

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The use of hip arthroscopy to treat a symptomatic dysplastic hip has been suggested; however, this approach is also a matter of some debate. While a number of studies reported favorable outcomes, a high percentage of patients undergoing hip arthroscopy for a dysplastic hip-defined as a lateral center edge (LCE) angle less than 20°-have been reported to require re-operations (e.g., total hip arthroplasty [THA])12). Theoretically, hip dysplasia may create instability due to the lack of osseous support, thus providing excessive stress on the labrum and cartilage potentially leading to osteoarthritis34). As the underlying deficiency acetabulum remains uncorrected during the arthroscopy procedure, it would seem likely that preoperative pain would recur if the patients return to their preoperative activity level.
Contrary to classic dysplasia, the use of hip arthroscopy to treat borderline dysplasia of the hip-defined as a LCE angle between 20° to 25°-remains even more controversial. It can be hypothesized that the mechanism of pain development in those with borderline dysplasia may be similar to those with a dysplastic hip; however, this connection is still not fully understood. A review of the available literature for the use of hip arthroscopy for treatment of borderline dysplasia of the hip reveals that favorable results have been achieved using simple treatments of intra-articular pathologies and by manipulation of acetabular capsule. However, reports on this topic are still limited and are largely confined to high-volume institutions. Thus, in this study, we report outcomes of symptomatic patients with underlying borderline dysplasia treated with commonly used arthroscopic methods. Additionally, we investigated factors that may influence surgical outcomes.
Go to : 
MATERIALS AND METHODS
In the current study, borderline dysplasia is defined as LCE angle between 20° and 25° as measured using simple pelvis anteroposterior radiograph. In this retrospective analysis of a prospective database, we reviewed the outcomes of patients who had a painful hip with underlying borderline dysplasia treated using arthroscopy. The study has been approved by the institutional review board at Chosun University (2019-03-018).
We identified patients who had painful hip with borderline hip dysplasia that were treated using hip arthroscopy in two university hospitals between March 2015 and December 2017. For inclusion in this study, patients were required to have: 1) hip arthroscopy with underlying borderline hip dysplasia, 2) Tönnis grade 0 or 1 at the time of the operation5), and 3) hip arthroscopy as primary and sole procedure. The exclusion criteria are: 1) operation following high energy injury, 2) underlying comorbidities that may have effect on the hip joint (e.g., rheumatoid arthritis, general laxity), and 3) age under 18 years. Forty-seven hips (45 patients) fulfilled all inclusion and exclusion criteria; this cohort is included in our study.
The mean age of patients was 39.2±11.8 years and included 17 males and 30 females. The mean time interval from the development of pain and the surgery was 14.2±9.3 months (range, 3–48 months). The mean LCE angle prior to the surgery was 21.8° (range, 20°–25°).
All operations were performed by two surgeons who each perform more than 50 hip arthroscopies per year. Prior to the surgery, patients were evaluated using simple X-ray (i.e., pelvis anteroposterior, hip lateral, false profile view, and Dunn 45° and 90° view). Additionally, either magnetic resonance imaging or magnetic resonance arthrogram was used to confirm the underlying intra-articular pathology. Patients had a minimum of 3 months of conservative treatment prior to the surgery. Intra-articular analgesic injection was used when necessary to confirm the diagnosis that the pain was from the hip joint. The chief complaint of patients before the surgery was pain around the hip joint that, in all cases, was severe enough to interfere with everyday life.
