

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Pulmonary embolism accounts for 1% of all cancer deaths and is a common complication in cancer patients. The incidence of pulmonary embolism in cancer patients is 1 in 200, which is 100 times that observed in the general population.123 In previous studies, the mortality rate in patients with pulmonary embolism was 15% in hemodynamically stable cases compared to 58% in hemodynamically unstable cases, and venous thromboembolism (VTE) was associated with a poor prognosis in patients with cancer.45 Adequate management of VTE is therefore a key priority for clinicians involved in the care of cancer patients.
In 2003, the Clinical Leaders of Thrombosis (referred to CLOT) group reported that low-molecular-weight heparin (LMWH) was superior to warfarin in the treatment of VTE in cancer patients.6 Subsequently, various treatment guidelines have recommended LMWH, including dalteparin, as the standard treatment for VTE in the oncology population.789 Advantages of LMWH over warfarin include a lower number of drug interactions and the lack of any requirement for routine therapeutic monitoring. However, LMWH is administered via subcutaneous injection, which may be associated with physical and/or psychological discomfort as well as adverse events at the injection site, such as extensive bruising.10
The 2014 European Society of Cardiology (ESC) guidelines for the treatment of VTE recommend the administration of direct oral anticoagulants (DOACs) as standard therapy.11 DOACs confer their anticoagulant effect through the inhibition of single factors within the coagulation cascade, such as factor X or thrombin.12 In view of their highly targeted mechanism of action and ease of administration, DOACs are of increasing interest in terms of the treatment of VTE in cancer patients. A recently published study demonstrated that rivaroxaban and edoxaban for cancer-associated VTE was not inferior to LMWH in terms of recurrence and major bleeding but increased clinically relevant bleeding.1314 Additionally, available research data support the administration of rivaroxaban to patients with cancer-associated VTE.15161718 However, there was no definitive study of the stability and therapeutic efficacy of rivaroxaban in gastrointestinal and pancreatobiliary cancer patients. In addition, several studies report an increased rate of gastrointestinal bleeding in patients receiving DOACs for the prevention or treatment of VTE.1920212223 These data suggest that studies into the safety of rivaroxaban, including the risk of bleeding, are warranted in cancer patients, in particular those with gastrointestinal malignancy.
The aim of the present retrospective study was to compare the incidence of bleeding and other treatment outcomes in patients with gastrointestinal cancer who received either rivaroxaban or LMWH for the treatment of VTE.
METHODS
Study design and patients
The present single-center study was performed at the Asan Medical Center, which is a 2,700-bed tertiary hospital in Korea. Eligible patients were identified through anticoagulant prescribing information contained in the electronic medical record system. The study inclusion criteria were: 1) a diagnosis of stomach cancer, colorectal cancer, or pancreatobiliary cancer (subsequently termed GI tract cancer); 2) a confirmed pulmonary embolism and/or deep vein thrombosis; and 3) treatment of the VTE with rivaroxaban or LMWH between January 1, 2012, and December 31, 2016.
Rivaroxaban and LMWH administration
Because no standardized protocol for the anticoagulants selection of rivaroxaban versus LMWH was in use at the study center during the study period, treatment choice was made on a case-by-case basis and at the discretion of the responsible clinician.
Rivaroxaban was administered orally 15 mg twice daily with food for 21 days followed by 20 mg once daily. LMWH was administered subcutaneously: dalteparin 200 IU/kg once daily; enoxaparin 1 mg/kg twice daily; nadroparin 85.5 IU/kg body weight twice daily.
Study groups
The rivaroxaban group comprised GI tract cancer patients with pulmonary embolism or deep vein thrombosis who were prescribed rivaroxaban, irrespective of previous prescription. Patients who were subsequently switched to anticoagulant medications other than rivaroxaban were excluded from the analyses. Duration of rivaroxaban administration was defined as the duration over which rivaroxaban was administered as the sole VTE therapy.
The LMWH group comprised GI tract cancer patients with pulmonary embolism or deep vein thrombosis prescribed dalteparin, enoxaparin, or nadroparin, irrespective of previous VTE medication history. Patients who were subsequently switched to a different LMWH preparation were considered to have undergone maintained LMWH therapy. However, patients who were switched to other drug classes were excluded from the analyses. Duration of LWMH therapy was defined as the sum duration of the administration of dalteparin, enoxaparin, or nadroparin.
Diagnosis of pulmonary embolism and deep vein thrombosis
Pulmonary embolism was diagnosed via the evaluation of a computed tomography (CT) or ventilation-perfusion scan by a board-certified radiologist. Deep vein thrombosis was diagnosed via lower extremity Doppler ultrasonography or CT venography. Follow-up examinations were only performed in cases of suspected recurrence or in patients requiring periodic evaluation of disease status.
