

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Endometrial cancer (EC) is the most common gynecological cancer in developed countries with an incidence in 2012 in Europe at 13.6 per 100,000 patients [1] and a 5-years overall survival (OS) of 95% for patients diagnosed at an early stage [23]. In Europe, standard treatments for early-stage EC consist of primary hysterectomy and bilateral salpingo-oophorectomy. Pelvic and para-aortic lymphadenectomy is recommended for patients of high-risk EC [4].
Adjuvant treatment, including vaginal brachytherapy (VB), external beam radiotherapy (EBRT) or chemotherapy, is based on post-operative analysis. In 2016, the European Society of Medical Oncology, European Society of Gynaecological Oncology and European Society of Radiotherapy and Oncology (ESMO-ESGO-ESTRO) established new guidelines for adjuvant treatment following the new post-operative classification [4]: patients can be classified as having early-stage EC at low, intermediate risk (IR), high-intermediate risk (HIR) or high-risk for recurrence by means of a combination of postoperative histological criteria (i.e., depth of myometrial invasion, histological type, grade and lymphovascular space invasion (LVSI) status) [4].
In this specific setting, VB which is usually performed to prevent local recurrence [5] is no more recommended in patients with low-risk EC and is optional in patients with IR and HIR EC, especially when lymph node sampling showed no lymph node metastases involvement. Furthermore, in patients with HIR EC with no lymphadenectomy performed, EBRT is recommended in case of LVSI positive status and VB is recommended in case of LVSI negative status. Thus, additional studies are needed to improve the selection of patients with IR and HIR EC for adjuvant VB.
Hence, the aim of this French retrospective, multicenter study was to assess the impact of VB in IR and HIR EC on local recurrence, local recurrence-free survival (RFS) and OS.
MATERIALS AND METHODS
1. Study population
Data of all patients who received primary surgical treatment between January 2000 and December 2016 were abstracted from 9 institutions in France (FRANCOGYN research group) with maintained EC databases (La Pitié-Salpêtrière University Hospital, Tenon University Hospital, Reims University Hospital, Dijon Cancer Center, Lille University Hospital, Creteil University Hospital, Bichat Hospital, Rennes University Hospital and Tours University Hospital), and also from the SENTI-ENDO trial [6]. The research protocol was approved by the Institutional Review Board of the French College of Obstetrics and Gynecology (CEROG 2014-GYN-020).
Clinical and pathological variables included patients age, comorbidities (body mass index, diabetes, health technology assessment), surgical procedure, 2009 International Federation of Gynecology and Obstetrics (FIGO)'s stage, final pathological analysis (histological type and grade, depth of myometrial invasion, LVSI status) and adjuvant VB.
Histological staging and grading were performed according to the 2009 FIGO classification system based on the final evaluation of the pathological specimen. The risk of recurrence was defined according to the ESMO-ESGO-ESTRO guidelines. Histological type I corresponds to endometrioid EC, whatever the histological grade. The four risk groups of EC are defined as follow: low-risk (type 1 EC FIGO stage IA grade 1 or 2 without LVSI); IR (type 1 EC FIGO stage IB grade 1 or 2 without LVSI); HIR (type 1 EC, FIGO stage IA grade 3 with or without LVSI and FIGO IA–IB, grade 1 or 2, with LVSI), high-risk (type 1 EC, FIGO stage IB grade 3, with or without LVSI) [4].
All patients with IR and HIR EC were included. Patients who received treatment other than VB and patients with lack of survival data were excluded from our analysis.
2. Treatment and follow-up
All patients underwent primary surgery, including at least total hysterectomy with bilateral salpingo-oophorectomy. Adjuvant VB was administered according to multidisciplinary committee's opinion based on French guidelines [7]. All the recruiting centers are referent in EC management and applied admitted guidelines for VB modalities. Currently, for post-operative VB, the 5 mm deep prescription regimens used in high dose rate are: 21 Gy in three fractions (Deq2 Gy=29.8 Gy), 20 Gy in four fractions (Deq2 Gy=25 Gy), 24 Gy in four fractions (Deq2 Gy=32 Gy). Doses at the level of risk organs not to be exceeded are D2cm3eq2 Gy=75 Gy for the rectum and sigmoid and D2cm3eq2 Gy=8 5Gy for the bladder. No imaging exam is needed before planning postoperative VB applications of the vaginal vault and the recommended techniques use a high dose rate planned on two-dimensional imaging [8].
