

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cervical cancer is the fourth most commonly diagnosed cancer in females worldwide [1]. In Korea, it was the fifth most common female cancer and the third most common cancer among 15–34-year-old women [2]. Oncogenic human papillomavirus (HPV) infection is a major risk factor for cervical cancer. The overall prevalence of high-risk human papillomavirus (HR-HPV) increases from 12% in normal cytology to 89% in cervical cancer [3]. Globally, HPV 16/18 are the 2 most common genotypes in approximately 70% of invasive cervical cancer cases [4]. The remaining 30% are caused by other HR-HPV types. HPV infections are common among young women and most spontaneously clear within 1–2 years [5]. Persistent infection with HR-HPV is considered essential for the development of cervical cancer [6]. However, the trend of persistent infection differed by HPV genotype and age. The most persistent types are 16, 31, 33, and 52 and the least persistent types are 35, 51, 66, and 68 [7]. The association between age and persistent infection is inconsistent. Previous studies suggested that women over 30 years of age have a higher rate of persistent HPV infection than women under 30 years of age [78]. Other studies showed that the persistence of HPV infection was not related to age [910].
In addition, HPV type-specific prevalence is different between low-grade squamous intraepithelial lesion (LSIL) and malignancy. HPV 16, 18, and 45 are more frequent in invasive cervical cancer than in any other grade of cervical disease, whereas HPV 51, 52, and 31 are more frequently detected in precancerous lesions than in invasive cervical cancer [11]. However, the risk of individual HPV type and the pattern of age-specific prevalence in cervical carcinogenesis are still not fully understood. A clear understanding of the individual risk according to HPV genotype would provide basic data for the prediction of vaccine effects and the clinical use of cervical cancer prevention. Thus, we performed this study to evaluate the genotype-specific risk for cervical carcinogenesis and the distribution of HPV types according to age in different cervical lesions.
MATERIALS AND METHODS
1. Study population
This study was a retrospective case-control analysis after Institutional Review Board approval (approval No. CGH-IRB-2016-48). Study samples were collected from HPV-positive women who underwent cervical biopsy between July 2011 and December 2017 at the Department of Obstetrics and Gynecology, Cheil General Hospital and Women's Healthcare Center, Dankook University College of Medicine. A total of 1,988 samples were collected from women with normal (n=400), cervical intraepithelial neoplasia (CIN) 1 (n=399), CIN 2 (n=400), CIN 3 (n=400), cervical cancer (n=399). According to a large meta-analysis and a Korean HPV cohort study the prevalence of the 5 most common HR-HPVs was 7.2%–18.7% in LSIL [1213]. Therefore 400 samples per disease grade are required to make up at least 30 cases for the five most common HR-HPVs that is needed to be statistically analyzed. Women were screened by cervical cytology and HPV test prior to biopsies. The women with abnormal cervical cytology and/or HR-HPV underwent a cervical biopsy. The pathologic result of chronic inflammation was included in the normal group. The inclusion criteria of this analysis were evidence of HPV infection and biopsy result. Women with previous hysterectomy were excluded from the analysis.
2. HPV DNA testing
The cervical samples were analyzed for HPV genotype using a Cheil HPV DNA chip kit (Cheil General Hospital, Seoul, Korea). HPV genotyping was based on a SYBR Green real-time polymerase chain reaction (RT-PCR) method. RT-PCR for HPV DNA was performed using the Light Cycler 480 (Roche Diagnostics, Rotkreuz, Switzerland). Post-amplification SYBR Green RT-PCR products were mixed with the hybridization buffer, and the mixture was incubated on the Cheil HPV DNA Chip. A total of 36 HPV types were identified using a chip scanner (NimbleGen MS 200; Roche NimbleGen, Vienna, Austria) and analyzed with GenePix® Pro 6.0 software (Axon Instruments, Union, CA, USA). The 36 HPV genotypes included 19 high-risk types (16, 18, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 67, 68a, 68b, 69, and 82) and 17 low-risk types (6, 11, 30, 32, 40, 42, 43, 44, 54, 55, 62, 70, 72, 81, 84, 90, and 91).
