

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Atrial fibrillation (AF) is the most prevalent arrhythmia in the elderly and requires adequate anticoagulation therapy for prevention of stroke. Frequently, patients with AF also have coronary atherosclerosis,1 for which percutaneous coronary intervention (PCI) should be performed either by an urgent or elective procedure. The optimal antithrombotic therapy for patients with AF undergoing PCI is challenging, as the balance between bleeding and thrombotic risk should be weighed.
Until recently, most of the guidelines recommended triple therapy, including anticoagulation plus dual antiplatelet agents (dual antiplatelet therapy [DAPT]), as the standard practice.23 However, triple therapy causes substantially increased major bleeding events, as high as 12% in the first year of treatment,4 and the risk of bleeding is 3-fold higher compared to that of warfarin therapy alone.5 Among fatal bleeding events, more than 30% are intracranial hemorrhage,67 one of the most dreadful complications. Therefore, an attempt to find a new antithrombotic strategy with a reduced bleeding risk was initiated.
The WOEST trial, which compared dual therapy with warfarin and clopidogrel vs. triple therapy for patients who required anticoagulation and underwent PCI, demonstrated significantly lower bleeding risk with similar major adverse cardiovascular events (MACEs) in the dual therapy group.8 Despite not all of the study participants having AF as the indication for anticoagulation, the trial suggested that dual therapy can be more appropriate by preventing excessive bleeding in patients with AF who underwent PCI. Furthermore, since the bleeding risk is lower with a non-vitamin K antagonist oral anticoagulant (NOAC) than a vitamin K antagonist,910 dual therapy using an NOAC may yield much fewer bleeding events. The following two, large, randomized, controlled trials investigated the bleeding risk and efficacy of dual antithrombotic strategy with either rivaroxaban or dabigatran.
PIONEER AF-PCI TRIAL
The PIONEER AF-PCI trial was an international, multicenter, randomized, open-label trial that enrolled 2,124 patients with nonvalvular AF who had just undergone PCI with stenting.11 The overview of the study design is shown in Table 1. Patients with documented AF within 1 year before screening were included, but patients with AF of more than 1 year duration who received anticoagulation therapy for AF for 3 months preceding the PCI were also eligible. Major exclusion criteria were a history of stroke or gastrointestinal bleeding within 12 months and creatinine clearance less than 30 mL/min. Patients were randomly allocated to groups 1 to 3 at a 1:1:1 ratio within 72 hours after PCI and stratified by treatment duration of DAPT (1, 6, or 12 months) and P2Y12 inhibitor use (clopidogrel, prasugrel, or ticagrelor), which were prespecified by the investigators before randomization. Group 1 received a three-quarter dose of rivaroxaban (15 mg daily) plus a P2Y12 inhibitor, group 2 received very low dose rivaroxaban (2.5 mg twice daily) plus a P2Y12 inhibitor (which was an established regimen from the ATLAS ACS-TIMI 51 trials12), and group 3 received triple therapy consisting of warfarin plus DAPT (target international normalized ratio 2–3). The primary endpoint was clinically significant bleeding, defined by Thrombolysis in Myocardial Infarction (TIMI) criteria including both major and minor bleeding or bleeding requiring medical attention over 12 months. Secondary efficacy endpoints were MACE and each of its components (cardiovascular death, myocardial infarction, and stroke).
Table 1
Designs of three trials comparing dual vs. triple antithrombotic therapy
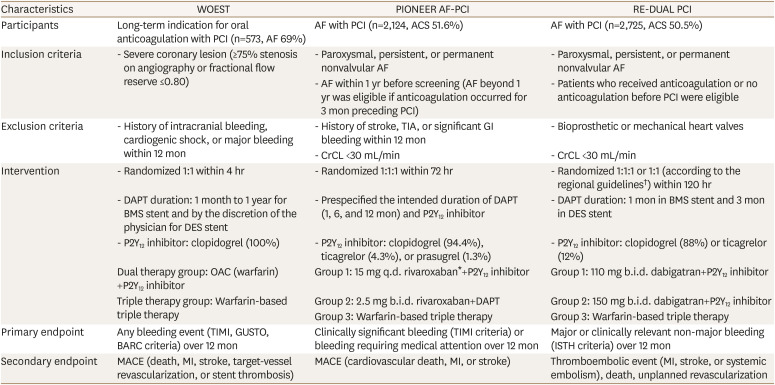
AF, atrial fibrillation; ACS, acute coronary syndrome; BMS, bare metal stent; CrCL, creatinine clearance; DAPT, dual antiplatelet therapy; DES, drug eluting stent; GI, gastrointestinal; MACE, major adverse cardiovascular event; MI, myocardial infarction; OAC, oral anticoagulation; TIA, transient ischemic attack; PCI, percutaneous coronary intervention; q.d., once a day; b.i.d., twice a day; TIMI, Thrombolysis in Myocardial Infarction; GUSTO, Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries; BARC, Bleeding Academic Research Consortium; ISTH, International Society on Thrombosis and Hemostasis.
