese.8) On the other hand, the paucity of data in procedural safety and long-term clinical impact in elderly patients warrant further study to elucidate, especially in Asians.
In the present study, we retrospectively exam our cohort subjects who received trans-catheter mitral valve repair for severe MR in a single tertiary center. Octogenarians or even older patients were compared with younger subjects in respect of procedural outcomes and long-term clinical impact after receiving MitraClip.
METHODS
Study participants
Subjects with HF and severe MR were eligible for this study. All patients would undergo a standard diagnostic workup, including medical history taking, physical examinations, functional capacity assessments by the New York Heart Association (NYHA) classification and 6-minute walk test (6MWT). The echocardiogram, diagnostic coronary angiography, and right heart catheterizations were performed for pre-operative evaluation. The heart team would disclose the surgical risks and shared-decision-making process was applied for the choice of treatment. The standard patient flow was shown in Figure 1. Patients undergone trans-catheter mitral valve repair were enrolled in this analysis. The investigation conformed to the principles outlined in the Declaration of Helsinki. A written informed consent approved by our Institutional Review Board was obtained from each subject before enrollment.
Figure 1
Patients flow for management of patients with symptomatic severe MR.
DMR = degenerative mitral regurgitation; FMR = functional mitral regurgitation; GDMT = goal-directed medical treatment; MR = mitral regurgitation; SMVR = surgical mitral valve replacement/repair; TMVR = transcatheter mitral valve repair.

Study protocol
In addition to the pre-operative evaluations, patients would undergo repeated assessments for functional capacity and cardiac performance by transthoracic echocardiogram at 1, 6, and 12 months after the index procedure. Blood tests at fasting were also obtained for the measures of hemoglobin, serum creatinine, and N-terminal pro-B type natriuretic peptide (NT-proBNP) levels. All participants were followed in the clinics or by telephone contact every month for a year.
Echocardiographic measurements
All patients received a comprehensive Doppler and M-mode transthoracic echocardiography according to the recommendations of American Society of Echocardiography.9)10) Left ventricular ejection fraction (LVEF) were measured by biplane Simpson's method and the effective regurgitant orifice of MR were also calculated.11) The severity of MR was then graded as mild (grade 1), mild to moderate (grade 2), moderate to severe (grade 3), or severe (grade 4) accordingly.12) The etiology of MR is classified as degenerative MR (DMR; prolapsing leaflets or rupture chordae) and functional MR (consequence of annulus dilatation or abnormal left ventricular function).13)
Transcatheter mitral valve repair
The procedure was conducted under general anesthesia with the guidance of fluoroscopy and transesophageal echocardiography in a hybrid operative room. The techniques for trans-catheter mitral edge-to-edge repair have been described in detail.6) In brief, MitraClip was introduced into left atrium after the transseptal puncture to grasp the leaflets and minimize the regurgitation.
Clinical end points were defined according to the Mitral Valve Academic Research Consortium (MVARC).14) Procedural success was defined as a successful implantation of one or more clips to immediately reduce MR of less than grade 2.15) Procedure related complications of single leaflet detachment, myocardial infarction, stroke, major vascular complications, conversion to surgery, prolonged intubation for more than 48 hours, acute kidney injury were recorded accordingly. The procedure duration was defined as the time interval between start of vascular puncture and end of the vascular closure.
Statistical analysis
Means, standard deviations, and percentages were used to describe the characteristics of the study population. Independent t-test and χ2-test were used to compare the baseline characteristics between octogenarians and younger patients. Because of the skewed distribution, NT-proBNP was taken natural logarithm transformation (Ln) prior to the statistical analysis. Predictors of all-cause death among baseline characteristics, echocardiographic findings, blood test, and pre-procedure functional capacity variables were investigated using penalized logistic regression. Cumulative events rate at follow-up were plotted according to the Kaplan-Meier method and differences in survival and disease-free intervals were tested with the log-rank test. Statistical significances were set at p<0.05 and all statistical analyses were carried out using SPSS 15.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Patient characteristics
From May 2016 to January 2018, 430 patients with symptomatic severe MR visited our valve clinics. Among them, 105 patients underwent isolated mitral valve surgery and 279 patients received medical treatment along. A total of consecutive 46 patients treated with MitraClip were included in this analysis. Nineteen patients (84.2±4.0 years, 63% male) were over age of 80 years and 27 (73.4±11.1 years, 81% male) were younger than 80. The baseline characteristics were displayed in Table 1. The patients in both groups were characterized by high surgical risk (median European System for Cardiac Operative Risk Evaluation II [EuroSCORE II] of 10.2% and median Society of Thoracic Surgeons Predicted Risk of Mortality [STS-PROM] score of 7.3% for mortality), and multiple morbidities. As compare to younger group, there were more DMR (aged ≥80 years and <80 years, 68% vs. 37%, p=0.04) and having better left ventricular systolic function (LVEF, aged ≥80 years and <80 years, 54.9±11.3% vs. 44.4±15.2%, p=0.014) in the elderly group. All of the participants had severe MR with a mean effective regurgitation orifice of 49±21 mm2 and 94% of them were with NYHA functional class (Fc) III to IV symptoms.