3. Statistical analysis
The data were analyzed using SPSS version 21.0 (SPSS Inc., Chicago, IL, USA). Categorical variables were indicated as numbers and percentages. To assess the risk of severe disease associated with HPV genotype, the odds ratio (OR) with 95% confidence interval (CI) was estimated using the χ2 test. All p-values <0.05 were considered statistically significant.
RESULTS
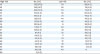
Among a total of 1,988 patients, normal, CIN 1, CIN 2, CIN 3, and cancer cases accounted for 400, 399, 400, 400, and 389, respectively (Table 1). The overall prevalence of HR-HPV infection was 97.4%. The rate of single HR-HPV infection in the cancer group (92.2%) was higher than that in the other groups (67.3%–77.9%). Multiple HR-HPV infection was more frequent in normal and CIN 1/2/3 cases. Except in cervical cancer, multiple HR-HPV infection was more frequent in women <30 years old.
Table 1
Rate of HPV infection and age distributions in study samples

Values are presented as number of patients (%) or mean ± standard deviation.
HPV, human papillomavirus; HR, high-risk; LR, low-risk.
![]()
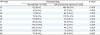
The prevalence of HPV genotype is summarized in Table 2. The 10 most common HR-HPV types were 16 (27.8%), 52 (16.7%), 58 (12.2%), 53 (9.3%), 51 (9.1%), 56 (7.7%), 68 (6.8%), 18 (6.0%), 39 (5.7%), and 31 (5.2%). Genotype-specific HPV infection varied according to the different grades of disease (Fig. 1). The most common HR-HPV genotypes identified were 16 (64.3%), 58 (8.7%), 33 (6.4%), 31 (5.9%), 18 (5.4%), and 52 (5.1%) in cervical cancer; 16 (44.5%), 52 (20%), 31 (10.8%), 58 (8.7%), and 68 (6.3%) in CIN 3; 52 (24%), 58 (19%), 16 (15%), 51 (15%), and 53 (9%) in CIN 2; 52 (17%), 53 (16%), 56 (16%), 51 (12%), and 39 (11%) in CIN 1; and 52 (17%), 53 (14%), 51 (12%), 56(12%), and 38 (11%) in normal cases.
Table 2
Prevalence of HPV genotypes (n=1,988)
![]()
 | Fig. 1Genotype-specific prevalence of HR-HPV in different cervical disease grades.CIN, cervical intraepithelial neoplasia; HR-HPV, high-risk human papillomavirus.
|
The distribution of HR-HPV according to age is shown in Fig. 2. Three HPV genotypes (16, 52, and 58) were most common in all age groups (≤30 years, n=799; 31–40 years, n=502; ≥41 years, n=653). In addition to HPV 16, 52, and 58, common types were HPV 51 and 53 in those aged ≤30 years; 53 and 68 in those aged 31–40 years; and 18 and 56 in those aged ≥41 years. The prevalence of HR-HPV was analyzed according to age and disease grade (Fig. 3). The genotypes showed a similar distribution according to disease grade regardless of age. The most common type was HPV 16 in cervical cancer and CIN 3. Young women with cervical cancer had fewer HPV types than older women. Only 3 types of HR-HPV, 16/31/52 were associated with cervical cancer in women ≤30 years of age. In all age groups, common HR-HPV types in CIN 2 and CIN 1 were 52/58 and 52/53/56, respectively.
 | Fig. 2Genotype-specific distribution of HR-HPV according to age.HPV, human papillomavirus; HR-HPV, high-risk human papillomavirus.
|
 | Fig. 3Prevalence of HR-HPV according to age and disease grades.CIN, cervical intraepithelial neoplasia; HPV, human papillomavirus; HR-HPV, high-risk human papillomavirus.
|
However, the distribution of genotype-specific HPV according to the severity of cervical lesions showed significant differences (Table 3). HPV 16, 31, 33, and 58 were significantly more common in the CIN 2/3/cancer group than in the normal/CIN 1 group. Conversely, HPV 39, 51, 53, 56, 66, and 68 were significantly more common in the normal/CIN 1 group than in the high-grade disease group (p<0.001).