1. Description of Surgical Procedures
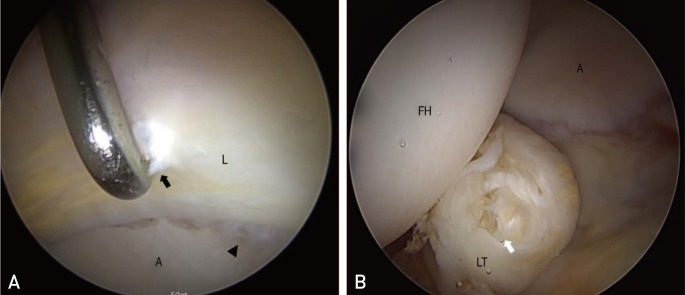
Operations were performed in either the supine or lateral decubitus positions according to the surgeons' preferences and clinical expertise. On distraction, conventional anterolateral portal was established under C-arm guide and subsequent anterior portal was created with direct visualization. In cases where thick labrums interfere with creating the anterior portal, the portal was placed more distally or additional traction was made. Initially, joint spaces were inspected with 70° scope to find evidence of labral injury, cartilage injury (acetabular labrum articular disruption, ALAD grade), ligamentum teres injury and synovitis. The findings on intra-articular pathology were recorded (Fig. 1). When a labral tear was observed, transportal capsulotomy was performed and the labrum was repaired or debrided depending on the stability of the labrum. In cases where labral repair was conducted, rim resection was minimized. Also, in the presence of ligamentum teres injury, debridement and thermal shrinkage was performed. Switching to a 30° scope was done when necessary. Osteochondroplasty (bumpectomy) of the femur was performed when necessary and in these cases, an additional T-shape capsulotomy was created. On completion of treatment for intra-articular pathology, the capsules were either left alone, or repaired with a large stitch on both sides of the capsule to perform plication. In cases where capsulotomy was not performed, capsules were either left alone or was shrunk using a thermal probe.
2. Patient Outcome Assessment and Radiographic Evaluation
Patient outcomes were assessed using modified Harris Hip Score (mHHS)6), Nonarthritic Hip Score (NAHS)7), visual analogue scale (VAS)8), and patient satisfaction. The outcome scores were measured in the out-patient office or through a detailed telephone interview at the last follow up, which was at a minimum of one year. Additional VAS was measured three months following the operation at the out-patient office. Patient satisfaction was determined by asking the patient whether they are satisfied or dissatisfied with the results of their treatment at the last follow up. Patients who experienced recurrent pain were asked to provide the time interval (i.e., between time of the surgery and when the pain recurred). The radiographs were also taken to evaluate the occurrence or progression of arthritis which was graded according to Tönnis grade5). Additionally, patients were interviewed to determine whether the patient had undergone additional surgery or was referred to another institution(s).
3. Statistical Assessment
Statistical analysis was performed using IBM SPSS Statistics software (version 25; IBM Corp, Armonk, NY, USA). Paired t-test was used to compare outcomes (postoperative measurements compared with preoperative measurements). Univariate logistic regression analysis was performed to identify factors that may contribute to poor outcomes using satisfaction as the dependent variable and operation method on capsule, labrum and ligamentum teres, age, gender, body mass index (BMI) and preoperative patient reported outcome scores as covariates. A P-value less than 0.05 was regarded as significant. The unadjusted odd ratios were calculated with 95% confident intervals.
Go to :
RESULTS
Synovitis was observed in all cases. Labral tears and ligamentum teres injuries were noted in 38 and 20 hips, respectively. Cartilage damage with ALAD grade three and higher was observed in four hips (Table 1). Overall, labral tears were repaired in 33 hips and debrided in five. The procedures performed according to each pathology were summarized in Table 2.

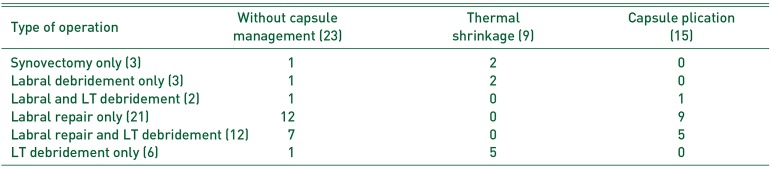
Table 1
Documentation of Intra-articular Pathologies from Arthroscopic Visualization
| Operative findings | ALAD grade 0-2 | ALAD grade 3-4 |
|---|---|---|
| No pathologic lesions (3) | 3 | 0 |
| Labral tear without LT tear (24) | 22 | 2 |
| Labral tear with LT tear (14) | 12 | 2 |
| LT tear without labral tear (6) | 6 | 0 |
![]()
Table 2
Management of Pathologic Lesion and Capsule
![]()
The mean follow up period was 25.9±11.1 months. All patients experienced pain relief following the surgery and the mean VAS score improved from 6.1±1.6 to 2.1±1.0 at the three month follow up (P<0.001) and changed to 3.5±2.8 (P=0.016) at the last follow up. The mHHS and NHAS at last follow up improved from 61.0±7.6 to 78.6±19.5 (P=0.001) and 62.1±7.5 to 80.0±18.5 (P=0.002), respectively. While significant improvement based on patient reported outcome measures was noted, 19 (40.4%) hips indicated that the operation was unsatisfactory at the last follow up as pain had returned. Five hips indicated that the pain had reached preoperative state, seven noted some minimal improvement and seven indicated that the pain was aggravated compared with the preoperative state. Of the 19 hips unsatisfied with their operation, six noted that the pain recurred after loss of the crutch (typically four to six weeks following the operation), and 11 indicated that the pain returned when they returned to the preoperative level of activity (typically at three to six months following the operation).
