

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Femoral neck fractures account for approximately half of all hip fractures1). Arthroplasty has become a standard treatment over internal fixation for displaced femoral neck fractures in elderly patients, based largely on the risk of potential complications (e.g., nonunion and avascular necrosis), early ambulation, and functional recovery after surgery2345).
In particular, bipolar hemiarthroplasty (BHA) is the preferred approach because of the short operation time, low dislocation rate, and functional improvements achieved1). However, potential complications, including inguinal pain accompanied by acetabular erosion have not satisfied the demand for higher quality of life due to prolonged lifespan6). Therefore, a few orthopedic surgeons have attempted total hip arthroplasty (THA) in patients with displaced femoral neck fractures178).
Previous studies have reported that THA used to treat femoral neck fractures in elderly patients increases operative time and bleeding compared with BHA, but does not increase mortality; additionally, patients initially exhibit excellent function with shortened hospitalization stays and early ambulation91011). Furthermore, there was no significant difference in long-term clinical results following THA compared with BHA; however, the rate of dislocation was high6).
Nevertheless, comparative studies on BHA and THA have revealed different characteristics associated with these two procedures (e.g., pre-injury functional status, prosthesis type, or average age) among the study groups. In elderly patients, pre-injury activity is a significant factor when considering THA6). The use of cement in the selection of prosthesis should be considered according to the bone condition of the patients12).
Thus, the purpose of this study is to analyze (via a meta-analysis) whether cement use and good pre-injury activity (i.e., independent ambulation) affect clinical outcomes of BHA compared with THA in elderly patients with femoral neck fractures.
Go to : 
MATERIALS AND METHODS
Our current meta-analysis was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline13).
1. Study Eligibility Criteria
Eligible studies met the following inclusion criteria. 1) Randomized controlled trials (RCTs) or non-randomized comparative studies; 2) patients (mean age of >65 years) had displaced femoral neck fractures (Garden type III of IV)14) treated with THA or BHA; 3) a follow-up of at least 1 year; and 4) reported at least one of the following clinical outcomes: one-year mortality, reoperation rate for any cause, dislocation, infection, functional outcome, and mobilization. Studies were excluded if they failed to meet the above criteria.
2. Search Methods for Identification of Studies
A comprehensive search of all relevant RCTs and comparative studies was conducted through PubMed Central, OVID Medline, Cochrane Collaboration Library, Web of Science, EMBASE, KoreaMed, and AHRQ, up to January 2018; languages were restricted to English and Korean. The following search terms were used: (“arthroplasty, replacement, hip” [MeSH Terms] OR (“arthroplasty” [All Fields] AND “replacement” [All Fields] AND “hip” [All Fields]) OR “hip replacement arthroplasty” [All Fields] OR (“total” [All Fields] AND “hip” [All Fields] AND “arthroplasty” [All Fields]) OR “total hip arthroplasty” [All Fields]) OR “femoral neck fracture” [All Fields]) AND (((“random allocation” [MeSH Terms] OR (“random” [All Fields] AND “allocation” [All Fields]) OR “random allocation” [All Fields] OR “randomized” [All Fields]) AND controlled [All Fields] AND study[All Fields]) AND “OR “[All Fields] AND (“comparative study” [Publication Type] OR “comparative study” [All Fields])) AND ((“2001/01/31” [PDAT] : “2018/01/31” [PDAT]) AND “humans” [MeSH Terms]). A manual search of search results was then conducted. Two investigators independently reviewed the titles, abstracts, and full text of all potentially relevant studies, as recommended by the Cochrane Collaboration15).
3. Data Extraction
The following data were extracted from the included articles: authors, publication date, study design, characteristics of the participants, follow-up period, specific interventions, and outcome measurements. The outcomes pooled in this analysis included one-year mortality, reoperations for any cause, dislocation, infection, general complication, functional outcome, and mobilization. For the data published as median, range and the size of the trial, mean difference and standard deviation were calculated by following the method of Hozo et al16).