Demographic and clinical characteristics
For each patient, data on the following factors were retrieved from the electronic medical record system: age, gender, body weight, cancer type, Eastern Cooperative Oncology Group performance score (ECOG PS), metastatic status, history of chemotherapy, history of recent surgery, glomerular filtration rate, occurrence of pulmonary embolism, occurrence of deep vein thrombosis, and hospitalization status.
Inpatient status was assigned to patients who were hospitalized at the time of VTE diagnosis. Outpatient status was assigned to patients whose VTE was diagnosed in the outpatient department or emergency room.
Metastatic status was assigned to patients meeting the M1 metastasis criteria of the TNM staging system (i.e., metastasis to distant organs beyond regional lymph nodes) at the time of pulmonary embolism or deep vein thrombosis diagnosis. History of chemotherapy status was assigned in patients who had received at least one dose of chemotherapy prior to VTE diagnosis. ECOG PS was retrieved by electronic medical records.
Outcome measures
The primary outcomes were the incidence of major bleeding and clinically relevant bleeding. Major bleeding was defined as any bleeding event occurring during treatment with LMWH or rivaroxaban that: 1) was associated with death; 2) occurred at a fatal site (intracranial, intraocular, retroperitoneal, intraspinal, or pericardial); or 3) required a transfusion of at least 2 units of packed red blood cell, or led to a hemoglobin decrease of at least 2.0 g/dL.24 Clinically relevant bleeding was defined as any obvious bleeding occurring during treatment with LMWH or rivaroxaban and resulted in medical intervention, unscheduled visits with clinicians, discontinuance of anticoagulants, or a decline in the activities of daily life.25
The secondary outcomes were mortality and recurrence rates. Recurrence was defined as CT or ultrasonographic evidence of an increase in thrombosis or embolism or of a thrombosis or embolism at a new site, during treatment with LMWH or rivaroxaban. Symptomatic recurrence was defined as CT or ultrasonographic evidence of recurrence in patients presenting with symptomatic pulmonary embolism or deep venous thrombosis during treatment with LMWH or rivaroxaban.
Data on survival status were retrieved from electronic medical records at the Asan Medical Center or from Korean National Health Insurance Database. Survival data were collected up until December 31, 2017.
Statistical analysis
Inter-group comparisons were made for all baseline characteristics and outcomes. Categorical variables are expressed as the number and the proportion of subjects. Differences between the rivaroxaban and LMWH groups were analyzed using the χ2 test. Continuous variables are expressed as means and standard deviations. Differences in continuous variables were analyzed using the independent two-sample t-test.
Time dependent variables, such as time to bleeding and survival, were analyzed using the Cox proportional hazard model. Multivariate analysis was performed by Cox proportional hazard model with backward elimination (likelihood ratio [LR] test) to determine the effect of anticoagulants on clinically relevant bleeding and all-cause mortality. The multivariate analysis included variants showing inter-group differences in the univariate analyses (threshold was set at P < 0.1). Time-to-event curve were calculated by post-estimation Cox proportional hazards model curves. We also performed competing risk analysis by Fine and Gray model. In this analysis, we regarded clinically relevant bleeding as main outcome and all-cause mortality as competing events. We included covariates, which were valid in multivariate analysis for clinically relevant bleeding and all-cause mortality. The proportional hazards assumption was confirmed by examination of log (-log [survival]) curves and no relevant violations were found.
Statistical significance was set at P < 0.05. All statistical analyses were performed using SPSS version 21 (IBM Corporation, Armonk, NY, USA) analytical software.
Ethics statement
The study was approved by the Institutional Review Board (IRB) of the Asan Medical Center (IRB No. 2017-0652). IRB confirmed the requirement for informed consent was waived due to the retrospective nature of the analyses. All study procedures were conducted in accordance with the Declaration of Helsinki.
RESULTS
Between January 1, 2012, and December 31, 2016, a total of 375 GI tract cancer patients were diagnosed with pulmonary embolism or deep vein thrombosis. Of these, 94 patients were not eligible for study inclusion. The 94 non-eligible subjects comprised 81 patients who were prescribed warfarin, and 12 patients who received anticoagulants other than rivaroxaban, dalteparin, enoxaparin, nadroparin, and warfarin. One further patient discontinued medication for undocumented reasons. Therefore, the data of a total of 281 patients were included in the present analyses: rivaroxaban group (n = 78), LMWH group (n = 203) (Fig. 1). In LMWH group, 177 patients (87.2%) used dalteparin, 25 patients (12.3%) used enoxaparin and 1 patient (0.5%) used nadroparin.
