

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Worldwide acute malnutrition or wasting (low weight-for-height) affects 50 million children aged under five years [1]. These children are vulnerable to short-term risks of disease, impaired development and mortality, and irreversible long-term risks such as short stature and impaired cognition. Undernutrition is estimated to be associated with 45% of the deaths among children under five every year, occurring mostly in low- and middle-income countries [2]. Identification of acutely malnourished children is thus a priority for timely treatment and ultimately to avoid child illness and death.
To measure non-oedematous acute malnutrition in children aged 6–59 months, the World Health Organisation (WHO) guidelines endorse the use of Mid-Upper Arm Circumference (MUAC) or Weight-for-Height Z-score (WHZ), using these to classify Severe Acute Malnutrition (SAM) (WHZ < −3, MUAC < 11.5 cm), Moderate Acute Malnutrition (MAM) (WHZ −3 to < −2, MUAC 11.5 to < 12.5 cm) and Global Acute Malnutrition (GAM) (WHZ < −2, MUAC < 12.5 cm) [34].
So far, the WHZ indicator has become the accepted ‘gold-standard’ anthropometric indicator for acute malnutrition. WHZ is an index of weight and height based on the WHO 2006 Child Growth Standards [5]. It is used for diagnosis, but also to compute prevalence estimates and global indicators. Yet, to obtain the WHZ, a measurement of height and weight by trained personnel using a board and scale is required. The results obtained can then be plotted using a growth chat.
In low-income, high-prevalence or emergency settings where resources may be limited, MUAC becomes an essential tool, as it is a quick, easy and cheap method to identify acutely malnourished children using only a non-stretch tape around the mid-upper arm. MUAC is primarily used to produce rapid prevalence estimates [67], and for community screening via Community-based Management of Acute Malnutrition (CMAM) [8]. However, in spite of MUAC's higher functionally as an alternative in areas of scare resources, its diagnostic value continues to be debated.
Since the use of the 2006 WHO Growth Standards [5], the SAM MUAC cut-off was increased from 11.0 to 11.5 cm [39]. Three subsequent studies investigating MUAC performance, suggest revised cut-offs for SAM (ranging from 11.8 to 13.7 cm) [101112] with one recommending age- and sex-specific MUAC cut-offs [10]. Three other performance studies concluded that MUAC should not be used alone as it fails to accurately identify acutely malnourished children according to WHZ [131415].
Studies also predominantly found that the children identified with GAM or SAM using MUAC versus WHZ were not the same groups. This aligns with existing knowledge, as highlighted in the WHO Guidelines [3]. Children identified with MUAC tend to be female, younger and shorter for their age [31617]. While this may be favourable for screening higher-risk children, it questions the value of MUAC to diagnose the individual child with acute malnutrition.
A recent work by Grellety et al. [18] showed large discrepancies when using MUAC and WHZ to identify GAM and SAM and the differences seen across countries. The authors highlighted the relevance of within country and regional variations of the indicators, and advised that both indicators should be used as independent admission criteria. Therefore, the inconsistent conclusions regarding the diagnostic value of current MUAC cut-offs to diagnose acute malnutrition along with the discrepancy seen across countries warrants continued investigation.
The present study was set in Niger, where the mortality rate of children under five is trending downward (326 deaths/1000 live births in 1990 to 114 in 2012), but still ranks among the highest in the world [19]. While there have been improvements in malnutrition prevalence, levels still remain high (children under five stunted 43.9% or wasted 18%) [20]. Recognising the priority for acute malnutrition identification, two recent studies conducted in Niger showed that mothers can reliably use MUAC to diagnose their children as acutely malnourished [2122]. With evidence for community monitoring using MUAC in Niger and the variability observed when using MUAC across countries, this study aimed at assessing the performance of MUAC as an indicator of GAM and SAM using WHZ as the gold-standard for the diagnosis of acute malnutrition among children aged 6–24 months in rural Niger.
SUBJECTS AND METHODS
Study Design
This study used cross-sectional, secondary data from a community-based sample of children aged 6 to < 24 months living in rural Madarounfa, Niger. The data was collected during August 2011 until October 2012. The current study used baseline data from Prudhon et al. [23] that originated from a larger study by Langendorf et al. [24]. The primary studies were conducted by Epicentre in partnership with national non-government organisation, Niger Health Forum (FORSANI). Full methodological details are published elsewhere [2324]. The STROBE checklist [25] was used for the reporting of this cross-sectional study (Supplementary Table 1).