*Rivaroxaban 10 mg if CrCL <50 mL/min; †Outside the United States, patients older than 80 were assigned to either group 1 or group 3. In Japan, the age cutoff was 70.
The three groups were well-matched and had around 700 patients each, with a mean age of 70 years. More than 90% of the participants received clopidogrel as the P2Y12 inhibitor. In the primary endpoint analysis, a significantly lower risk of bleeding was confirmed in both of the rivaroxaban groups (groups 1 and 2) compared to the triple therapy group (group 3), and clinically significant bleeding events occurred in 16.8%, 18.0%, and 26.7% of patients in groups 1, 2, and 3, respectively, at 12 months: hazard ratio (HR), 0.59 (95% confidence interval [CI], 0.47–0.76, p<0.001) for group 1 vs. group 3; HR, 0.63 (95% CI, 0.50–0.80; p<0.001) for group 2 vs. group 3. Reduced bleeding risk was consistently identified across the major subgroups and the strata of DAPT use duration. Notably, the secondary efficacy endpoints of the three groups were not significantly different between the rivaroxaban groups (groups 1 and 2) and the triple therapy group (group 3): HR, 1.08 (95% CI, 0.69–1.68; p=0.75) for group 1 vs. group 3; HR, 0.93 (95% CI, 0.59–1.48; p=0.76) for group 2 vs. group 3. Similar event rates were observed for each component of the MACE as well as in the multiple subgroups.
Compared to the WOEST trial mentioned earlier, this trial had certain strengths. The PIONEER AF-PCI trial participants were all AF patients, whereas 31% of the participants in the WOEST trial did not have AF and received anticoagulation therapy for other medical conditions.811 Thus, the PIONEER AF-PCI trial was more specific for patients with AF undergoing PCI. Moreover, in the PIONEER AF-PCI trial, only 22% of the participants in the triple therapy group were treated for 1 year.11 Considering that up to 66% of the participants in the triple therapy group in the WOEST trial received triple therapy for 1 year, demonstrating the lower bleeding risk in the PIONEER AF-PCI trial was more difficult.811 The limitation of the study was that it was not powered to test the superiority of the secondary endpoint among the groups. Therefore, it remains unclear whether the 15 mg dose of rivaroxaban sufficiently prevents thromboembolic events, although it is now an available option in the guidelines.131415
In summary of the PIONEER AF-PCI trial for AF patients who underwent PCI, dual antithrombotic therapy with use of either three-quarter dose or very low dose rivaroxaban plus a P2Y12 inhibitor had a significantly lower rate of bleeding events compared to the conventional warfarin-based triple therapy, while the occurrence of MACE was similar among the three groups.
