

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Severely comminuted acetabular fractures present a challenging scenario for the orthopaedic surgeon. Open reduction and internal fixation is a recommended treatment for many displaced acetabular fracture patterns; however, certain fracture patterns may not yield favorable short and long-term outcomes with osteosynthesis1). These patients are often left with persistent hip pain2345). Acute total hip arthroplasty (THA) is an alternative treatment option for these patients to allow for early mobilization, a primary objective for any orthopaedic procedure678).
Primary THA in acute acetabular fractures on the other hand, especially in association with pelvic discontinuity, transverse patterns with or without a posterior wall fracture, bi-columnar fractures, and T-type patterns pose an additional challenge due to difficulty in obtaining primary stability of the acetabular construct9). Although internal fixation may be combined with acute THA in these patients, immediate postoperative mobilization may be compromised, due to protected weight bearing for a period of time.
Poor clinical outcomes anticipated in some patients with the already recommended treatment methods led the authors to employ the revision THA principle of using a revision porous metal shell for acetabular fixation with adjunct stability provided by a cage known as ‘cup-cage construct’ technique in order to expedite postoperative mobilization allowing for full weight bearing. The early success on using a Trabecular Metal™ Revision Shell (TMRS) with Trabecular Metal™ Acetabular Revision System (TMARS) cage (all Zimmer®, Warsaw, IN, USA), in revision hip arthroplasty; led the authors to the expanded use of this reconstruction technique in the management of most challenging acetabular fractures. However, due to certain constraints including high costs and non-availability of the implant in low socioeconomic countries especially where patients are responsible for purchasing implants on their own and need to be imported for individual cases; we used Burch-Schneider cage (BS cage; initially brought by Sulzer Orthopedics Ltd., Winterthur, Switzerland; later by Zimmer Inc. and now with Zimmer Biomet Inc.) as a substitute for a TMARS cage. To the authors' knowledge, this is the first study of its kind discussing the use of a BS cage in a cup-cage construct for managing complex acetabular fractures. The purpose of this study was to evaluate the clinical and radiographic results of using a BS cage in conjunction with a porous hemispherical shell construct for the management of selected acetabular fracture patterns.
Go to : 
MATERIALS AND METHODS
Between 2010 and 2015, 24 patients were operated with this cup-cage construct technique, of which eight (33.3%) patients had an acetabular fracture indicated for an acute THA as per the criteria in our institution10). There were 7 male (87.5%) and one (12.5%) female patient. All patients were operated within three weeks of injury (range, 6–21 days).
All acetabular fractures were classified according to the Letournel and Judet classification11). In all the patients, the fracture pattern, bone defects and the presence of pelvic discontinuity were diagnosed based on radiological findings (X-rays and computed tomography scan) and confirmed intra-operatively (Fig. 1A–C, 3A). All those cases where host bone contact is inadequate, a pelvic discontinuity exists, and/or, the acetabular shell fixation is not primarily stable were considered for cup-cage construct. As the TMARS cage that specifically comes with TMARS was not available and had to be imported at an inflated cost, less expensive BS cage (Fig. 2) was used in all these patients.
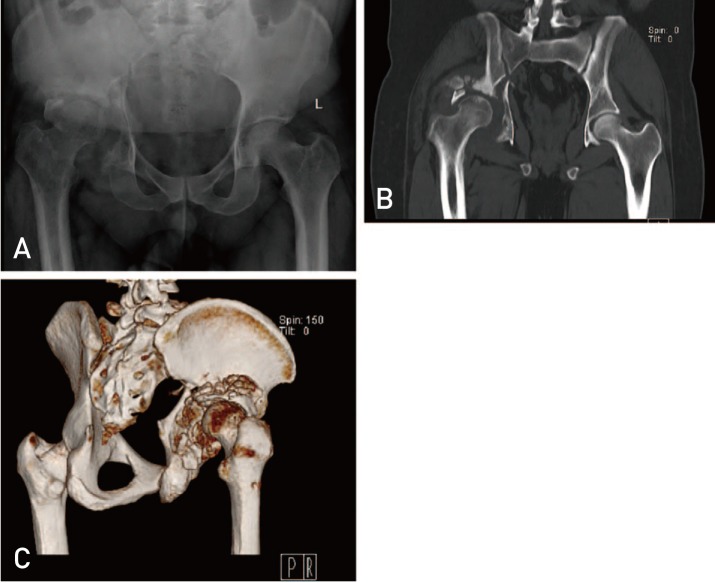 | Fig. 1(A) X-ray both hips with pelvis in anteroposterior view showing acetabular fracture in right side. (B) Computed tomogram scan of the pelvis in coronal section showing comminuted fracture of the acetabulum. Note the pelvic discontinuity. (C) Three-dimensional reconstruction computed tomogram showing the posterior aspect of the right hip. Note the comminuted fragments and near complete loss of bone in posterior column.