4. Methodological Quality Assessment
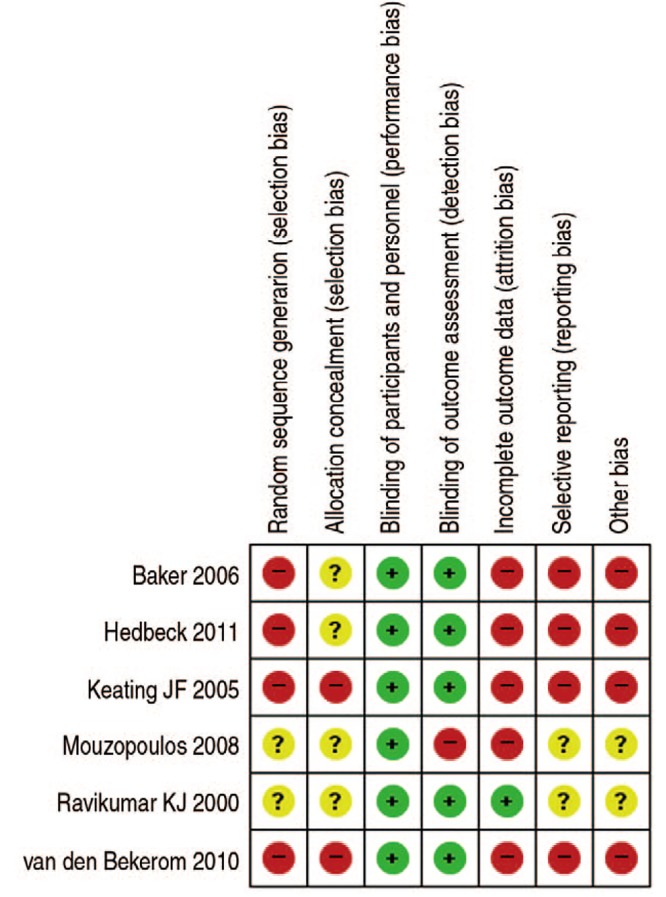
Two authors independently assessed the methodological quality of included studies using the same criteria for RCTs and as described in the Cochrane Handbook for Systematic Reviews of Interventions 5.2 (Fig. 1). Criteria included the following 10 items; 1) allocation concealment, 2) clarity of inclusion and exclusion criteria, 3) use of an intent-to-treat analysis (i.e., outcomes of patients who withdrew or were excluded after allocation described and included), 4) quality of matching or appropriate covariate adjustments, 5) surgeon experience with trial operations prior to commencement, 6) comparative nature of non-surgical care programs, 7) clarity of outcome measure definitions in the text with a definition of any ambiguous terms, 8) blinding status of outcome assessors, 9) appropriateness of the timing of outcome measures, and 10) appropriate reporting of loss to follow-up and percentage of patients loss to follow-up (i.e., greater or less than 5%).
The Newcastle-Ottawa scale was used to assess the methodological quality of non-randomized studies. The scale contains eight items, which are categorized into three dimensions: the selection of the study population, the comparability of the groups, and the ascertainment of the exposure (case-control study) or outcome (cohort study). Each dimension consists of subcategorized questions: selection (a maximum of 4 stars), comparability (a maximum of 2 stars), and exposure or outcome (a maximum of 3 stars)1718). A study can thus be awarded a maximum of 9 stars-a value indicating the highest quality. In the present study, two authors independently evaluated the quality of all assessed studies.
5. Data Analysis
The meta-analysis was performed with Review Manager Software (RevMan 5.3; Cochrane Community, London, UK) and the level of significance was set at P<0.05. For dichotomous outcomes, odds ratio (OR) and 95% confidence interval (CI) were calculated. For continuous outcomes, standardized mean difference and 95% CI were calculated. The size of heterogeneity across studies was estimated with I2 statistic and the chi-squared test. A P-value of >0.10 and an I2 ≤50% were considered to be representative of no statistical heterogeneity18). For the heterogeneity test, we used Higgins I2 statistics. Signi cant heterogeneity was observed in the reviewed studies and we have reported the data from random-effects. A random-effect or fixed-effect model was adopted depending on the heterogeneity of the included studies. Subgroup analysis was performed based on the type of methodological quality (RCT vs. non-RCT) and type of fixation method (cemented vs. cementless), respectively. Sensitivity analysis was conducted by omitting one study in each turn and pooling the data of the remaining studies to explore possible explanations for high heterogeneity and determine the stability of the outcomes.