Study Setting
This study was set in Madarounfa, a rural district of the Maradi region of Niger. During the study period 2011 to 2012, the Maradi region was affected by drought and at risk of severe food insecurity [26]. Niger is a low-income country, ranks the lowest on the Human Development Index (Index 0.354, Rank, 189) [27], and it is prone to political instability, chronic food insecurity and natural crises.
Study Sample
Participants of this study were children aged 6 to < 24 months with complete anthropometric data (weight, height, MUAC), and without clinical signs of oedema, as this can increase body weight and compromise the reliability of WHZ and MUAC. The participants were enrolled in the primary study based on eligibility criteria: height > 60 and ≤ 80 cm, nil known food allergies or difficulties swallowing, and primarily residing in one of the 17 selected study villages within the Madarounfa district.
Data Collection
All houses in the selected villages were visited and eligible children, after informed consent was given, had anthropometrics measured (height/length, weight, MUAC) by trained nutrition assistants according to standardised protocol and using calibrated equipment. Sex of the child, date-of-inclusion and birth-date were recorded using a questionnaire completed by the primary caregiver. If date-of-birth was unknown, a local calendar of events was used to assist the primary caregiver to recall the birth and estimate the child's age, as recommended by WHO [3].
Data management
Children with missing information for key variables: MUAC, height, weight or age were excluded from the analysis (Fig. 1). WHO Anthro software (version 3.2.2, January 2011) with macro for SPSS was used to calculate z-scores for anthropometric indices (Height-for-Age Z-score: HAZ, and WHZ). Any children with extreme values for z-scores according to commonly applied WHO flag recommendations [28] were excluded from analysis (Fig. 1). Both MUAC and WHZ indicators were dichotomised according to the WHO guidelines for GAM (WHZ < −2 and MUAC < 12.5 cm) and also for SAM (WHZ < −3 and MUAC < 11.5 cm).
Where age was obtained using a local events calendar, it was recorded to the nearest day. Where date-of-birth was known, date-of-inclusion was subtracted from date-of-birth and age was calculated in days. The age variable was dichotomized according to children aged 6–11.9 months and 12–23.9 months. This is of practical relevance as children aged 6–12 months have greater growth velocity and comparatively plateau at 12–24 months [29]. Secondly, feeding guidelines change between these age groups; while continued breastfeeding is recommended for both age groups, children 12–24 months require greater quantities and more complementary foods [30]. Stunting status was dichotomised as HAZ < −2 stunted or HAZ > −2 not stunted, as per WHO growth standards [5].
Statistical analysis
SPSS software Version 23 (SPSS Statistics for Windows, Armonk, NY: IBM Corp) was used for analysis. Means and standard deviations (SD) were calculated for normally-distributed height, weight and MUAC variables. Frequencies of categorized standard WHO growth indicators were calculated (WHZ, HAZ and MUAC). These variables were stratified by age and sex for descriptive purposes.
Contingency tables for GAM and SAM identification with current MUAC and WHZ cut-offs were used to calculate sensitivity (Se), specificity (Sp), Positive Predictive Values (PPV) and Negative Predictive Values (NPV). These calculations were repeated when stratified by dichotomous variables: sex, age group and stunting status, factors known to differ with MUAC classification [16].
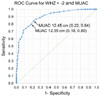
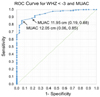
An empirical Receiver Operating Characteristic (ROC) analysis and Area Under the Curve (AUC) index was used to assess performance of MUAC as a diagnostic test when using WHZ as the criterion for acute malnutrition. The ROC analysis plots the Se and 1-Sp of the diagnostic test (MUAC) at intervals of cut-off points, against the diagnostic criteria WHZ. The analysis was run for diagnosis of GAM (WHZ < −2) and then SAM (WHZ < −3).
The AUC obtained from ROC analysis, ranges between 0 and 1, where 0.5 signifies a worthless test (50% accuracy), and 1 signifies a perfect test (100% accuracy). The upper and lower 95% Confidence Intervals (CI) of AUC are also presented. Overlapping CIs for AUC were considered indicative of a lack of significant difference between stratified groups. The ROC analysis was repeated, stratified by age group, sex and stunting status.