Poor preoperative VAS was the only factor found to be significantly correlated with patients' satisfaction (P=0.023). We found no significant difference in patients' satisfaction according to age, gender, BMI, LCE angle and management of the capsule, the ligamentum teres and the labrum (P>0.05) (Table 3).
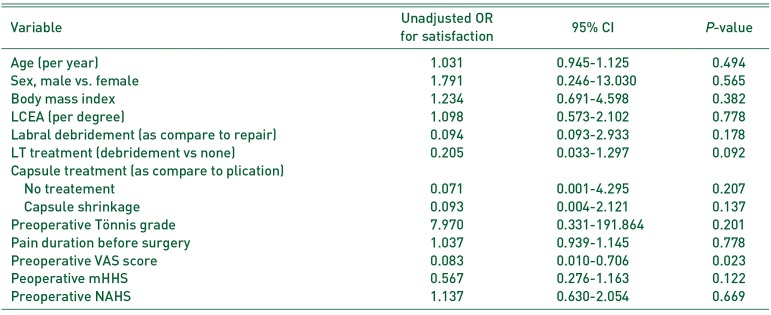
Table 3
Assessment for Risk Factors for Poor Outcome (Satisfied vs. Non-satisfied)
![]()
The acquisition of the last follow up radiograph was possible in 34 hips (taken at a mean of 22.1±10.4 months from the initial surgery). Of these 34 hips, the initial Tönnis grade was 0 (n=28) and 1 (n=6). Two index grade 1 hips had aggregated to grade 2, 4 grade 0 hips had aggregated to grade 1 and one grade 0 hips had aggregated to grade 3 at the last follow up. All patients who had alteration in the joint space (7 hips) were unsatisfied with the surgery (Fig. 2).
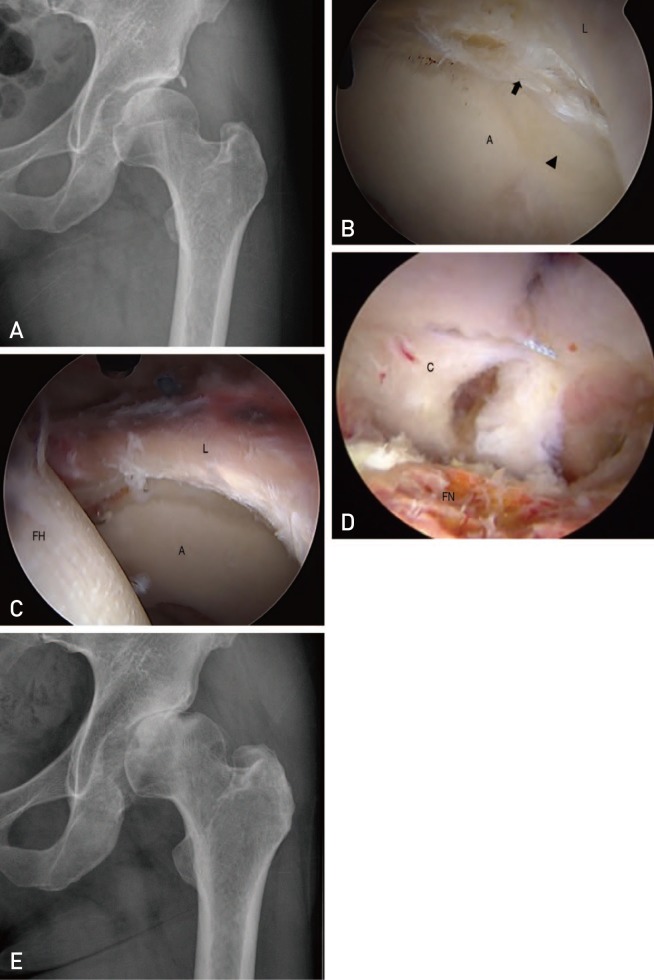 | Fig. 2(A) A 47-year-old female with a painful left side hip revealing lateral center edge angel of 24°. (B) Labral tear (black arrow) was noted with cartilage degeneration (arrowhead) which was treated with. (C) Labral repair using mattress suture and (D) capsular plication. (E) The patient did not achieve satisfactory results, instead developed osteoarthritis at 1 year follow up.A: acetabulum, FH: femoral head, FN: femoral neck, L: labrum.