Go to :
RESULTS
1. Search Results
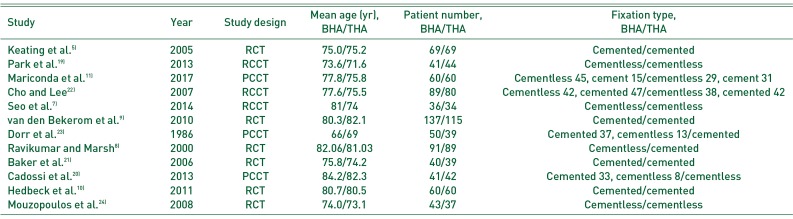
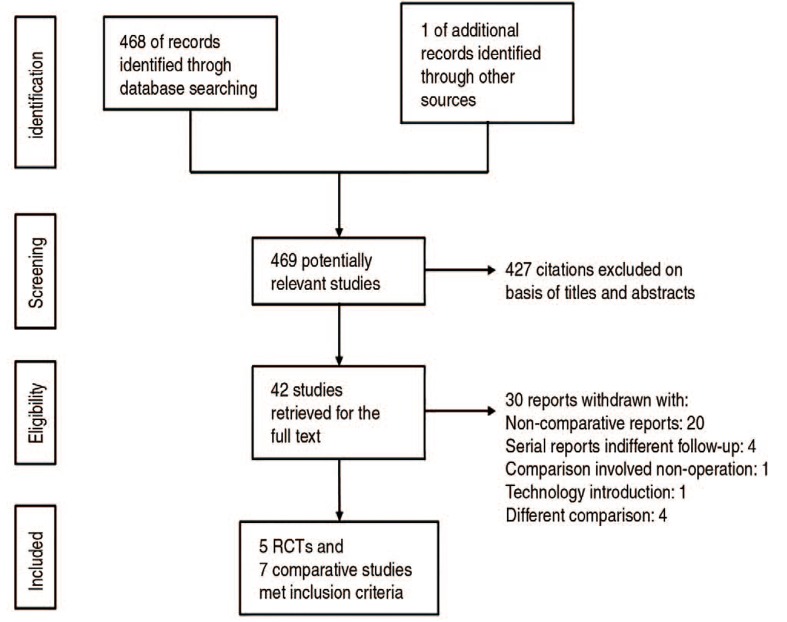
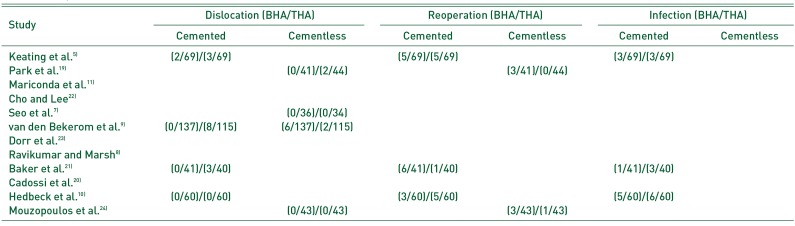
The initial search identified 468 references from the selected databases. Four hundred and twenty-seven references were excluded by screening the abstracts and titles for duplicates, unrelated articles, case reports, systematic reviews, and non-comparative studies. The remaining 42 studies underwent full-text reviews and subsequently, 30 studies were excluded. The details of the identification of relevant studies are shown in the flow chart of the study selection process (Fig. 2). Five randomized controlled studies and seven comparative retrospective studies, including 1,465 patients (708 and 757 forming the THA and BHA groups, respectively) were selected for further investigation. The main characteristics and outcomes of the studies included in the meta-analysis are presented in Table 157891011192021222324). Among these 12 studies, a meta-analysis was performed for each of the four studies with a cemented prosthesis, three studies with a cementless prosthesis, and four studies with a report on pre-injury activity.
 | Fig. 2PRISMA (Preferred Reporting Items for Systematic Reviews) flow diagram representing the details of the process of selecting relevant clinical studies.RCT: randomized controlled trial.