Fig. 1
Patients flow diagram.
GI = gastrointestinal, VTE = venous thromboembolism, LMWH = low-molecular-weight heparin.

Table 1 shows the baseline characteristics of the two study groups. No significant inter-group difference was observed for age, gender, body weight, hospitalization status, or incidence of pulmonary embolism. However, a significant inter-group difference was found for age ≥ 65, cancer type, ECOG PS, metastasis, history of chemotherapy, recent surgery and glomerular filtration rate < 50. The rivaroxaban group included a higher proportion of patients with a good performance status with reference to ECOG PS and recent surgery than the LWMG group. The LMWH group included a higher proportion of patients with metastasis, a history of chemotherapy, and stomach cancer than the rivaroxaban group (Table 1).
Table 1
Baseline characteristics of the study cohort

Clinically relevant bleeding occurred in 19 patients (24.4%) in the rivaroxaban group and 31 patients (15.3%) in the LMWH group. Thus, the rivaroxaban group showed a higher incidence of clinically relevant bleeding without significance (P value = 0.074) (Table 2). In the rivaroxaban group, the following types of clinically relevant bleeding occurred: gastrointestinal tract, 12 patients (60.0%); urinary tract, 5 patients (25.0%); hemoptysis, 2 patients (10.0%); and skin, 1 patient (5.0%). In the LMWH group, the following types of clinically relevant bleeding occurred: gastrointestinal tract, 19 patients (61.3%); urinary tract, 1 patient (3.2%); intramuscular, 2 patients (6.5%); hemoptysis, 2 patients (6.5%); intraperitoneal, 3 patients (9.7%); pleural cavity, 1 patient (3.2%); and vaginal, 3 patients (9.7%) (Table 3). Major bleeding occurred in 4 patients (5.1%) in the rivaroxaban group and in 18 patients (8.9%) in the LMWH group.
Table 2
Univariate analysis of primary and secondary endpoints within 6 months

Table 3
Sites of bleeding by groups

During the anticoagulant therapeutic period, VTE recurrence occurred in 3 patients (3.8%) in the rivaroxaban group and 8 patients (3.9%) in the LMWH group. Symptomatic recurrence occurred in 0 patients in the rivaroxaban group and 1 patient in the LMWH group (0.5%). No significant inter-group difference was found for recurrence or symptomatic recurrence (Table 2).
After 6 months from anticoagulants start day, 167 patients had died. Of these, 29 (37.2%) deaths occurred in the rivaroxaban group. These included 1 death secondary to bleeding. In the LMWH group, 138 patients had died (68.0%). These included 4 deaths secondary to pulmonary embolism and 3 deaths secondary to bleeding. All-cause mortality was significantly higher in the LMWH group than in the rivaroxaban group (P < 0.001). However, no significant inter-group difference was found for mortality secondary to pulmonary embolism or bleeding (Table 2).
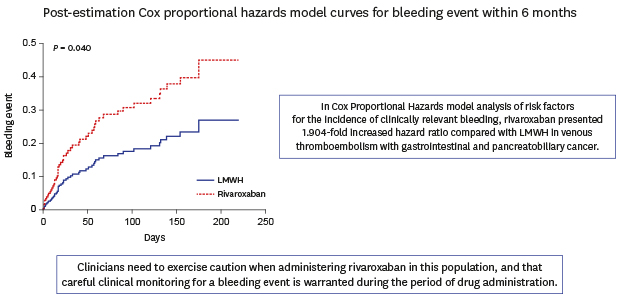
A Cox proportional hazards model was used to analyze the incidence and timing of bleeding during study drugs administration in the two study groups. The hazard ratio (HR) for bleeding within the therapeutic period was 1.904-fold (95% confidence interval [CI], 1.031–3.516; P = 0.040) higher in the rivaroxaban group (Fig. 2). In the multivariate analysis, poor performance status showed a trend towards association with bleeding risk. By contrast, no significant association with increased bleeding risk was found for cancer type, metastasis status, or history of chemotherapy (Table 4).
Fig. 2
Post-estimation Cox proportional hazards model curves for bleeding event within 6 months.
We compared incidence of clinically relevant bleeding between low-molecular-weight heparin and rivaroxaban. We drew the curves by post-estimation Cox proportional hazards model after adjustment for Eastern Cooperative Oncology Group Performance Status.
LMWH = low-molecular-weight heparin.