According to French guidelines, frequency of clinical follow-up was every four months for the first two years, and then every six months until five years and every year thereafter. Further imaging investigations were carried out if clinically indicated [7].
Disease recurrence was diagnosed either by biopsy or imaging studies and defined as a relapse without differentiating between their local or distant nature. RFS was calculated in months from the date of surgery to recurrence. In this study, the outcome was local recurrence defined by vaginal and pelvic recurrence.
3. Statistical analysis
Statistical analysis was based on the Student's t-test or analysis of variance test, as appropriate, for continuous variables, and the χ2 test or Fisher's exact test, as appropriate, for categorical variables. The Kaplan-Meier method was used to estimate the survival distribution, and comparisons of survival were made using the log-rank test. The Cox proportional hazards model was used to account for the influence of multiple variables. Values of p<0.05 were considered to denote significant differences.
Data were managed with an Excel database (Microsoft Corporation, Redmond, WA, USA) and analyzed using R 3.0.1 software (R Foundation, Vienna, Austria), available online.
RESULTS
1. Study population
A total of 429 patients with IR EC and 365 HIR EC were documented as having received primary surgical treatment. Among them, 138 were treated differently than by VB alone or simple follow-up and were excluded. Among the 138 patients excluded, 83 patients received VB and chemotherapy, 10 VB and external radiotherapy, 6 VB, external radiotherapy and chemotherapy, 2 chemotherapy only, 26 external radiotherapy only and 6 radiotherapy and chemotherapy. Data was lacking for 5 patients.
Finally, survival data were available for 191 patients (135 with adjuvant VB alone and 56 with no adjuvant therapy), according to the following distribution: La Pitié-Salpêtrière University Hospital (n=42; 22%), Tenon University Hospital (n=16; 8%), Reims University Hospital (n=13; 7%), Dijon Cancer Center (n=23; 12%), Lille University Hospital (n=26; 14%), Creteil University Hospital (n=12; 6%), Bichat Hospital (n=5; 3%), Rennes University Hospital (n=15; 8%), Tours University Hospital (n=25; 13%), and the SENTI-ENDO trial [6] (n=14; 7%). Flow-chart of the study is reported in Fig. 1.

Patients with IR EC and HIR EC received adjuvant VB in 79% (n=92) and 59% (n=43), respectively (p=0.01).
2. Characteristics according to ESMO-ESGO-ESTRO risk-group
The demographic, clinicopathological and surgical characteristics of IR and HIR EC patients according to adjuvant management (VB vs. no adjuvant therapy) are reported in Table 1. There was no difference between the two groups regarding other demographic, clinicopathological and surgical characteristics.
Table 1
Epidemiological, histological and surgical characteristics

Values are presented as median (IQR) or number (%). Student's t-test or analysis of variance test, as appropriate, for continuous variables, and the χ2 test or Fisher's exact test, as appropriate, for categorical variables.
BMI, body mass index; HIR, high-intermediate risk; HBP, high blood pressure; IR, intermediate risk; IQR, interquartile range; LVSI, lymphovascular space invasion; VB, vaginal brachytherapy.
![]()
3. Local recurrence rate
Local recurrence rates in patients with adjuvant VB or no adjuvant therapy are presented in Table 2. In the overall population, there were nine patients presenting with local recurrences: eight patients with isolated local recurrence and one patient with simultaneous local, nodal and distant metastasis.
Table 2
Local recurrence

Values are presented as number (%). The χ2 test or Fisher's exact test, as appropriate, for categorical variables.
HIR, high-intermediate risk; IR, intermediate risk; LVSI, lymphovascular space invasion; VB, vaginal brachytherapy.