|
Table 1
Characteristics of Included Studies and Patients
| Study | Year | Study design | Mean age (yr), BHA/THA | Patient number, BHA/THA | Fixation type, BHA/THA |
|---|---|---|---|---|---|
| Keating et al.5) | 2005 | RCT | 75.0/75.2 | 69/69 | Cemented/cemented |
| Park et al.19) | 2013 | RCCT | 73.6/71.6 | 41/44 | Cementless/cementless |
| Mariconda et al.11) | 2017 | PCCT | 77.8/75.8 | 60/60 | Cementless 45, cement 15/cementless 29, cement 31 |
| Cho and Lee22) | 2007 | RCCT | 77.6/75.5 | 89/80 | Cementless 42, cemented 47/cementless 38, cemented 42 |
| Seo et al.7) | 2014 | RCCT | 81/74 | 36/34 | Cementless/cementless |
| van den Bekerom et al.9) | 2010 | RCT | 80.3/82.1 | 137/115 | Cemented/cemented |
| Dorr et al.23) | 1986 | PCCT | 66/69 | 50/39 | Cemented 37, cementless 13/cemented |
| Ravikumar and Marsh8) | 2000 | RCT | 82.06/81.03 | 91/89 | Cementless/cemented |
| Baker et al.21) | 2006 | RCT | 75.8/74.2 | 40/39 | Cemented/cemented |
| Cadossi et al.20) | 2013 | PCCT | 84.2/82.3 | 41/42 | Cemented 33, cementless 8/cementless |
| Hedbeck et al.10) | 2011 | RCT | 80.7/80.5 | 60/60 | Cemented/cemented |
| Mouzopoulos et al.24) | 2008 | RCT | 74.0/73.1 | 43/37 | Cementless/cementless |
![]()
2. Cemented Prosthesis
1) One-year mortality
Four studies with a total of 510 participants reported the mortality rate with 244 and 266 patients assigned to the THA and BHA groups, respectively591021). There was low evidence of heterogeneity across the studies (I2=0%, P=0.74) and the fixed-effect model was performed. There was no statistical difference between the two groups (OR, 1.00; 95% CI, 0.56–1.79; P=1.00, Z=0.00) (Fig. 3).

2) Complications
Four studies with a total of 591 participants reported dislocation rates and 284 and 307 patients were assigned to the THA and BHA groups, respectively591021). There was low evidence of heterogeneity across the studies (I2=30%, P=0.24) and the fixed-effect model was performed. Dislocation rate was significantly higher in those treated with cemented THA compared with patients treated with cemented BHA (OR, 0.18; 95% CI, 0.05–0.62; P=0.006, Z=2.73) (Fig. 4A and Table 2).
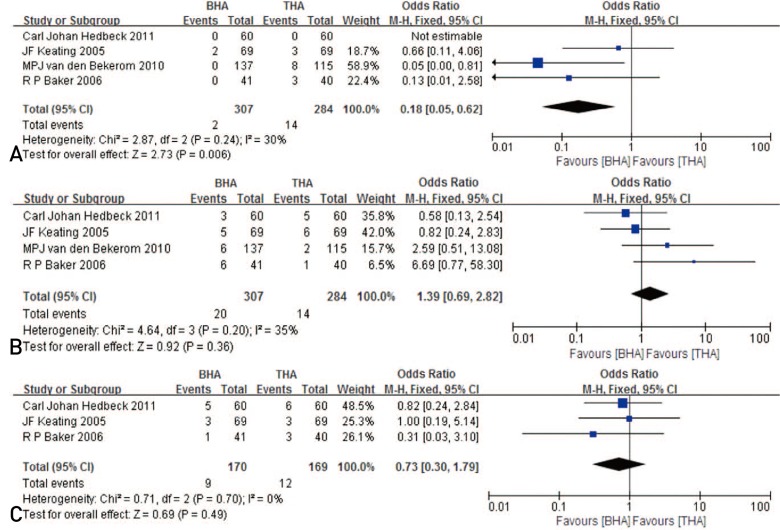 | Fig. 4(A) Forest plot of the dislocation rates comparing the experimental (THA) and control (BHA) groups in those treated with cemented prosthesis. (B) Forest plot of reoperation rates comparing the THA and BHA groups in those treated with a cemented prosthesis. (C) Forest plot of infection rates comparing the THA and BHA groups in those treated with a cemented prosthesis.THA: total hip arthroplasty, BHA: bipolar hemiarthroplasty, CI: confidence interval, M-H: Mantal-Haenszel.