Table 4
Cox Proportional Hazards model analysis of risk factors for the incidence of clinically relevant bleeding

We analyzed the incidence of clinically relevant bleeding by Cox proportional hazard model. We selected meaningful variables by backward elimination (LR test). We initially included age ≥ 65, ECOG PS, cancer type, metastatic status, history of chemotherapy, recent surgery and anticoagulants. After backward elimination with LR test, we used anticoagulants and ECOG PS for multivariate analysis. In multivariate analysis, rivaroxaban presented 1.904-fold increased hazard ratio compared with LMWH.
HR = hazard ratio, CI = confidence interval, LMWH = low-molecular-weight heparin, ECOG PS = Eastern Cooperative Oncology Group performance status, CTx = chemotherapy, LR = likelihood ratio.
A Cox proportional hazards model was used to analyze all-cause mortality rate and survival time in the two study groups. Anticoagulant type did not impact all-cause mortality. A significant association with all-cause mortality was found for age, cancer type, metastasis status, and ECOG PS. In comparisons to patients with pancreatobiliary cancer, the hazard ratio for all-cause mortality was 0.705 in patients with stomach cancer (P = 0.014), and 0.278 (P < 0.001) in patients with colorectal cancer (Table 5).
Table 5
Cox Proportional Hazards model analysis of risk factors for all-cause mortality

We analyzed the incidence of all-cause mortality by Cox proportional hazard model. We selected meaningful variables by backward elimination (LR test). We initially included age ≥ 65, ECOG PS, cancer type, metastatic status, history of chemotherapy, recent surgery and anticoagulants. After backward elimination with LR test, anticoagulants were eliminated because it was not a valid variable for multivariate analysis.
HR = hazard ratio, CI = conference interval, LMWH = low-molecular-weight heparin, ECOG PS = Eastern Cooperative Oncology Group performance status, CTx = chemotherapy, LR = likelihood ratio.
We performed competing risk analysis by Fine and Gray model for clinically relevant bleeding and all-cause mortality. In univariate analysis, rivaroxaban presented 1.650-fold (95% CI, 0.942–2.880; P = 0.080) increased hazard ratio for clinically relevant bleeding. In multivariate analysis, rivaroxaban presents 2.418-fold (95% CI, 1.003–5.830; P = 0.049) increased hazard ratio for clinically relevant bleeding (Table 6).
Table 6
Competing risk analysis by Fine and Gray model for clinically relevant bleeding and all-cause mortality

We performed competing risk analysis by Fine and Gray model. In this analysis, we regarded clinically relevant bleeding as main outcome and all-cause mortality as competing events. We included anticoagulants, ECOG PS, cancer type, metastatic status, which were valid covariates in multivariate analysis of Table 4 and Table 5. In multivariate analysis, rivaroxaban presented 2.418-fold increased hazard ratio compared with LMWH.
HR = hazard ratio, CI = conference interval, LMWH = low-molecular-weight heparin, ECOG PS = Eastern Cooperative Oncology Group Performance Status.
DISCUSSION
To our knowledge, there is only limited data for investigating bleeding risk in GI tract cancer patients administered rivaroxaban, and the present study is performed to compare bleeding risk in GI tract cancer patients treated with rivaroxaban versus standard treatment for VTE in cancer patients, i.e., LMWH.26 Patients receiving rivaroxaban showed a 1.904-fold increased hazard ratio in clinically relevant bleeding tendency compared to patients treated with LMWH. However, no significant inter-group differences were found for major bleeding incidence and the secondary endpoints recurrence rate, symptomatic recurrence rate, and mortality. Several randomized control studies presented similar trends for DOACs use in cancer patients.1314 Recommendations for the use of DOACs in the treatment of VTE are based on findings that compared to warfarin, DOACs, including rivaroxaban, are associated with less bleeding and similar recurrence rates.2425 A previous meta-analysis showed that DOACs were not inferior to warfarin in terms of the treatment of VTE in cancer patients.27 Therefore, these results suggested that careful decision making to use DOACs in patients with GI tract cancer was warranted.
The present analyses demonstrated significant inter-group differences in several baseline clinical features, in particular age, ECOG PS, cancer type, metastasis status, history of chemotherapy, and recent surgery. The rivaroxaban group included a high proportion of patients with good ECOG PS and favorable metastasis status and a history of recent surgery, while the LWMH group included a high proportion of patients with a history of chemotherapy and metastases. This may reflect a tendency on the part of clinicians to adhere to standard drug administration guidelines in patients with more severe disease states.