Table 1
Baseline characteristics between the elderly and younger patients
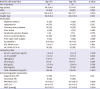
Values are presented as number (%) or mean±standard deviation.
Alb = serum albumin level; EROA = effective regurgitant orifice area; EuroSCORE II = European System for Cardiac Operative Risk Evaluation II; Glu = fasting blood glucose; HF = heart failure; HgB = hemoglobin; LVEF = left ventricular ejection fraction; MR = mitral regurgitation; Na = serum sodium level; NT-proBNP = N-terminal pro-B type natriuretic peptide; NYHA Fc = New York Heart Failure Association functional class; PASP = pulmonary artery systolic pressure; STS-PROM = Society of Thoracic Surgeons Predicted Risk of Mortality.
Procedure outcomes
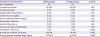
Among the 46 procedures, the procedures success rate was 95% in the elderly group and 93% in the younger group (p=1.00). There was no peri-procedure death, myocardial infarction, stroke or any adverse events requiring emergent cardiac surgery in both groups. There was no significant difference in vascular access complications, rate of using mechanical ventilation over 48 hours, and post-procedure hospital stays between groups (Table 2).
Table 2
Characteristics of the index procedure
Clinical improvements and 1-year follow-up
After the index procedure, the clinical symptoms and functional capacity were significantly improved with time. More than 80% of patients were with NYHA Fc I or II symptoms during follow-up, as opposed to only 13% of patients were with NYHA Fc I or II before intervention (Figure 2A). After fixing the MR, 94% of patients were with mild or mild to moderate degree of MR at 1 month and 92% of patients were remained mild or mild to moderate degree of MR at 1 year (Figure 2B). The Ln NT-proBNP level decreased from 7.6±1.2 to 7.3±1.2 at 1 month (n=40, p=0.004), 6.9±1.4 at 6 months (n=36, p<0.001), and further down to 6.6±0.8 (n=19, p=0.008) at 1 year (Figure 3A). The 6MWT increased from 259±114 to 313±107 meters (n=34, p=0.02) at 1 month, and up to 319±92 (n=16, p=0.03) at 1 year (Figure 3B). During follow-up period, 6 patients experienced death whereas 3 are cardiovascular mortality. The overall 1-year survival rate was 86% (80% in aged ≥80 years and 88% in those <80 years, p=0.590) (Figure 4A). There was also no difference in 1-year free from all-cause mortality or HF admission rate between 2 groups (70% in aged ≥80 years and 78% in those <80 years, p=0.738) (Figure 4B). By univariate analysis, pre-procedural 6MWT was a predictor of all-cause mortality (odds ratio [OR], 0.99; 95% confidence interval [CI], 0.982–0.999; p=0.026) after the MitraClip procedure but not age (OR, 1.12; 95% CI, 0.975–1.299; p=0.108) (Table 3).
Figure 2
(A) Results for NYHA Fc improvement before, 1, 6, and 12 months after clip implantation. (B) Results for MR reduction before, 1, 6, and 12 months after clip implantation.
NYHA Fc = New York Heart Failure Association functional class.

Figure 3
(A) Results for Ln NT-proBNP before, 1, 6, and 12 months after clip implantation. (B) Results for 6MWT distance (meters) before, 1, 6, and 12 months after clip implantation.
6MWT = 6-minute walk test; NT-proBNP = N-terminal pro-B type natriuretic peptide.

Figure 4
Kaplan-Meier curves at 1-year follow-up. (A) Freedom from all-cause death. (B) Freedom from all-cause death or re-admission for heart failure.

Table 3
Effects of variables associated with all-cause mortality tested by multiple logistic regressions
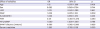
6MWT = 6-minute walk test; CI = confidence interval; EuroSCORE II = European System for Cardiac Operative Risk Evaluation II; FMR = functional mitral regurgitation; LVEF = left ventricular ejection fraction; NT-proBNP = N-terminal pro-B type natriuretic peptide; OR = odds ratio; PASP = pulmonary artery systolic pressure.
DISCUSSION
The present study has demonstrated the efficacy and safety of trans-catheter mitral valve repair with MitraClip to treat patients with severe MR in both octogenarians and younger patients who carry high surgical risks.