|
Table 2
Complication Rates of Included Studies and Patients
| Study | Dislocation (BHA/THA) | Reoperation (BHA/THA) | Infection (BHA/THA) | |||
|---|---|---|---|---|---|---|
| Cemented | Cementless | Cemented | Cementless | Cemented | Cementless | |
| Keating et al.5) | (2/69)/(3/69) | (5/69)/(5/69) | (3/69)/(3/69) | |||
| Park et al.19) | (0/41)/(2/44) | (3/41)/(0/44) | ||||
| Mariconda et al.11) | ||||||
| Cho and Lee22) | ||||||
| Seo et al.7) | (0/36)/(0/34) | |||||
| van den Bekerom et al.9) | (0/137)/(8/115) | (6/137)/(2/115) | ||||
| Dorr et al.23) | ||||||
| Ravikumar and Marsh8) | ||||||
| Baker et al.21) | (0/41)/(3/40) | (6/41)/(1/40) | (1/41)/(3/40) | |||
| Cadossi et al.20) | ||||||
| Hedbeck et al.10) | (0/60)/(0/60) | (3/60)/(5/60) | (5/60)/(6/60) | |||
| Mouzopoulos et al.24) | (0/43)/(0/43) | (3/43)/(1/43) | ||||
![]()
Four studies with a total of 591 participants reported reoperation rates, and 284 and 307 patients were assigned to the THA and BHA groups, respectively591021). There was low evidence of heterogeneity across the studies (I2=35%, P=0.20) and the fixed-effect model was performed. There was no statistical difference between the cemented THA group and the cemented BHA group (OR, 1.39; 95% CI, 0.69–2.82; P=0.36, Z=0.92) (Fig. 4B).
Three studies with a total of 339 participants reported infection rates, and 169 and 170 patients were assigned to the THA and BHA groups, respectively51021). There was low evidence of heterogeneity across the studies (I2=0%, P=0.70) and the fixed-effect model was performed. There was no statistical difference between the cemented THA group and the cemented BHA group (OR, 0.73; 95% CI, 0.30-1.79; P=0.49, Z=0.69) (Fig. 4C).
3) Functional scores
Three studies with a total of 510 participants reported Harris hip scores (HHS) with 244 and 266 patients assigned to the THA and BHA groups, respectively5910). There was high evidence of heterogeneity across the studies (I2=65%, P=0.09) and the fixed-effect model was performed. There was no statistical difference between the cemented THA group and the cemented BHA group (OR, −3.12; 95% CI, −6.49 to 0.26; P=0.07, Z=1.81) (Fig. 5A).
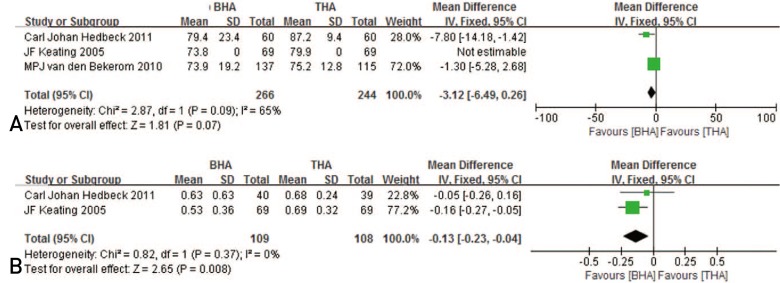 | Fig. 5(A) Forest plot of Harris hip score comparing the experimental (THA) and control (BHA) groups in those treated with a cemented prosthesis. (B) Forest plot of EQ-5D comparing the THA and BHA groups in those treated with a cemented prosthesis.THA: total hip arthroplasty, BHA: bipolar hemiarthroplasty, SD: standard deviation, CI: confidence interval.
|
Two studies with a total of 217 participants reported the EQ-5D with 108 and 109 patients assigned to the THA and BHA groups, respectively510). There was low evidence of heterogeneity across the studies (I2=0%, P=0.37) and the fixed-effect model was performed. EQ-5D was significantly higher in the cemented THA group compared with the cemented BHA group (OR, −0.13; 95% CI, −0.23 to −0.04; P=0.008, Z=2.65) (Fig. 5B).