In the present cohort, recurrence rate in both groups was about 4%, and no significant inter-group difference was found for symptomatic recurrence. The present recurrence rate was consistent with the 4%–15% recurrence rates reported in previous studies.616182728
Although the univariate analysis revealed a higher rate of clinically relevant bleeding without statistical significance in the rivaroxaban group, a multivariate analysis was performed to account for inter-group differences in baseline demographic and clinical characteristics. Factors with a reported association to bleeding during anticoagulant therapy in cancer patients include cancer type and history of chemotherapy.29 The LMWH group in particular included a high proportion of patients with metastases and a diagnosis of stomach cancer, well-established associations with bleeding.29 We also performed competing risk analysis for clinically relevant bleeding and death, because the LMWH group had more severe disease at baseline and also faced a higher mortality risk during follow-up. In the multivariate analysis and the competing risk analysis, rivaroxaban also presented increased HR for clinically relevant bleeding. Despite this, no significant inter-group difference was found for the incidence of major bleeding. However, the number of major bleeding events in the present cohort was very small, and future studies of larger cohorts are required to replicate these findings.
The most frequent site of bleeding in both study groups was the gastrointestinal tract. This is consistent with the findings of studies conducted by Chan et al.,19 which demonstrated an association between DOAC administration and increased gastrointestinal tract bleeding. Whereas the incidence of intracranial hemorrhage is lower in patients receiving DOACs than in patients receiving warfarin, research has shown that compared to warfarin, the DOACs rivaroxaban and dabigatran are associated with a higher rate of gastrointestinal bleeding.303132
Although the precise mechanisms were unknown, previous authors have hypothesized that DOACs cause bleeding in patients with gastrointestinal tract lesions.1933343536 Rivaroxaban is largely excreted through the kidneys (66%); however, 28% is excreted through the feces.36 A plausible hypothesis is that because rivaroxaban does not require transformation to an active form to exert its anticoagulant effects, its passage through the gastrointestinal tract may trigger bleeding.37 Chan et al.19 suggested that active rivaroxaban in the gastrointestinal tract could induce bleeding in existing lesions. By contrast, LMWH is mainly excreted via the kidneys, and thus the associated risk of gastrointestinal bleeding risk is relatively low.38 In our study, hematuria presented more common in the rivaroxaban group. When rivaroxaban was excreted in urine, unmetabolized rivaroxaban accounted for 36% of the total dose, otherwise LMWH showed 5%–10% anti-Xa activity of injected dose in the urine.39
Several studies provide evidence in support of the use of rivaroxaban for the treatment of VTE in cancer patients. These studies demonstrated that rivaroxaban was not inferior to LMWH in terms of recurrence, bleeding incidence, or mortality. However, patients with GI tract cancer accounted for only 25.4%–60% of patients in these studies.13151740 Therefore, these results cannot be generalized to the GI tract cancer population.
In the present cohort, all-cause mortality rates were higher in the LMWH group. However, the baseline characteristics of the two study groups differed, and the LMWH group would be expected to have higher mortality rates due to its higher proportion of poor prognosis cancer patients. After backward elimination with LR test, anticoagulants did not have association with all-cause mortality. This is consistent with previous findings from non-cancer patients.2425
The present study had several limitations. First, the retrospective study design may have resulted in build-in confounding, information bias and selection bias. Second, significant inter-group differences were found in terms of baseline characteristics. To address this, a multivariate analysis and competing risk analysis were performed. In addition, there was a concern that more deaths occurred in the LMWH, and this could lead to fewer opportunities for bleeding complications. For adjustment, we performed Fine and Gray model for competing risk analysis. Thirdly, a number of patients were lost to follow-up. However, this had no significant impact on the analysis of outcomes, because most patients were followed up until the time of death. Fourthly, because we found the bleeding events based on the electronic medical records, it can be underrecognized or miscategorized. Additionally, we obtained the data about baseline characteristics at the start day of anticoagulants therapy. There were possibilities that changes in time-varying confounding might not be captured. Finally, the present study focused on rivaroxaban, and thus the generalizability of the results to other DOACs, such as apixaban or dabigatran, is limited.
Despite these limitations, the present study present associations that rivaroxaban may increase the risk of bleeding in VTE patients with GI tract cancer. Despite having no impact on mortality or major bleeding, clinically relevant bleeding may impair quality of life and lead to an increased consumption of medical resources. The present data thus suggest that if DOACs are used for management of VTE in GI tract cancer patients, clinicians should be careful about bleeding events.
The present study generated valuable data concerning the safety and efficacy of rivaroxaban in the management of pulmonary embolism and deep vein thrombosis in patients with GI tract cancer. The results suggest that clinicians need to exercise caution when administering rivaroxaban in this population, and that careful clinical monitoring for a bleeding event is warranted during the period of drug administration. Because our study has several limitations, further study will be needed to confirm these issues.
 XML Download
XML Download