Advanced age is a traditional risk factor for peri-operative morbidities or mortality in open-heart surgery.16)17) In Euro Heart Survey, every 10-years increase of age carries nearly 70% incremental risk for 1-year mortality in subjects who underwent surgical mitral valve intervention.4) In the same survey, impaired LVEF, older age, and comorbidity were the most striking characteristics of patients who denied surgery. From systemic review, even surgical correction is the standard treatment for subjects with severe MR, surgical correction of MR in octogenarians is associated with high perioperative mortality and poor long-term survival with an uncertain benefit on quality of life.18)
As compare to surgical mitral valve intervention, trans-catheter mitral valve repair with MitraClip device appears remarkably safe in the elderly population in terms of acute mortality and complications.19) From Getting Reduction of Mitral Insufficiency by Percutaneous Clip Implantation (GRASP) registry, MitraClip was shown to be safe and effective in most patients, with similar hospital length of stay, 1-year clinical outcomes and re-hospitalization rates in either elderly or younger patients.20) As comparing to previous studies, our cohort demonstrated that octogenarians after the procedure could benefit from increase of distances in 6MWT. This functional regain sustained for 1-year follow-up. This information is important especially in the elderly subjects. In patients with severe MR, effort dyspnea or exercise intolerance significantly limited physical activity and clinical frailty was adversely affects quality of life.21) In fact, Metze et al.22) found frailty or pre-frailty was diagnosed in 94% of patients who underwent trans-catheter mitral valve repair. Interestingly, we found the distance of pre-procedure 6MWT can predict the all-cause mortality at 1 year. This finding may correspond to previous study, which showed frail patients still benefit from trans-catheter mitral valve repair in spite of higher mortality compared with non-frail patients.22) In the transcatheter mitral valve interventions (TRAMI) registry, pre-procedural 6MWT distance <200 meters showed a strong trend towards increased 1-year mortality in patients underwent MitraClip procedure.23)
Given the Asian patients are reluctant to undergo open-heart surgery and the observed mortality is higher than the surgical risk prediction model,24)25) there is an unmet need to ameliorate the disease awareness and the therapeutic adherence in Asians. Even though more than half of the subjects who underwent MitraClip procedure at age over 75 in western registries, Asians paid more attention about peri-operative complications and long-term efficacy especially after age of 80. In our study, the 1-year overall survival rate is 86%,26) which is very similar to western data, 80% in the TRAMI registry from Germany, 84% in GRASP registry from Italy,27) 83% in ACCESS-EU registry in the Europe.28) In TRAMI registry, they found the predictors of 1-year mortality were NYHA class IV, anemia, previous aortic valve intervention, poor renal function, peripheral artery disease, LVEF <30%, severe tricuspid regurgitation and procedural failure but not age per se. Every 5-years increasing age above 60, the surgical risk upgrade in the EuroSCORE II for open-heart surgery. Using GRASP registry, Buccheri et al.27) developed a risk model for prediction of 1-year mortality in patients undergoing MitraClip implantation. By calculate the data of natural log pro-B type natriuretic peptide level, NYHA Fc IV, mean arterial blood pressure, and hemoglobin, the GRASP nomogram had superior discriminative ability than traditional surgical risk prediction model with EuroSCORE II and STS-PROM score.27) The negative impact of advanced age on surgical risk is not observed in trans-catheter mitral valve repair. However, there are still uncertainties of procedure long-term efficacy when we try to treat extreme elderly patients with trans-catheter approach. Nonagenarians showed an increased peri-procedural mortality and higher mortality in follow-up compared to octogenarians who underwent trans-catheter aortic valve intervention.29) Nowadays, there is no data investigating safety and efficacy of trans-catheter mitral valve intervention in nonagenarians. In our cohort, 2 nonagenarians with DMR received MitraClip procedures. One subject suffered from acute rupture of abdominal aortic aneurysm and led to mortality at 6 months after index procedure. Another patient suffered from re-hospitalization due to HF at 1 month after index hospitalization. This finding indicates age alone is not a predictive factor but apply for treatment should be carefully evaluated by the heart team on an individual basis.
Our study has the inherent limitations of its observational design, single center experience, and the data were collected retrospectively. Even the preliminary data may have encouraged the clinical application of MitraClip, the case number is still limited. In our cohort, the left ventricular function in elderly patients was better than younger patients. This could counterbalance the negative impact of age in survival probability. The long-term impacts of MitraClip on hemodynamics, clinical outcomes and functional recovery after 1 year should be further evaluated. Parallel surgical or medical control groups are lacking. According to the guideline, we believe MitraClip should be reserved for patients with high or prohibitive surgical risks.
In conclusion, trans-catheter edge-to-edge mitral valve repairs are safe and have positive clinical impact in Asians with severe MR, even in advanced age. For those with eligible vavular anatomy, octogenarians can also benefit from MitraClips in respect of HF symptoms and functional capacities improvement up to 1-year follow-up. This preliminary experience demonstrates that advanced age per se should not be the only reason for deferring trans-catheter mitral valve repair.
 XML Download
XML Download