3. Cementless Prosthesis
1) One-year mortality
One study reported one-year mortality rates24). The authors reported that there was no statistical difference between the two groups (13/43 in cementless BHA group vs. 10/43 in cementless THA group).
2) Complications
Three studies with a total of 241 participants reported dislocation rates, and 121 and 120 patients were assigned to the THA and BHA groups, respectively71924). The heterogeneity could not be evaluated and the fixed-effect model was performed. No statistical difference was observed between the cementless THA group and the cementless BHA group (OR, 0.20; 95% CI, 0.01–4.40; P=0.31, Z=1.01) (Fig. 6A and Table 2).
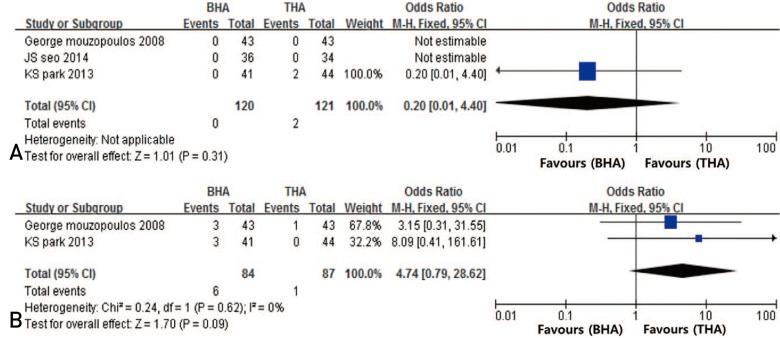 | Fig. 6(A) Forest plot of dislocation rates comparing the experimental (THA) and control (BHA) groups in those treated with cementless prosthesis. (B) Forest plot of reoperation rates comparing the THA and BHA groups in those treated with a cementless prosthesis.THA: total hip arthroplasty, BHA: bipolar hemiarthroplasty, CI: confidence interval, M-H: Mantal-Haenszel.
|
Two studies with a total of 171 participants reported reoperation rates, with 87 and 84 patients assigned to the THA and BHA groups, respectively1924). There was low evidence of heterogeneity across the studies (I2=0%, P=0.62) and the fixed-effect model was performed. There was no statistical difference between the cementless THA group and the cementless BHA group (OR, 4.74; 95% CI, 0.79–28.62; P=0.09, Z=1.70) (Fig. 6B).
However, the statistical analysis of the infection rate could not be performed because there were no cases of infection in those treated with cementless fixation.
3) Functional scores
Two studies with a total of 150 participants reported HHS with 71 and 79 patients assigned to the THA and BHA groups, respectively724). There was high evidence of heterogeneity across the studies (I2=93%, P=0.00) and the fixed-effect model was performed. HHS was significantly higher in the cementless THA group compared with the cementless BHA group (OR, −6.59; 95% CI, −9.54 to −3.65; P=0.00, Z=4.38) (Fig. 7).

4. Independent Ambulation
1) Dislocation, reoperation, infection
Four studies reported dislocation rates. There were a total of 418 participants, with 206 and 212 patients assigned to the THA and BHA groups, respectively19202122). There was low evidence of heterogeneity across the studies (I2=0%, P=0.97) and the fixed-effect model was performed. Dislocation rate was significantly higher in the THA group compared with the BHA group (OR, 0.17; 95% CI, 0.03–0.98; P=0.05, Z=1.98) (Fig. 8A and Table 2).