Using the ROC analysis coordinates, the Youden Index [31] was calculated according to the formula (Se + Sp) − 1. Resultant values range between 0 and 1, with 0 indicating no differential ability, and 1 indicating complete differential ability, giving equal weight to Se and Sp [32]. From inspection of the ROC graph and the Youden Index, the optimal cut-off points providing maximum Se and Sp were identified for GAM and SAM diagnosed by WHZ. If the optimal MUAC cut-off point differed from the current guidelines, MUAC was dichotomised using the new cut-off point and the Se, Sp, PPVs and NPVs were calculated using this value. Prevalence estimates of GAM and SAM using current guidelines for MUAC and WHZ, and new MUAC cut-offs found through the ROC analysis are presented.
Ethics approval
For this secondary analysis, a Material Transfer Agreement was signed 13 June 2016 between Epicentre and Karolinska Institutet. Data was de-identified (no individual, cluster or village location could be identified). The primary study protocol received approval from National Ethical Committee of Niger (013/2011/CCNE), Ministry of Public Health and the Comité de Protection des Personnes, Ile de France XI, France (11058) and was registered at ClinicalTrials.gov (NCT01828814).
RESULTS
Sample characteristics
A sample of 1161 children aged 6 to < 24 months were included in the analysis. The median age of the children was 12.4 (inter-quartile range 7.6, 18.2) months, with 48% aged 6 to < 12 months and 46% female. The mean height, weight and MUAC of the children in addition to categorised anthropometric indicators (WHZ, HAZ, and MUAC) categorised by current WHO classifications are presented in Table 1. Over half of the children were stunted (HAZ < −3 28.6%, HAZ −3 to < −2 34.3%) and almost one quarter had low weight for their height (WHZ < −3 4.4%, WHZ 3 to < −2 18.9%).
Diagnostic performance of MUAC
A preliminary bivariate Pearson correlation of WHZ and MUAC variables showed a strong positive linear relationship (R = 0.759, P < 0.001). The predictive values and empirical ROC analysis indicators for MUAC as a diagnostic test for GAM (WHZ < −2) and SAM (WHZ < −3) stratified by sex, age and stunting status, are presented in Tables 2 and 3. All AUC values were > 0.88, and all 95% CIs within stratified groups overlapped, indicating no significant differences within stratified groups.
When MUAC < 12.5 cm was used to identify GAM (Table 2), the Se and Sp of MUAC < 12.5 cm ranged from 0.66 to 0.87. For the total sample, Se was 0.79 (i.e. 79% true positive cases identified with both MUAC < 12.5 and WHZ < −2), Sp was 0.84 (i.e. 84% true negative cases, MUAC > 12.5 and WHZ > −2), Youden Index 0.63 and AUC was 0.89. The overlapping AUC CIs indicate no significant differences seen within each of the stratified categories. Among those who had a positive GAM screening test (MUAC < 12.5 cm), the probability of GAM according to WHZ < −2 criterion was 60% (PPV 0.60), whereas for a negative GAM screening test (MUAC > 12.5 cm), the probability of not having GAM according to WHZ < −2 criterion was higher (NPV 0.93).
When MUAC < 11.5 cm was used to identify SAM (Table 3), Se was lower than for GAM (57% true positive cases, i.e. identified with both MUAC < 11.5 cm and WHZ < −3) and Sp was higher; 97% children without SAM were accurately identified (i.e. 97% true negative cases, MUAC > 11.5 and WHZ > −3). AUC showed greater strength (0.94), yet Youden Index was lower (0.54). Again, within each of the stratified categories there were no statistically significant differences. The most pronounced difference was seen for stunting status; MUAC was less sensitive but more specific among children with normal height for age when compared to stunted children. Compared with GAM, PPV for SAM was lower and NPV was higher (0.44 and 0.98 respectively).
Receiver operating characteristic curves
Upon inspection of the ROC curve (Fig. 2) and Youden Index calculations, the MUAC cut-off point maximising Se and Sp to identify GAM was approximately 12.5 cm (Se 0.79, Sp 0.84, Youden Index 0.63). Upon inspection of the ROC curve (Fig. 3) and Youden Index, the MUAC cut-off point maximising Se and Sp was approximately MUAC 12.0 cm (Se 0.84, Sp 0.87, Youden Index 0.71).