*p-value <0.05.
![]()
With a median follow-up of 22 months (interquartile range [IQR]=8–41), 9 patients (4.7%) experienced a local recurrence. In HIR group, VB was correlated with a lower local recurrence rates (0% vs. 16.7%, respectively; p=0.02). In IR group, VB and no adjuvant therapy were associated with similar local recurrence rates (3.2% vs. 4.2%, respectively; p=1.00).
If we focus on patients with positive LVSI status, VB reduces the rate of local recurrence from 21% to 0% (p<0.05).
In the HIR group, among the patients over 60 years old, the local recurrence rate increased from 0% in the VB group to 21.7% in the no adjuvant therapy group (p=0.01). In the IR group, among the patients over 60 years old, these results were not statistically significant (p=0.48).
4. OS and local RFS
In IR and HIR groups, VB was not associated with a better OS compared to no adjuvant therapy (Fig. 2A-C). In univariate analysis, none of the parameters included was statistically associated with OS (Table 3).
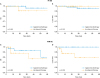 | Fig. 2OS and local RFS according to adjuvant therapy subgroup in IR EC (A, B) and in HIR EC (C, D).EC, endometrial cancer; HIR, high-intermediate risk; IR, intermediate risk; OS, overall survival; RFS, recurrence-free survival.
|
Table 3
OS: univariate analysis

The Kaplan-Meier method was used to estimate the survival distribution, and comparisons of survival were made using the log-rank test. The Cox proportional hazards model was used to account for the influence of multiple variables.
BMI, body mass index; HBP, high blood pressure; HIR, high-intermediate risk; HR, hazard ratio; IR, intermediate risk; IQR, interquartile range; LVSI, lymphovascular space invasion; NA, not applicable; OS, overall survival.
![]()
In univariate analysis, brachytherapy was statistically associated with RFS in HIR group (Table 4). In HIR group, VB was associated with a better local RFS (Fig. 2D) (p=0.01), but not in IR group (Fig. 2B) (p=0.55).
Table 4
Local RFS: univariate analysis

The Kaplan-Meier method was used to estimate the survival distribution, and comparisons of survival were made using the log-rank test. The Cox proportional hazards model was used to account for the influence of multiple variables.
BMI, body mass index; HBP, high blood pressure; HIR, high-intermediate risk; HR, hazard ratio; IR, intermediate risk; IQR, interquartile range; LVSI, lymphovascular space invasion; NA, not applicable; RFS, recurrence-free survival.
*p-value<0.05.
![]()
DISCUSSION
We report the results of the first study assessing the impact of VB as adjuvant therapy on local recurrence in IR and HIR EC based on recent ESMO-ESGO-ESTRO recommendations [4]. Our data suggest that VB is significantly associated with a better local RFS in the HIR group, but not in the IR group.
Several recent studies have shown that patients with EC have specific recurrence patterns according to their ESMO-ESGO-ESTRO group of risk [591011]. In their study, Bendifallah et al. [11] stated that patterns of recurrence in EC differ widely in terms of localization and timing depending on the risk subgroup. Overall recurrence rate differed between HIR group (16%) and IR group (9%) (p<0.01). Nevertheless, in this study, vaginal vault and central pelvic recurrence concerned only 1% of patient in IR group and 3% in the HIR group whatever the adjuvant therapy undertaken, confirming that local recurrence is rare and justifying the current debate in national [812] and international [4] recommendations concerning the indication of VB in those populations.
In French recommendations published in 2017, VB is recommended in IR group to reduce vaginal vault recurrence [12]. Our results do not support this proposition as we did not observe any improvement of RFS or OS in this group of patients when undertaking VB. The very low rate of local recurrence in IR EC is consistent with histological findings that define IR, in particular the absence of LVSI. Thus, in the light of our results we may do not recommend VB in this population of patients.
On the contrary, considering HIR group, we found a 6.8% local recurrence rate, in agreement with published results [5]. We observed that VB reduces local recurrence rate in this population (0% in the VB group vs. 16.7% in the no adjuvant therapy group, p=0.02) and improves local RFS. Thus, our data support the use of VB as an effective adjuvant therapy in HIR population to reduce local recurrence rate.