|
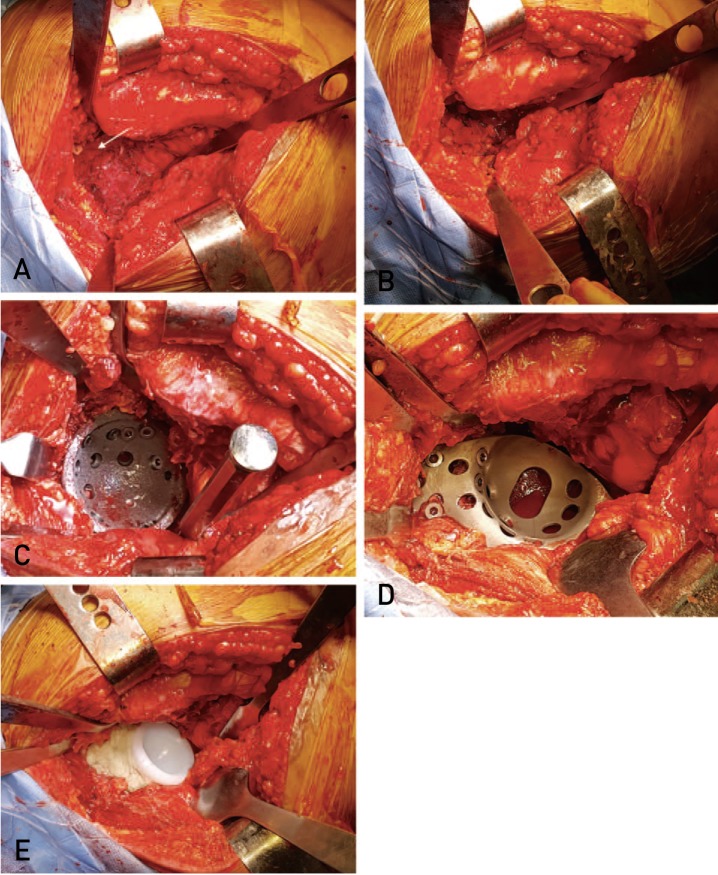 | Fig. 3(A) Exposure of the acetabulum. White arrow showing the only acetabular bone that was intact. Only soft tissue seen in the acetabular bed due to bone loss. (B) The acetabulum filled up with autografts from the resected femoral head. (C) Impaction of the trabecular metal shell and fixed with multiple screws. (D) Placement of the Burch-Schneider cage onto the acetabular shell and fixed with screws. The lower flange is into the osteotomy made in the ischium. (E) A polyethylene liner cemented onto the cage.
|

The mean age at the time of surgery was 61.5 years (range, 35–73 years). The period of hospitalization range from 6 to 14 days. One patient (No. 6) had an injury of the foot as well which was initially managed with conservative treatment. Later, she developed arthritis and required a triple arthrodesis two years following the hip reconstruction.
1. Surgical Technique
All the procedures were performed by the senior author (RM). Each case utilized a standard posterior approach. The decision to use a cup-cage construct was made intra-operatively following acetabular exposure. The femur was prepared first in all the cases. The femoral broaching was done with successive broaches of increasing sizes and the last broach that was securely fit in the canal was left in situ. The femur with the last broach in situ was retracted anteriorly with the help of a curved retractor to ease the acetabular exposure. The acetabulum was fully exposed by dividing the reflected head of rectus femoris and the gluteus minimus muscle. The acetabulum was then assessed for the fracture pattern, the extent of bone loss and presence of pelvic discontinuity (Fig. 3A). The findings were noted and corroborated with the pre-operative radiological findings. Patients with severe acetabular deficiency defined by discontinuity and/or bone loss >50% and would have compromised stability with the use of a cementless shell alone were considered for a cup-cage construct.