Acute malnutrition prevalence estimates
MUAC overestimated prevalence of GAM (MUAC 31.1%, versus WHZ 23.3%) and SAM (MUAC 5.7% versus WHZ 4.4%) (Fig. 4). If both indicators were applied, fewer children were identified with GAM (18.5%) and with SAM (3.3%). When using MUAC < 12.0 cm, identified from the ROC analysis, there were greater true positives (3.7% SAM identified with both WHZ and MUAC) and fewer cases were missed (0.7% identified with WHZ only), however the SAM prevalence was largely overestimated (16.8%) (Fig. 4).
DISCUSSION
This study assessed the diagnostic performance of current MUAC cut-offs to identify acute malnutrition diagnosed using the gold-standard WHZ in a large community sample of children aged 6–24 months from rural Niger. Se and Sp of MUAC was optimised using the current cut-off for GAM, and a higher cut-off for SAM. Based on our findings, we recommend community screening using the current MUAC cut-off < 12.5 cm for GAM, but using MUAC < 12.0 cm for SAM. Children identified at risk of SAM using MUAC < 12.0 cm should be referred to health care services and, as currently recommended, receive treatment based on MUAC < 11.5 cm and WHZ < −3 to achieve increased identification and accuracy, vital for timely management of SAM.
Within this sample, the current MUAC cut-off for SAM failed to capture 40% of severely malnourished children. Using the increased cut-off < 12.0 cm identified in this study, this figure decreased to 16% (Se 84%, true-positive identification increased from n = 29 to 43). Acknowledging the potential and valid criticism of placing equal importance on Se and Sp, this objective method applied in this context achieved higher Se. This is arguably preferred, as more high-risk severely malnourished children would be appropriately referred to Outpatient Therapeutic Programmes (OTP) to receive treatment.
According to our results, using MUAC < 12.0 cm as a sole referral criterion would more than triple the number of children directed to OTP, and only one third of these would be true-positive SAM cases. Even with the increasing cost-effectiveness of CMAM [33], this is not ideal in a resource- and financially-constrained environment. It would also place undue stress on children and families when SAM is not present (false-positive cases). To mitigate these issues, the authors support the two-step community screening process, first using MUAC < 12.0 cm for SAM, followed by weight and height measurements to make diagnoses using the WHZ indicator (illustrated in Fig. 5). Depending on local feasibility, WHZ assessment may take place at the location of community screening or at the local health service.
Other studies investigating the validity of current MUAC cut-offs to diagnose acute malnutrition also found low Se using the current MUAC cut-offs [101112131415] and those assessing SAM highlighted the need to revise the MUAC < 11.5 cm cut-off [11121315]. Laillou et al. [11] suggest increasing the MUAC above the current cut-off to < 13.3 cm at screening and then using current MUAC and WHZ for SAM diagnosis, as per the procedure proposed in this study. Our study suggests a middle ground and we assume that the additional time, staff and equipment requirements of obtaining WHZ can be justified when the alternatives are either increasing OTP referrals by 300% using MUAC < 12.0 cm, or continuing to miss 40% of children with SAM using the current MUAC cut-off.
In contrast to the findings of this study, two validity studies both obtained lower Se values and concluded MUAC < 12.5 cm should not be used as a stand-alone criterion for GAM [1014]. Our diagnostic performance measures did not show significant differences when stratified by sex, age or stunting status. This may be partly explained by the younger age group and the high prevalence of stunting in our study sample. Differences in age are most apparent for 6–23 months compared with 24–59 months [3], and WHZ can be influenced by body shape and can affect prevalence of acute malnutrition in some populations [34].
It is accepted and highlighted in the WHO guidelines [3] that MUAC and WHZ indicators identify different groups of acutely malnourished children. These differences are more apparent for SAM, as seen in our results. If two-step screening using MUAC and then WHZ was implemented according to the current guidelines, approximately 40% of the children with SAM would be missed (prevalence using both indicators: 2.5%, WHZ only: 4.4%). This poor overlap of indicators for SAM provides support for our proposed change to MUAC of < 12.0 cm screening. In addition to the low cost and ease of using MUAC as the principal screening tool, it may be a better predictor of mortality for SAM in younger age groups [335]. Therefore, after MUAC < 12.0 cm screening, children identified by MUAC < 11.5 cm or WHZ < −3 should receive treatment. The same method was suggested by Laillou et al. [11] and is currently practiced by WHO Integrated Management of Childhood Illness (IMCI) [36].