|
Four hips underwent second-look hip arthroscopy at mean of 10.4 months from the index operation at the same institution. All reoperated hips were found to have aggravated cartilage delamination at the reoperation. Other than these patients, no patients had additional surgery at the last follow up; however, nine were referred for pelvic osteotomy or hip arthroplasty at another referral center.
Go to :
DISCUSSION
The results of the current study indicate that while arthroscopic management may be helpful for a subset of patients with borderline dysplasia, a substantial number of patients may be dissatisfied with the results of this treatment approach. Additionally, we note that the preoperative pain score appears to be the sole indicator (of those investigated) of poor outcomes.
The increased joint pressure in deficient acetabular coverage has been suggested to be a predisposing factor for the development of osteoarthritis. As such a condition is difficult to replicate in an in-vivo setting, most of the field's knowledge is theoretically derived from indirect testing (e.g., finite element analysis)910). The study by Henak et al.11) revealed that the labrum in a dysplastic hip supports 4% to 11% of the total load transfer to the hip joint compared with 1% to 2% in a normal joint, indicating that a labrum injury may occur in a dysplastic hip11). A number of clinical studies have validated this hypothesis by observing a positive association between hip dysplasia and osteoarthritis development12).
On the other hand, the effect of borderline dysplasia on the hip joint, more specifically to the labrum and the cartilage, is still not fully understood. Recently, a study by Irie et al.13) reported an association between borderline to mild dysplasia and hip osteoarthritis. Their study evaluated patients with developmental dysplasia of the hip using computed tomography scans and concluded that: i) cumulative hip stress distribution was not concentrated on the lateral side of acetabulum in their patent cohort and ii) the mechanism of failure may be different than in cases of severe dysplasia. While there are debates on the effect of arthroscopy for the treatment of a dysplastic hip, most studies report favorable outcomes of arthroscopic treatment for borderline dysplasia. Ding et al.14) recently summarized the results from all available literatures on this topic. In their systematic review of 425 patients from 9 studies, the overall failure rate was recorded to be 14.1% with a mean reoperation rate of 8.5%. All studies uniformly reported improvement in outcome measures assessed.
However, our results contradict previous studies. While we noted improve pain in a substantial number of the hips included in our analysis, however, 40% classified their results as unsatisfying. The immediate pain resolution observed in all patients is likely due to the treatment of synovitis or simple washout effect of the arthroscopy procedure15). We are unable to identify the reason for this substantial discordance in our results with those previously reported. It can be suggested that the surgical technique of the operator may be a relevant factor that influences surgical outcomes. Nonetheless, the surgeons who performed the surgeries on the patients included in the current study perform a number of operations that far exceeds the number that is suggested to reach the learning curve plateau161718). Therefore, while the surgeon's technique may be a contributing factor, it is important to note that most non high-volume surgeons would likely face similar outcomes. Another well-known issue to consider is the well-accepted notion that negative results are not commonly published19). A study by Fanelli20) assessed the frequency of positive results in publication and reported that “the papers are less likely to be published and to be cited if they are reporting ‘negative’ results”. For this reason, and although most studies on this topic report favorable outcomes, we think it is necessary to report these negative results as well to broaden the field's understanding of this controversial topic. Upon a review of the available literature, two studies with results comparable to those reported here were identified. Kalore and Jiranek21) reported outcomes of 50 patients with borderline dysplasia and noted a failure rate of 46%. The study by Parvizi et al.22) reported that in an analysis of 34 hips with borderline dysplasia, 47% of patients required reoperation after 2 years of follow up. However, it should be noted that the arthroscopic maneuver on the capsule is not documented in detail in either study and it is likely that these studies may have not manipulated the capsule in the same manner as described in this study.
