

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Dementia is a highly prevalent chronic neuropsychiatric syndrome globally and is accompanied by memory deficit and cognitive dysfunction, which ultimately result in disability or limitations in the activities of daily living.1 The population with dementia is rapidly increasing compared to those having other diseases and, based on a clinical report, the number of individuals with dementia is projected to reach approximately 66 million by 2030.2 Dementia can be commonly classified into 2 types: Alzheimer's disease (AD) and vascular dementia (VaD).3 AD is characterized by an onset with a progressive course with memory loss and visuospatial functions that leads to global cognitive impairment,4 whereas VaD is markedly characterized by vascular changes and its onset is described as being a less gradual progression compared to AD, which involves a step-by-step cognitive decline.5 The neuropathologic features of these diseases include neuronal loss, atrophy of the frontal and temporal lobes, severe memory loss, and language impairments.6 AD is degenerative and incurable, while VaD is reversible or temporary. AD patients mainly have difficulty recalling recent events or new information and have more severe troubles with memory loss and communication than do individuals with VaD. VaD occurs as a result of a lack of adequate oxygen transfer to the brain and ultimately leads to neuronal cell death. One study demonstrated that VaD patients are more impaired than AD patients in the areas of attention and visual construction tasks.7 Also, several studies have suggested that memory function and temporal lobe function are mainly impaired in AD, whereas frontal lobe function impairment is predominant in VaD.8 AD accounts for more than 60% of cases of dementia in older individuals and is characterized by the deposition of extracellular amyloid-β (Aβ) plaques and intracellular neurofibrillary tangles of hyperphosphorylated tau proteins, representing the most frequent type of dementia worldwide.9 The excessive accumulation of senile plagues composed of Aβ peptide and the hyperphosphorylation of tau proteins trigger neuroinflammation, blood–brain barrier (BBB) dysfunction, and cognitive decline.10 VaD is accompanied by cognitive impairment, is the second most prevalent type of dementia, and is attributable to cerebrovascular pathology.11 Cognitive impairment in VaD is directly correlated with the suppression of cerebral blood pressure (BP) and cardiovascular complications,12 leading to an increase of BBB permeability from neurotoxic substances and the increase of amyloid deposition.13 The impairment of cerebrovascular function triggers excessive Aβ deposition and the early opening of the BBB.14
According to previous studies, dementia is also related to metabolic diseases such as hypertension and type 2 diabetes15 as a result of various risk factors related to cognitive decline. With respect to the relationship between dietary pattern(s) and the onset of dementia, many studies to date have investigated therapeutic approaches for preventing dementia using dietary regulation to support diet's positive role in mitigating memory decline in patients with dementia.16 Calorie restriction achieved by altering dietary patterns results in weight loss and ultimately improves metabolic and cognitive function by regulating lipid metabolism and improving glucose metabolism, inflammation, and insulin resistance.17 Previous studies have reported that caloric restriction has demonstrated neuroprotective effects on neuroinflammation and cognitive function.18 In particular, intermittent fasting as a method of dietary caloric restriction has been shown to more effective in reducing weight and fat mass versus continuous calorie restriction.19
Intermittent fasting is not a type of diet but instead is a pattern of eating. Its success more so relies on when one eats rather than what one eats. There are several different methods of intermittent fasting: for example, well-known methods include the Leangains protocol, which involves eating for eight hours and fasting for 16 hours between feedings; the eat-stop-eat protocol, which involves fasting for 24 hours, once a week; and the 5:2 diet, which involves consuming only 500 calories on 2 nonconsecutive days of the week and then normally eating on the other 5 days.20 Intermittent fasting has been highlighted as a promising method of calorie restriction, in that modulation of the circadian cycle can more effectively regulate the function of the hypothalamus, which controls appetite, energy metabolism, and the inflammatory response.21 In addition, intermittent fasting has demonstrated neuroprotective effects, a reduction of neuroinflammation, and an improvement in redox status and promotes an increase in the production of neurotrophic factors, leading to increased neurogenesis and improvement in mitochondrial function.22 Furthermore, intermittent fasting improves cognitive dysfunction and the dysregulation of energy metabolism and dyslipidemia in patients with AD.23 Another study reported that intermittent fasting protected against brain damage by restoring aquaporin-4 polarity in AD,24 while a recent investigation indicated that intermittent fasting leads to increases in ketone body levels in the blood and continuously supports neuroprotective effects by regulating the activity of β-hydroxybutyrate in AD.25 Herein, we review recent evidence regarding the effects of intermittent fasting on dementia and discuss the therapeutic potential of intermittent fasting to prevent the onset of dementia and attenuate neuropathology.