An additional consideration for implementation is the degree of measurement error when the proposed cut-offs differ by 0.5 cm. There are many knowledge gaps regarding the inter- and intra-rater reliability of both MUAC and WHZ [373839]. While potentially more difficult to measure, the 0.5 cm difference modifies only the proposed referral to step 2 of screening with WHZ, not the overall children identified as acutely malnourished. Two recent studies conducted in Niger demonstrated that mothers can reliably use MUAC to classify their children as acutely malnourished, and suggests MUAC done regularly by mothers should become the focal point for efforts to scale-up CMAM [2021]. There is no screening tool that surpasses MUAC in terms of ease and practicality and, with use among community members to achieve ongoing monitoring, the resultant earlier detection and treatment of children with acute malnutrition can ultimately reduce child mortality.
This study is of importance within the current food insecurity crisis and high acute and chronic malnutrition across areas of western Africa. These findings can assist in adapting acute malnutrition screening processes and increasing identification of high-risk children with SAM. Implementing changes to the screening process must be considered in context. The ability to cope with increased demand on staff, resources and finances must be assessed. In neighbouring countries Burkino Faso and Chad, MSF currently consider these factors, adjusting MUAC thresholds for treatment admission according to contextual factors, for example, ongoing mortality, presence of other nutrition service providers, access and resources [40]. It is highly relevant to consider this in the Sahel region, and other regions with ongoing high prevalence of chronic and acute malnutrition.
The results of these analyses suggest that the prevalence of acute malnutrition (i.e. GAM and SAM) is relatively similar when MUAC or WHZ are used with the existing cut-offs, but that a MUAC of < 12.0 cm could improve case identification when screening for SAM. Thus, current MUAC cut-offs should continue use when rapid estimates are required for efficiently assessing the nutrition needs of a location, particularly in emergency settings as recommended [67].
A strength of the present study is the methodological standards adhered to during anthropometric data collection, crucial for validity studies [41]. Measures were collected at one single time-point, were in accordance with globally-accepted, standardised protocol and undertaken by trained nutrition assistants using calibrated equipment. Given the critical importance of sound methodologies in validity studies, and the question of reliability of the indicators, it is recommended that future sutures assess and report on inter- and intra- observer reliability of the anthropometric measures.
This study made efforts to exclude children with clinical signs of oedema, which can influence weight and thus WHZ, leading to false-negative or false-positive results. The primary data did not include other potential factors evidenced to impact either indicator, such as body shape, injury or disability [143442] which could cause random or systematic classification errors.
In conclusion, this study contributes to the body of evidence regarding the performance of current MUAC cut-offs to identify acute malnutrition defined by WHZ and suggests that a higher MUAC cut-off (< 12.0 cm) could improve accurate case identification of SAM when undertaking community screening among children under five. Children with MUAC < 12.0 cm should then be referred to health services for diagnosis and subsequent treatment based on MUAC < 11.5 cm and WHZ < −3, as per current guidelines. Existing MUAC cut-offs for GAM and SAM should continue to be used for rapid prevalence estimates and resultant direction of humanitarian response, policy and nutritional programming.
The acute malnutrition and stunting prevalence in this sample of children aged 6–24 months living rurally in Niger were comparable to regional national estimates. Acknowledging that there are country variations in the different groups of acutely malnourished children that MUAC and WHZ indicators [18], and that MUAC and WHZ are impacted by factors such as body shape [9], the authors cannot claim global application but are confident that these results have good external validity, particularly within the Sahel region. These findings can assist in adapting acute malnutrition screening processes and increasing identification of high-risk children with SAM.
The use of MUAC as a fast, effective, low-cost screening tool is invaluable. When paired with the gold-standard WHZ, a greater number of severely malnourished children can be directed to treatment services. Early identification and intervention should be a priority for management of acute malnutrition in emergency settings and globally, ultimately reducing acute malnutrition related child morbidity and mortality.






 XML Download
XML Download