

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Neuroendocrine tumors (NETs) of the gynecological tract are rare tumors that represent approximately 2% of all gynecological malignancies [1]. They are classified into four categories: typical carcinoid, atypical carcinoid, small cell carcinoma and large cell carcinoma [2]. Typical and atypical carcinoids are well-differentiated and typically have a more indolent course. Small and large cell carcinomas are considered high-grade neuroendocrine neoplasms, and are closely related to pulmonary small cell carcinoma which is highly aggressive [3]. The majority of gynecologic NET are small cell carcinomas. Studies of NET in cervical cancer have shown that patients present at earlier age, with greater incidence extra-uterine disease and have an overall worse prognosis compared to squamous cell carcinoma [14]. At the present time, there are no studies examining the outcomes of NET of the uterine corpus. The goal of this study was to compare the clinicopathologic features and survival outcomes of neuroendocrine tumor of the uterine corpus (NET-U) versus endometrioid type endometrial carcinoma (EC).
MATERIALS AND METHODS
Patients with EC and NET-U were identified using the Surveillance, Epidemiology and End Results (SEER) cancer registry database. The SEER database is a population based cancer registry that includes approximately 28% of the US population from 18 population-based cancer registries. International Statistical Classification of Diseases and Related Health Problems, 10th Revision code of C54.1 (malignant neoplasm of the corpus uterus) were used to identify patients with endometrial cancer. We further limited our study to include only those with endometrioid adenocarcinoma and high-grade NET (small and large cell carcinoma) from 1993 to 2012. Patient characteristics including year of diagnosis, age, race, stage, grade, surgery, adjuvant therapy and survival were obtained. Exclusion criteria included benign or in situ neoplasms, and more than one histology type. Chi-square and t-tests were used to compare frequency distribution among categorical and numerical variables, respectively. Kaplan-Meier curves were used to analyze survival outcomes. Analysis was controlled for both stage and age. Pearson-Correlation tests were used to analyze trends in NET. Statistical significance was determined using p<0.05.
RESULTS
From 1993–2012, a total of 99,219 patients were identified. Of this cohort, 98,363 patients had sufficient data for analysis. The 98,245 with EC and 118 with NET-U. The mean age at diagnosis for EC was 61.7 (range: 17–106) years compared to 64.8 (range: 30–97) for NET-U (p=0.01). Majority of patients in both groups were white (86.4% in EC vs. 77.1% in NET-U; p=0.03) (Table 1). We observed significant increase in extrapelvic disease at time of diagnosis in patients with NET-U compared to those with EC, 49.1% vs. 4.8% respectively (odds ratio=18; 95% confidence interval=13.1–27.2; p≤0.01). NET-U cases were more likely to be poorly differentiated when compared to EC (97.0% vs. 15.6%, respectively; p≤0.01). 45.3% of patients with NET-U and 59.0% of patients with EC underwent lymph node dissection. Of these patients, 56.4% with NET-U and 11.1% with EC had nodal metastases (p≤0.01). The overall survival (OS) for patients with NET-U without nodal metastasis was 9.8 compared to 2.4 years in patients with nodal metastasis (p≤0.01) (Table 1).
Table 1
Patient demographics and characteristics
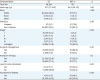
Patients with EC were more likely to receive surgical treatment compared to those with NET-U (95.4% vs. 68.6%, respectively; p≤0.01). Patients with NET-U who received surgical management had an OS of 5.6 compared to 0.9 years in those that did not receive surgical management (p≤0.01). There was no significant difference in adjuvant radiation therapy between the two groups, 22.6% EC vs. 22.9% NET-U (p=0.5). Patients with NET-U who received radiation therapy had an OS of 7.7 years compared to 3.3 years in those that did not receive radiation therapy (p≤0.01). Among the entire cohort, the OS for EC was 14.4 compared to 4.6 years for NET (p≤0.01). The cancer-specific survival for EC was 17.7 compared to 5.7 years for NET (p≤0.01).
DISCUSSION
NET-U is a rare gynecological malignancy. Only 118 patients have been diagnosed during the study time period of 19 years. When compared to EC, NET-U represents a more aggressive malignancy that presents at advanced stage with extrapelvic and nodal disease. These findings likely contribute to the lower OS observed in patients with NET-U regardless of adjuvant therapy. Although there was a significant increase in the number of white patients in the EC cohort compared to NET-U, the majority of both groups were white. These numbers correspond with published literature on EC and on NET. A recent large SEER data base analysis of all NETs reported 79.2% of effected patients were white [5].
Our findings mirror those found in cervical NET, which also demonstrate a worse prognosis compared to their more common squamous cell carcinoma counterpart [678]. Studies show a high rate of lymphatic metastasis in early stage cervical NET. Stage I small-cell carcinoma of the cervix has been found to have lymph node metastasis in up to 40% of cases, approaching 60% in those with lymphovascular space invasion [39]. In contrast to our present findings, the majority of patients with cervical NET are diagnosed at an early stage and younger age [110]. When comparing the rate of lymph node metastasis between cervical NET and NET-U, we observed a similar incidence in the literature [11]. Thus, illustrating the aggressive nature of these tumors regardless of their location in the gynecologic tract.
Current treatment regimens for NET-U are extrapolated from cervical NET which are based on data arising from pulmonary literature, focusing on the use of multimodality therapy including surgery, chemotherapy and radiation [1121314]. A study of cervical large-cell NET showed improved survival with platinum as single agent and when given in combination with etoposide [10]. Our study does show improved outcomes in patients with NET-U who received adjuvant radiation. Those treated with radiation showed improved OS compared to those who did not, 7.7 versus 3.3 years. We also observed improved survival in patients with NET-U who underwent surgical management (OS: 5.6 compared to 0.95 years). The limited data available on NET-U shows that surgical resection followed by combination chemotherapy with cisplatin and etoposide, plus radiation has variable levels of response [151617]. Although we cannot draw conclusions regarding chemotherapy based on the current study, our results do indicate there is a role for surgical resection and radiation in the treatment of NET-U.
Prior to our study, only 80 cases of NET-U have been published in the literature. However, there is a recent increase in the incidence of NET reported [1819]. The reason for this uptrend is possibly due to increasing recognition and diagnostic accuracy, rather than a true increase incidence. This increase has been observed in cervical NET as well as gastro-entero-pancreatic NET [20]. With this recent increase in NET across difference cancers, we expect a parallel increase in NET-U.
To our knowledge, this is the largest review of NET-U to date, and the first report to examine the clinicopathologic features in comparison to EC. The major limitation of our study is its retrospective nature. Furthermore, the SEER database only encompasses approximately 28% of the United States population and does not include chemotherapy data. Despite these limitations, the present study demonstrates aggressive nature of NET-U compared to EC. Highlighted by the significantly lower OS observed in NET-U compared to stage equivalent EC. The present study suggests that surgery and radiation offer improved survival and are a potential platform for prospective research. Additionally, platinum-based chemotherapy has shown benefit in other neuroendocrine malignancies of the gynecologic tract and warrants further investigation along with targeted agents in NET-U.
 XML Download
XML Download