A Hohmann retractor was placed in the obturator foramen to demine the inferior extent of the true acetabulum. The acetabulum was prepared by progressively larger reamers until the appearance of bleeding bone. The acetabular floor was autografted from removed from the resected femoral head (Fig. 3B). The TMRS of an appropriate size (i.e., the size of last reamer) was impacted into the prepared acetabulum and then held in place by multiple screws (Fig 3C).
Adjunct screw fixation in the pubis or ischium can be used to secure the acetabular shell by drilling additional holes with a metal cutting burr and/or straight drill through the trabecular metal shell near its rim. The ring of the TM shell was removed in most cases where peripheral screw placement was required. The shell was intentionally positioned in a vertical and retroverted position to maximize the contact with host bone and permit the seating of a BS cage on top of the shell. The cup was then assessed for its stability with a Kocher clamp.
The BS cage of appropriate size was chosen to secure the TM shell in place. The ischium was exposed and a slot was prepared by an osteotome for placement of the inferior flange of the cage. The ilium in the posterosuperior part of the acetabulum was also exposed for placement of the superior flange of the cage. The inferior flange of the cage was appropriately molded and seated onto the cup with the molded flange into the slot in ischium, and cage secured with screws into the ilium through the superior flange (Fig. 3D).
The authors' own experience led to an observation that a size difference of 16 between the cup and the BS cage was appropriate for perfect seating of the cage onto the cup i.e. when a TMRS of size 66 was used, the BS cage size of 50 best fitted onto it. Accordingly, cups size 66 and size 60 were implanted in 4 patients each with corresponding BS cage size 50 and 44, respectively. Whenever possible (four cases), we used longevity liner of Trilogy cup from the same manufacturer (Zimmer®) that provides an option for 36-mm head (internal diameter) with an external diameter starting from 50 mm. Femoral head size 28-mm head was used in three cases, and 32-mm in one case.
The liner was selected and cemented in position over the cup-cage construct with pressure directed at 45° abduction and 20° anteversion for maximum stability of the joint (Fig. 3E). A trial reduction was done using the appropriate size head over the femoral broach followed by the definitive femoral stem and head implantation after ensuring the joint stability. All the patients were mobilized from the first post-operative day and advised for regular follow up.
An ambispective study was conducted. All the patients who had completed a year follow up were called up to attend our out patient department after the approval of institutional review board was obtained. The patients' medical details were obtained from medical records. They were then prospectively followed for a minimum of one-year then after, hence giving us a minimum follow up of 2 years. Clinical evaluation was done using the Harris Hip Score (HHS)12). In addition, data regarding the use of walking aids by the patient were also recorded. The serial radiographs including anteroposterior view of the pelvis and lateral view of the operated hip taken in immediate postoperative period (post-operative day 2) and then at six weeks, six months and once in a year thereafter as per our service protocol were evaluated for healing of fracture and, loosening or migration (if any). The immediate postoperative X-ray was taken as a baseline with which all the follow-up radiographs were compared. The acetabular bone bed medial to the cup was looked for its continuity without a break to label it as radiological healing.
Go to :
RESULTS
The mean follow-up was 50.5 months (range, 24–72 months). The HHS at the latest follow up was 88 (range, 78–92). The score was excellent in 3 (37.5%), good in 4 (50.0%) and fair in one (12.5%) patient. All except two patients were walking without a cane at the latest follow up. One patient (No. 1) was walking a painful limp. He had trochanteric bursitis and was treated with local steroid injection. Overall, there was 87.5% good to excellent clinical outcome with immediate weight bearing, and good walking ability without functional restriction in carrying activities of daily living. The patient demographics, clinical profile, treatment details and follow up of the patients in the study group are summarized in Table 1.