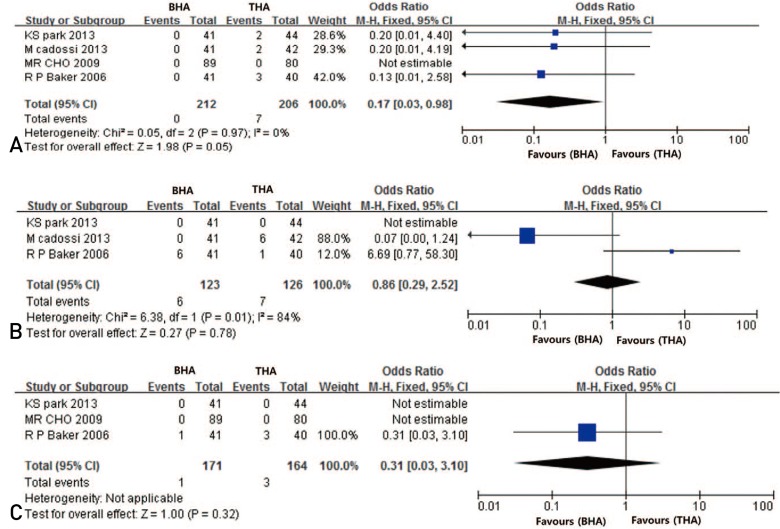 | Fig. 8(A) Forest plot of dislocation rates comparing the experimental (THA) and control (BHA) groups in a subgroup analysis including independent walkers. (B) Forest plot of reoperation rates comparing the THA and BHA groups in a subgroup analysis including independent walkers. (C) Forest plot of infection rates comparing the THA and BHA groups in a subgroup analysis including independent walkers.THA: total hip arthroplasty, BHA: bipolar hemiarthroplasty, CI: confidence interval, M-H: Mantal-Haenszel.
|
Three studies reported reoperation rates. There were a total of 249 participants with 123 and 126 patients assigned to the THA and BHA groups, respectively192021). There was high evidence of heterogeneity across the studies (I2=84%, P=0.01) and the fixed-effect model was performed. There was no statistical difference between the THA and BHA groups (OR, 0.86; 95% CI, 0.29–2.25; P=0.78, Z=0.27) (Fig. 8B).
Three studies reported infection rates192122). There were a total of 335 participants with 164 and 171 patients assigned to the THA and BHA groups, respectively. The heterogeneity could not be evaluated and the fixed-effect model was performed. There was no statistical difference between the THA and BHA groups (OR, 0.31; 95% CI, 0.03–3.10; P=0.32, Z=1.00) (Fig. 8C).
5. Risk Bias
Five RCTs and seven comparative studies reported on the risk of bias. The Cochrane Handbook for Systematic Reviews of Interventions was used to assess the quality of two RCTs. Scoring in five RCTs was done from four to seven points. The Newcastle-Ottawa scale was used to assess the quality of the selected studies. All included studies scored between five and eight points, indicating relatively high quality. A funnel plot was not applied to assess publication bias due to the small size (<10) of RCTs included in this meta-analysis.
Go to :
DISCUSSION
The major findings of this study are as follows: 1) the use of a cemented prosthesis for femoral neck fractures in elderly patients was associated with a higher dislocation rate in the THA group compared with the BHA group; 2) there were no difference the in dislocation rates of the THA and BHA groups when a cementless prosthesis was used; 3) THA for femoral neck fractures in the elderly yielded higher functional results compared with BHA; however, there was no difference in 1-year mortality between these groups; and 4) dislocation rates in elderly patients with femoral neck fractures treated with THA who were independent walkers prior to injury was higher compared with those treated with BHA.
The extent of the use of bone cement when conducting arthroplasty varies depending on a number of factors (e.g., bone condition of a patient, surgical techniques, or personal preferences of surgeons). Many studies analyzed outcomes with long term follow-up and revealed no significant differences between cemented and cementless hemiarthroplasty in terms of morbidity, mortality or length of hospital stay252627). Furthermore, researchers have reported a trend toward poorer functional results in patients treated with cementless hemiarthriplasty compared with those treated with cemented hip arthroplasty. However, the choice between cemented or cementless prosthesis for treatment of displaced femoral neck fractures in the elderly continues to be debated despite the presence of numerous studies on the subject28). Also, the routine use of cement in elderly patients has been reported to be a technically more demanding procedure and may be associated with cardiopulmonary complications2930). Therefore, it has been stated that potential complications associated with THA (e.g., extensive bleeding or longer operation time) may result in an increase in cardiopulmonary loading compared with BHA, leading to higher morbidity rates. However, in the present study, no difference was observed. Older studies have reported no differences between the morbidity and mortality rates of cemented hemiarthroplasty and cementless hemiarthroplasty or the morbidity rates of cemented THA and cementless THA25262731). Furthermore, no difference in the morbidity rates associated with THA and BHA were observed in elderly patients with femoral neck fractures. The studies reviewed in this analysis report a similar pattern when comparing cemented BHA and THA as well as with cementless BHA and THA. It could thus be concluded that no increase in morbidity rates should be expected regardless of: 1) the use or omission of cement or 2) the type of prosthesis used1). Also, as reported previously, our meta-analysis revealed that there were no statistically significant differences between the rate of infections, general complications, or re-operation rates in the BHA and THA groups irrespective of cement use91011).