This leads to the second important finding of the current study revealing that contemporary operation methods may have a limited role in borderline dysplasia of the hip. A study by Chandrasekaran et al.23) reported 2-year outcomes following capsular plication, with favorable outcomes achieved in 79.5% of cases; these findings led the surgeons in the current study to start capsule plication. As capsular plication has been suggested as a procedure that may provide tightness to the dysplastic hip, it can be suggested that abundant capsule release in the arthroscopic procedure, an approach which is routinely done to manipulate the instrument within the joint, may aggravate the symptom2425). However, even with capsule plication, we were unable to find significant improvements in patient outcomes. In our study, four of the seven cases with detrimental outcomes were patients with unrepaired T-shape capsulotomy; additionally, two patients with capsule plication experienced aggravated pain. Thus, we were unable to either confirm or refute the hypothesis that the absence of capsular management may have attributed to poor outcomes in the described patient cohort. It is the opinion of the authors that sutures for plication may not be sufficient to manage hip movement torque, which typically reaches more than 10 Nm26).
Previous studies have suggested that advanced age, labral debridement, preoperative cartilage status, and deficient anterior coverage to be risk factors for poor outcomes; however, these notions have also been challenged in other papers21272829). Importantly, these possible risk factors were not correlated with outcomes in this analysis. In fact, the only risk factor we observed was the preoperative pain score. Specifically, patients who had significant pain prior to the surgery were more likely to have poor outcomes. While this may be an important finding, it is also important to note that there could be other factors that may contribute to poor outcomes, including those that are the cause of the severe pain in those with borderline dysplasia. As the natural history of the borderline dysplastic hip is not understood, our results do not provide answers to this question.
We acknowledge several limitations of the current manuscript. First, the number of patient cohort may be too small to make broad inferences. The 47 hip that are included were not sufficient to perform multivariate analysis which would support the analysis of risk factors for poor outcomes and validating the effect of each operation procedure. The authors do note a rather poor result in those patients who had already undergone hip arthroscopy and concluded that it would be unethical to perform additional surgery without defining factors that may positively or negatively affect the outcome. Second, the follow-up period may be too short. All patients in the current study had a minimum of one-year follow up and we believe that this time frame is sufficient to identify the effects of the arthroscopy on outcomes. However, we also think these results may be more discouraging with longer follow up. The short follow up in the study is probably the reason why the percentage of those requiring reoperation and/or conversion to THA is not a high as previous reports. Third, the study does not include the quality of the labral and ligamentum teres injury or quality of the operation performed (i.e., amount of capsular plication, adequacy of ostechondroplasty). As this is a retrospective review and the operation was performed by two surgeons at different institutions, we were unable to objectively classify intra-operative findings and these remains as an important limitation to the current study.
Go to :
CONCLUSION
The current study reports the outcomes of almost fifty hip arthroscopies performed on patients with borderline hip dysplasia. The results of the current study indicate that arthroscopic management may be beneficial for a subset of patients with borderline dysplasia. However, the study also reveals that even with the contemporary technique: i) operations may not be satisfactory in a substantial portion of patients and ii) the preoperative pain score should be considered when performing arthroscopic procedure in the hips with borderline dysplasia. However, what additional factors may contribute to the development of severe pain preoperatively remains an important unanswered question.
Go to :
 XML Download
XML Download