RE-DUAL PCI TRIAL
The RE-DUAL PCI trial was another international, multicenter, randomized, open-label trial that evaluated the safety and efficacy of dual therapy (using dabigatran) compared to triple therapy in nonvalvular AF patients who underwent PCI.16 The summary of the study design is shown in Table 1. The trial was designed to examine whether dual therapy with dabigatran is noninferior to triple therapy. Anticoagulation status, before or after enrollment, did not affect patient eligibility. Briefly, after the participants with AF underwent PCI stenting, they were randomly assigned to one of the following groups: group 1 treated with dabigatran 110 mg twice daily plus a P2Y12 inhibitor (110-mg group); group 2 treated with dabigatran 150 mg twice daily plus a P2Y12 inhibitor (150-mg group); or group 3 treated with warfarin-based triple therapy (triple therapy group). The P2Y12 inhibitor included in this study was either clopidogrel or ticagrelor, and the DAPT duration was 1 month for bare-metal stents and 3 months for drug-eluting stents. Group assignment for the participants was performed according to their countries' guidelines for use of dabigatran. In the United States, all participants were randomized to one of three groups at a 1:1:1 ratio. In the other countries, non-elderly participants were assigned to one of three groups as well, whereas elderly participants were assigned to either the 110-mg group or the triple therapy group at a 1:1 ratio based on regional recommendations. The cutoff age was 80 years, except in Japan, which set the age criterion at 70 years. This randomization resulted in a relatively larger size in group 1 and group 3. The primary endpoint was major or clinically relevant non-major bleeding event defined by International Society on Thrombosis and Hemostasis. The secondary endpoints comprised thromboembolic events (myocardial infarction, death, and unplanned revascularization).
A total of 2,725 patients was randomized. The mean age was 70.8 years, and 88% of participants received clopidogrel as the P2Y12 inhibitor, similar to the PIONEER AF-PCI trial. During the mean follow-up period of 14 months, 15.4% of the 110-mg group experienced the primary endpoint, whereas the incidence in the corresponding triple therapy group was 26.9%: HR, 0.52 (95% CI, 0.42–0.63; p<0.001 for noninferiority). The incidence of the primary endpoint in the 150-mg group was 20.2%, which also showed a significantly lower bleeding risk compared to the triple therapy group: HR, 0.72 (95% CI, 0.58–0.88; p<0.001 for noninferiority). The reduced bleeding risk in the dual therapy group was consistent for most of the other bleeding endpoints, including major or minor bleeding as defined by the TIMI criteria. Comparing the two dual-therapy groups with the triple therapy group, the incidence of thromboembolic events was not significantly different (HR, 1.04; 95% CI, 0.84–1.29; p=0.005 for noninferiority). Moreover, the incidence of thromboembolic events was not significantly different for each of the dual therapy groups vs. the triple therapy group (HR, 1.13; 95% CI, 0.90–1.43; p=0.30 for 110-mg group vs. triple therapy group; HR, 0.89; 95% CI, 0.67–1.19; p=0.44 for 150-mg group vs. triple therapy group).
In summary, the RE-DUAL PCI trial showed that, in patients with AF undergoing PCI, dual antithrombotic therapy with dabigatran was associated with a significantly lower risk of major or clinically relevant non-major bleeding events compared to triple therapy. Of note, in the 110-mg group, the rate of thromboembolic events was not significantly higher than that in the triple therapy group (15.2% vs. 13.4%), whereas that in the 150-mg dual therapy group was not significantly lower (11.8% vs. 12.8%).16 The trial was not powered to compare the thromboembolic endpoints. However, the result suggests that the dose of dabigatran should be determined after careful evaluation of the bleeding and thromboembolic risks for each individual patient.
The RE-DUAL PCI trial had an advantage over the PIONEER AF-PCI trial regarding the use of the standard doses of dabigatran. Although the maximal duration of triple therapy was 3 months, it was still able to demonstrate significantly lower risks. The limitation of the study is that it could not evaluate the efficacy endpoints, which were not initially planned, as in the PIONEER AF-PCI trial.