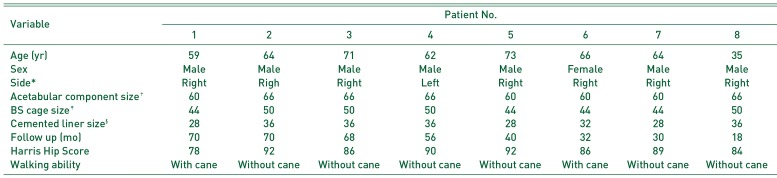
Table 1
Patient Demographics, Implant Details, Follow-up Duration and Clinical Profile of the Patients Operated with Cup-Cage Technique
![]()
In all the 8 hips, there were no changes in the radiological position of the acetabular component or the cage at the latest follow up. There were no signs indicative of loosening at the latest follow-up as assessed from the serial follow up radiographs. All the cases that had developed continuity of the bone graft medial to the acetabular shell with a varying extent of remodeling showing healing with bridging bone formation (Fig. 4). One patient had developed asymptomatic heterotopic ossification of Grade II as per Brooker's classification13).
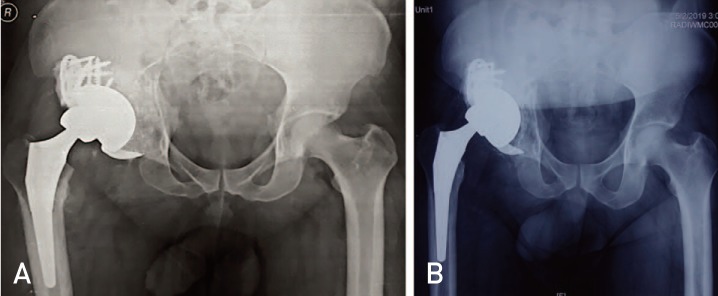 | Fig. 44. (A) Immediate post-operative X-ray of the same patient (in Fig. 1 and 3) showing reconstructed right hip with cup-cage construct technique. (B) Four-year follow up X-ray of the same patient showing the cup-cage components in situ. The fracture has healed and the component position is unchanged as compared to the immediate post-operative X-ray.
|
One patient (No. 1) had dislocation two months following the surgery, which was treated by closed reduction and hip abduction brace for 6 weeks. One patient developed infection (No. 7) at 3 weeks necessitating debridement and antibiotics for 6 weeks. The same patient had sciatic nerve palsy that had recovered after 4 months. The patient was doing very well at the latest follow up with a HHS of 88.
Go to :
DISCUSSION
The management options for complex acetabular fractures are limited and the measures that have been in practice since the past have poor results especially in elderly patients141516). The paradigm shift from conservative management with in bed traction to osteosynthesis, both have consequences of medical problems as well as psychological impacts on the patients due to immobilization17). Moreover, the patients with unfavorable outcome even after surgical fixation become the candidates for THA in the future. Hence, in selected patients with the anticipated unfavorable outcome from osteosynthesis, acute THA has recently been in practice7818). However, stability remains a major concern in cases with inadequate contact of non-fragmented host bone with the acetabular shell. Antiprotrusio cages that span from ilium to ischium bridge the pelvic discontinuity and/or address the major acetabular bone defect. These cages provide immediate mechanical stability by transferring the load across the fractures; however, most of these cages are non-biological as they are non-porous, no bone ingrowth occurs into them and hence they eventually fail1920). The authors already have a vast experience of using cages with hydroxyapatite coating and potential for biological ingrowth to manage acetabular fractures with severe bone loss in elderly10). With the advent of a newer technique of using a porous shell spanned by an anti-protrusio cage into which a polyethylene liner is cemented-so-called ‘cup-cage construct’ in revision hip arthroplasty, the same technique has been employed in complex acetabular fractures as well21222324252627). The philosophy behind this construct is that in cases where host bone contact is inadequate, a pelvic discontinuity exists, and/or, the acetabular shell fixation is not stable, the cage placed on top of the porous shell provides initial primary stability and protects the shell till biological fixation takes place. The bony ingrowth into the acetabular component occurs even with limited contact with the bleeding bone that often accompanies the pelvic discontinuity2829). Hence, the unitization of the cup with cage gives the entire construct adequate stability and long-term durability.