Previous studies reported that patients treated with THA achieved greater functional results13233). The present study confirms that consistently greater functional results in the group with THA were achieved regardless of whether or not cement was used. Despite being associated with a high dislocation rate, the reason for attempting THA in elderly patients with femoral neck fractures with favorable pre-injury activity is due to concerns about the inactivity of the patient resulting from inguinal pain caused by acetabular erosion and achieving greater functional results91034). However, the use of cemented THA was associated with a significantly higher rate of dislocation compared with cemented BHA, while there was no difference in the dislocation rates between the cementless THA and cementless BHA groups. The use of a cemented prosthesis in elderly patients is technically demanding and may affect the formation of a cement mantle28); it is hypothesized that these problems might have influenced the stability of the prosthesis and hip joint by unoptimal position of the prosthesis, offset, and leg length. Thus, the use of cement may help explain the difference in dislocation rates between those treated with THA compared with BHA. However, considering the variation in the number of factors affecting dislocation, it cannot be stated that cemented fixation of THA in elderly patients with femoral neck fractures should not be implemented.
In this study, the risk of dislocation after THA in pre-injury independent walker patients was higher than in those treated with BHA. It is possible that preinjury activity may be associated with a difference in dislocation rates between these two types of prostheses. The dislocation rate of those treated with THA was observed to increase in active people35). The dual articulation of BHA may help prevent the rate of dislocations in patients with high pre-injury. The principle of joint motion of a dual-mobility prosthesis is similar to the joint motion mechanism of BHA. A comparison of dual-mobility prostheses with conventional THA revealed that the dual-mobility prosthesis was associated with a low rate of dislocations, similar to the results of this study36). However, we cannot definitively state that BHA should be performed over THA in elderly patients with femoral neck fractures and who were pre-injury independent walkers. The overall clinical outcomes, including functional results, should be taken into consideration. However, careful attention should be paid to complications potentially affecting high-activity patients considering the differences in prosthesis mechanism during the postoperative follow-up.
Our systematic review has several limitations. First, the search was restricted to RCTs and comparative studies published in peer-reviewed journals, excluding other sources of biomedical literature that could have possibly provided additional relevant studies. In such a case, studies with positive or statistically significant results would be expected to be over-represented in our review, as such studies were more likely to be published, particularly in the English language. Second, the validity of our results is limited by the low quality of the included studies; double-blinding was not used in most of the trials, which may decrease the strength of our conclusions. Third, there is the potential for bias because of the high heterogeneity in some comparisons, which may have affected the pooled results. Studies brought together in a meta-analysis will inevitability differ, and any type of variability among studies may be termed heterogeneity. The included studies had clinical heterogeneity caused by variability in the participants (e.g., age, gender, comorbidities, and preoperative ambulatory status), interventions (e.g., instrumentation from different manufacturers, different surgeons), outcomes (e.g., selective reporting and data deficiency), and methodological heterogeneity caused by variability in study design and risk of bias. Lastly, it is not sufficient to analyze the position of the prosthesis, which is the most important factor related to dislocation in patients undergoing THA.
Go to :
CONCLUSION
When THA was performed in elderly patients with femoral neck fractures and who were independent walkers prior to their injury, the dislocation rate increased. In addition, cemented THA was associated with a higher dislocation rate compared with cemented BHA. However, cementless THA was associated with a similar dislocation rate compared with cementless BHA. With regards to functional score, THA was superior to BHA in both cementless and cemented fixation.
Go to :
 XML Download
XML Download