FUTURE DIRECTION
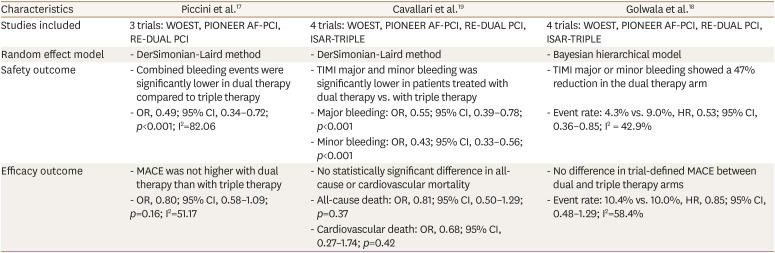
Emerging evidence suggests that, in patients with AF who had undergone PCI, dual therapy with an NOAC is more reasonable than the conventional triple therapy by avoiding excessive bleeding events with similar efficacy. Moreover, meta-analysis of the WOEST, PIONEER AF-PCI, and RE-DUAL PCI trials demonstrated that bleeding risk was significantly lower (odds ratio [OR], 0.49; 95% CI, 0.34–0.72; p<0.001) and incidence of MACE was comparable (OR, 0.80; 95% CI, 0.58–1.09; p=0.16) among the studies, further strengthening the favorable results of dual therapy (Table 2).17 This result was reproduced in other systematic reviews, which further incorporated the results from the ISAR-TRIPLE trial (Table 2).1819
Table 2
Summary of recent meta-analyses
| Characteristics | Piccini et al.17 | Cavallari et al.19 | Golwala et al.18 |
|---|---|---|---|
| Studies included | 3 trials: WOEST, PIONEER AF-PCI, RE-DUAL PCI | 4 trials: WOEST, PIONEER AF-PCI, RE-DUAL PCI, ISAR-TRIPLE | 4 trials: WOEST, PIONEER AF-PCI, RE-DUAL PCI, ISAR-TRIPLE |
| Random effect model | - DerSimonian-Laird method | - DerSimonian-Laird method | - Bayesian hierarchical model |
| Safety outcome | - Combined bleeding events were significantly lower in dual therapy compared to triple therapy | - TIMI major and minor bleeding was significantly lower in patients treated with dual therapy vs. with triple therapy | - TIMI major or minor bleeding showed a 47% reduction in the dual therapy arm |
| - OR, 0.49; 95% CI, 0.34–0.72; p<0.001; I2=82.06 | - Major bleeding: OR, 0.55; 95% CI, 0.39–0.78; p<0.001 | - Event rate: 4.3% vs. 9.0%, HR, 0.53; 95% CI, 0.36–0.85; I2 = 42.9% | |
| - Minor bleeding: OR, 0.43; 95% CI, 0.33–0.56; p<0.001 | |||
| Efficacy outcome | - MACE was not higher with dual therapy than with triple therapy | - No statistically significant difference in all-cause or cardiovascular mortality | - No difference in trial-defined MACE between dual and triple therapy arms |
| - OR, 0.80; 95% CI, 0.58–1.09; p=0.16; I2=51.17 | - All-cause death: OR, 0.81; 95% CI, 0.50–1.29; p=0.37 | - Event rate: 10.4% vs. 10.0%, HR, 0.85; 95% CI, 0.48–1.29; I2=58.4% | |
| - Cardiovascular death: OR, 0.68; 95% CI, 0.27–1.74; p=0.42 |
Supported by the evidence from those studies, recent guidelines now recommend dual therapy with an NOAC as the standard regimen for patients with AF undergoing PCI, whereas triple therapy should be considered only for patients with high ischemic and low bleeding risks.13141520 For dual therapy, an NOAC plus one of the P2Y12 inhibitors is preferred over the regimen with warfarin or aspirin in nonvalvular AF.1520 The 15 mg dose of rivaroxaban, which was adopted in the PIONEER AF-PCI trial, is currently the available option for AF patients who underwent PCI. However, as mentioned earlier, the trial was not powered to compare the efficacy for prevention of thromboembolism. Since the 15 mg dose had not been investigated as a dose for stroke prevention13 except in a small Japanese study21, further trials testing the efficacy of low-dose rivaroxaban for prevention of thromboembolic events may be required.
Upcoming trials will investigate the potential benefits of dual therapy with edoxaban and apixaban (the ENTRUST-AF-PCI trial and the AUGUSTUS trial).2223 In particular, the AUGUSTUS trial has a 2-by-2 factorial design that can simultaneously compare an NOAC vs. warfarin and aspirin vs. no aspirin, and the trial has a much larger population of up to 4,600 patients. The results will specifically elucidate the impact of each of the anticoagulation and antiplatelet agents and also broaden the spectrum of the available NOACs for patients with AF who underwent PCI.
CONCLUSION
The aforementioned two, large, randomized trials demonstrated that dual antithrombotic therapy with either rivaroxaban or dabigatran had a significantly lower risk of bleeding, with similar thromboembolic events, compared to the conventional warfarin-based triple therapy in AF patients with PCI stent insertion. In addition, the upcoming trials should support the benefits of dual therapy as well as widen the available choices of NOAC.
 XML Download
XML Download