It has now been well established that the presence of LVSI positive status and a grade 3 tumor are risk factors for local and distant recurrence [13141516171819]. Furthermore, a positive LVSI status is associated with a high rate of para-aortic lymph node metastases [1720]. Thus, the main contribution of the ESMO-ESGO-ESTRO 2016 classification is the inclusion of positive LVSI status which leads to reclassify the low risk and RI groups into HIR group. In the present study, 26.9% of patients had a positive LVSI status, and therefore were classified in the HIR population. In the HIR population, there was no statistically significant difference concerning the LVSI status (higher than 70% in both groups) and VB reduces the local recurrence probability from 16.7% to 0%. Furthermore, considering patient with positive LVSI status, VB reduces the rate of local recurrence from 21% to 0% (p<0.05).
According to the ESMO-ESGO-ESTRO 2016 recommendations, it is specified that in the IR and HIR groups, it is possible to perform no adjuvant treatment, especially in patients under 60 years of age [4]. Moreover, the pejorative impact of age is not modified by the therapies used [2122]. Our data could be used to refine adjuvant VB indications for patients carrying a HIR EC and older than 60, as in the HIR group, among the patients over 60 years old, the local recurrence rate increased from 0% in the VB group to 21.7% in the no adjuvant therapy group (p=0.01).
Studies have been conducted to evaluate the purpose of EBRT as adjuvant therapy for IR EC [2324252627]. These studies have demonstrated a decrease in local recurrence rate after EBRT. However, the results were not different when comparing VB vs. EBRT on reducing the risk of local RFS and OS [2728]. EBRT alters the quality of life and is a source of intestinal and urinary toxicity, unlike VB alone [2829]. Regarding the quality of sexual life, it has been observed the same results with a more deleterious effect of EBRT compared to VB [30]. In the same way, it has been stated that general quality of life and sexuality are equivalent after surgery by hysterectomy and bilateral salpingo-oophorectomy alone or in combination with VB in EC [3132]. HIR and IR groups present a risk of local recurrence but also a risk of nodal recurrence [18]. The indication of EBRT can therefore be retained in patients who have not benefited of pelvic lymph node dissection, especially in the presence of LVSI. However, in front of our results, we could offer for these patients instead of a pelvic EBRT alone, deleterious for their quality of life, a combination of VB and EBRT with limited field of pelvic irradiation to node areas to decrease the side effects of EBRT. In this context, intensity modulated radiotherapy could allow to reduce side effects of irradiation in comparison with the association VB-EBRT [33]. Furthermore, European recommendations no longer recommend external irradiation after pelvic lymph node dissection if negative and in the case of positive LVSI status [4]. On the contrary, the French recommendations recommend a pelvic irradiation in this context [8]. The proposal of no adjuvant therapy as an option in LVSI positive patients in European recommendation may be considered as insufficient, while VB is well tolerated and may decreased the rate of local RFS. Furthermore, local pelvic recurrence is not easy to manage and may impact survival.
Some limitations of the present study deserve to be underlined. First, the retrospective nature of the study may be responsible for bias. Second, there is the no precise data concerning VB protocol undertaken in the different centers and the modifications that could occur in this protocol along the period of inclusion (number of sessions, dose delivered, and technique used). Third, we do not have data on treatment-related toxicity. Some studies have shown that VB have side effects and reduces quality of life and sexual quality of life [303132]. Finally, a small number of patients and a relatively short follow-up period make it difficult to draw clear conclusions from this study.
In conclusion, this is the first study evaluating the impact of VB on local recurrence in IR and HIR EC groups. The present study concludes that VB is an efficient adjuvant treatment for patients with HIR EC, with a decrease in the local recurrence rate and an improvement of the RFS. However, VB is not associated with an improvement of RFS or OS in IR EC patient. A prospective randomized study should be undertaken to confirm those results.
 XML Download
XML Download