There are limited studies of using cup-cage construct technique for reconstruction in complex acetabular fractures. Chana-Rodríguez et al.30) used this technique in 6 patients with acetabular fractures, and, had 83% of good to excellent results at a minimum follow up of 2 years in patients with an average age of 77 years. There was no evidence of mechanical failure, in any of the cases. Solomon et al.31) performed a radiostereometric analysis of cup-cage constructs in 10 of their 12 patients with acetabular fracture and found that only 3 patients had migration above their suggested limits for primary THA defined by the author themselves. However, none of the patients including those above the threshold of migration were symptomatic at the follow up of one year. The patient demographics and clinicoradiological outcome of both studies are compared with the current study in Table 2. All our patients were physiologically elderly with chronological age above 59 years except one with 35-year age who had to undergo cup-cage construct due to severe comminution not amenable for fixation. The clinicoradiological results in our study are comparable to the other two studies. However, the other studies had used the TMARS system for fixation unlike ours. The cage provided in this system has the advantage of modularity, flexibility, and design but is not readily available in developing country like ours. It's quite expensive if needed to be imported. We used the alternative BS cage, in our cases, which is readily available in our settings and less expensive for the patients. Amenabar et al.27) used BS cages in 9 of his 67 cases of revision hip arthroplasty with satisfactory results. However, there are no previous reports on the use of BS cage and porous cup for acetabular fractures. We emphasize that the ability to use different implant cup-cage combinations is not only the strength of modular acetabular revision, as it allows for customized component combinations for individual patients, but also cost-effective as it decreased the overall cost to the patient to one-fifth due to the low cost of BS cage. Moreover, we were able to achieve similar clinical results with our combination as compared to the original combinations.
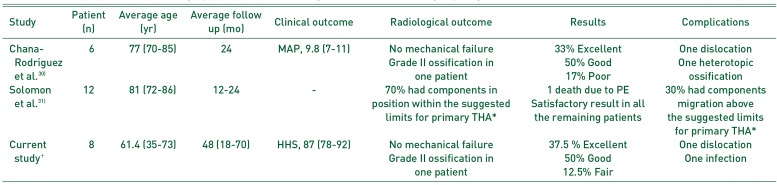
Table 2
Summary of the Patient Demographics and Clinicoradiological Outcomes Following Cup-Cage Construct in Acetabular Fractures from Different Studies
| Study | Patient (n) | Average age (yr) | Average follow up (mo) | Clinical outcome | Radiological outcome | Results | Complications |
|---|---|---|---|---|---|---|---|
| Chana-Rodríguez et al.30) | 6 | 77 (70-85) | 24 | MAP, 9.8 (7-11) | No mechanical failure | 33% Excellent | One dislocation |
| Grade II ossification in one patient | 50% Good | One heterotopic ossification | |||||
| 17% Poor | |||||||
| Solomon et al.31) | 12 | 0.81 (72-86) | 12-24 | - | 70% had components in position within the suggested limits for primary THA* | 1 death due to PE | 30% had components migration above the suggested limits for primary THA* |
| Satisfactory result in all the remaining patients | |||||||
| Current study† | 8 | 61.4 (35-73) | 48 (18-70) | HHS, 87 (78-92) | No mechanical failure | 37.5 % Excellent | One dislocation |
| Grade II ossification in one patient | 50% Good | One infection | |||||
| 12.5% Fair |
![]()
The high cost and hurdles in procuring the implant from overseas prompted the authors to use a routinely available, less expensive BS cage even in revision hip arthroplasty cases for reconstruction. This cage provides the initial stability for the porous metal and substitutes the role of TMARS cage. BS cage is also made of pure titanium (Protasul-Ti) like a TMARS cage. In addition, the problem of design and flexibility of the implant was easily catered by our finding in initial few cases that a size difference of 16 mm between the TMRS and the BS cage was best suited for coupling between the two. This finding of a unique combination between TMRS and BS cage is the other strength of this paper that allows a fellow surgeon to use this technique thereof. Using this technique we could get good to excellent results from short to mid-term follow up of 24 to 72 months. The authors have been routinely using this technique for management of bone defects with or without pelvic discontinuity during revision hip arthroplasty as well.
Go to :
CONCLUSION
This is the first study elucidating the use of BS cage in cup-cage construct with good to excellent results. Although the long-term reports of using cup-cage construct technique in acute acetabular fractures are yet to come up, short to medium term result of using a BS cage with TM shell is encouraging as immediate stability can be achieved, function is restored, pain is relieved, mobilization can be started early, and, hospitalization time is reduced. The authors have made routine use of a combination of a TMRS and BS cage to treat patients requiring a cup-cage construct for patients with acetabular fractures as well as for failed hip arthroplasty. However, these patients need to be followed up further for the long term before reaching a definitive conclusion.
Go to :
 XML Download
XML Download