Go to : 
THE EFFECTS OF INTERMITTENT FASTING IN DEMENTIA
1. Intermittent fasting: focus on neuroinflammation
A previous study demonstrated that caloric restriction reduces the production of reactive oxygen species and promotes antioxidant responses such as nuclear factor-erythroid 2 signaling.26 Additionally, calorie restriction reduces DNA damage by attenuating telomere erosion through regulating nuclear factor kappa B in inflammatory signaling and the production of proinflammatory mediator C-reactive proteins.27 In particular, intermittent fasting reduces the levels of proinflammatory cytokines including interleukin (IL)-1β and IL-18 in the brain.27 One study reported that intermittent fasting decreases the production of IL-1α, IL-1β, and tumor necrosis factor-α under lipopolysaccharide-induced inflammatory conditions and increases the production of brain-derived neurotrophic factor in the hippocampus.28 Furthermore, intermittent fasting has been reported to improve cognitive decline by downregulating inflammatory responses.29 Intermittent fasting controls inflammatory pathways and contributes to hippocampal neuronal function, relating to memory,30 and inhibits neuronal cell apoptosis by controlling autophagic flux.31
2. Intermittent fasting: focus on neurotransmitters and synaptic plasticity
Neurotransmitters, including glutamate, are involved in synaptic plasticity and contribute to neuronal circuitry.32 Fasting may activate cAMP responsive element binding signaling in hippocampal and entorhinal cortical neurons involved in synaptic function and memory formation.33 In particular, intermittent fasting boosts hippocampal plasticity and mitochondrial function via calcium signaling.34 Intermittent fasting also contributes to neuronal synaptic plasticity by controlling the secretion of neurotransmitters including serotonin, noradrenaline, and dopamine.35 Intermittent fasting additionally improves the impairment of synaptic plasticity in hippocampal neurons36 and enhances autonomic synaptic plasticity,37 subsequently rescuing cognitive impairment.38
3. Intermittent fasting: focus on vascular function
Cerebrovascular dysfunction is commonly exhibited in patients with dementia.39 It leads to neuroinflammation and oxidative stress in the brain and causes neuronal damage; provokes BBB breakdown; and triggers amyloid plaque production by boosting the amyloid precursor protein (APP) cleavage enzyme, beta-secretase, and tau protein phosphorylation.40 A recent study demonstrated that arterial stiffness (or high-pulse wave velocity) could promote the increase of amyloid beta deposition and exacerbate cognitive decline.41 Additionally, neurovascular coupling is impaired in AD, and abnormal blood flow leads to an imbalance between neural activity and glucose metabolism in the brain.42 Calorie restriction has been reported to decrease the risk for atherosclerosis and reduce BP and triglyceride levels in blood vessels.43 Previous research has demonstrated that intermittent fasting improves endothelial dysfunction and attenuates the risk for cardiovascular diseases.44 Intermittent fasting has been found to improve endothelial vasorelaxation and stabilize high BP.45 A few studies have reported dramatic decreases in BP values after intermittent fasting46 as well as improvement in vascular function.47
4. Intermittent fasting: focus on insulin resistance and neurogenesis
Intermittent fasting leads to a decrease in insulin-like growth factor 1 expression and a consequent reduction in glucose levels.30 Additionally, intermittent fasting enhances insulin sensitivity in neurons and ameliorates dysfunction in glucose metabolism.48 Neurogenesis describes the process where new neurons are generated to replace injured neurons in the subventricular and subgranular zones of the hippocampus.49 In dementia, the process of neurogenesis is impaired and, consequently, cognitive impairment occurs.49 In AD, the excessive accumulation of APP triggers a decrease in neurogenesis in both the dentate gyrus and subventricular zone.50 Intermittent fasting enhances hippocampal neurogenesis51 and reduces brain damage by generating new neurons in response to oxidative stress.52
Go to :
CONCLUSIONS
We reviewed the effects of intermittent fasting on dementia based on previous significant findings. We focused on the therapeutic potential of intermittent fasting in view of known risk factors for dementia, including neuroinflammation, synaptic dysfunction, vascular dysfunction, insulin resistance, and neurogenesis (Fig. 1). A previous study has reported that chronic intermittent fasting improves cognitive dysfunction.53 Another recent study demonstrated that intermittent fasting inhibits hippocampal neuronal damage against oxidative stress and, ultimately, suppresses memory deficits.54 A separate investigation suggested that intermittent fasting ameliorates memory deficits by controlling inflammatory responses.55 However, although there is much evidence available to support the positive effect of intermittent fasting on cognitive decline in dementia, the mechanisms involved in the fasting process and occurrence of memory deficit remains unclear. We reviewed related mechanisms regarding the therapeutic potential of intermittent fasting in dementia. We suggest that the application of intermittent fasting may be an effective dietary therapy for preventing the onset and/or suppressing the development of dementia.
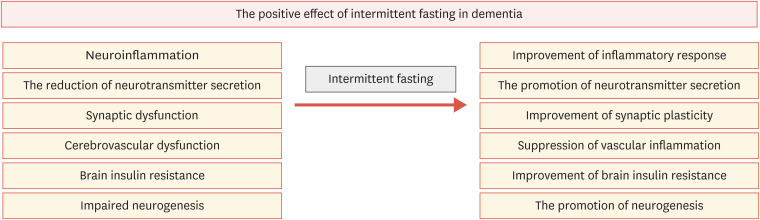 | Fig. 1The positive effects of intermittent fasting in dementia. Pathologies in dementia including neuroinflammation, the abnormal secretion of neurotransmitters, synaptic dysfunction, cerebrovascular inflammation, brain insulin resistance, and impaired neurogenesis were improved by intermittent fasting.
|
Go to :
 XML Download
XML Download