Table 3
Genotype-specific HPVs according to the severity of cervical lesions
![]()
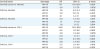
The genotype-specific risks in the CIN 2/3/cancer group in comparison to those in the normal/CIN 1 group are shown in Table 4. Compared with the normal group, genotype-specific risk for cancer was found with HPV 16 (OR=17.1; CI=11.6–22.5; p<0.001) and HPV 33 (OR=3.4; CI=1.5–7.6; p=0.002). HPV 16, 31, and 33 were associated with high risk for CIN 3. HPV 58, 16, and 52 were associated with high risk for CIN 2. In contrast to CIN 1, a significantly high risk of cancer was associated with HPV 16 (OR=24.8; CI=15.9–38.6; p<0.001), 31 (OR=6.2; CI=2.1–18.1; p<0.001), and 33 (OR=3.0; CI=1.5–6.6; p=0.005). HPV 16, 31, and 33 were associated with a high risk for CIN 3. HPV 31 and 16 were associated with a high risk for CIN 2.
Table 4
HPV genotype-specific risks of CIN 2/3/Cancer compared with normal/CIN 1
![]()
DISCUSSION
This study analyzed the genotype-specific risk for the spectrum of cervical carcinogenesis and investigated genotype-specific age distribution for different grades of cervical disease. Although the distributions of HPV infections are different according to geographical region, our results are in agreement with previous studies, with a point prevalence of HPV 16 [314]. HPV 16 was the most common type, especially in CIN 3 and cervical cancer. HPV 52, 58, 53, and 51 followed HPV 16 in the top 5. HPV 18 (6.0%) and 45 (1.8%) were not common in this study, consistent with the less common types in East Asia [15]. HPV genotypes 16, 52, and 58 were the most common in all age groups according to cervical disease grade. The prevalence of multiple infections was approximately 30% in this study. Multiple HR-HPV infections were more frequent in precancerous lesion and more common in women <30 years old. Several previous studies reported a multiple infection rate of 20%–40% [1617]. Multiple infections present more frequent in younger women with high-grade CIN and the infection rate decline with increasing age [11]. The potential significance of multiple infections is their common presence in young women and women with multiple sexual partners, and in specimens with abnormal cytology [1618].
HPV 16/31/33/58 types were more frequently detected in women with high-grade CIN and cervical cancer, whereas HPV 39/51/53/56/66/68 were more frequently detected in women with normal and low-grade CIN. Several HR-HPV types (HPV 53/56/51/39/66/68) were prominent in low-grade CIN but disappeared in high-grade CIN and cancer. The results suggest that there is genotype-specific risk of HR-HPV developing into high-grade CIN and cancer by causing persistent infection. Indeed, these HR-HPV types belong to alpha-9 species (HPV 16/31/33/35/52/58/67) and are likely to have biological properties similar to those of HPV 16 [19]. HPV types in the alpha-9 species are more persistent and more likely to progress to CIN 3 or worse, compared with HPV types in the alpha-5 (HPV 51), 6 (HPV 53/56/66) and 7 (HPV 18/39/45/59/68) groups [20].
This study estimated genotype-specific risks. HPV 16, 31, and 33 were associated with higher risk of CIN 2/3 and cervical cancer compared with normal and CIN 1 cases. HPV 52 and 58 were only associated with higher risk for CIN 2 compared with the normal group. The results showed that relative carcinogenic potential varied. HPV 16/31/33 infection may be a consistent and strong risk for carcinogenesis. Carcinogenic risk of HPV 31 and 33 has been reported [72122]. A 12-year follow-up study in Denmark showed that the absolute risk of CIN 3 or worse among those infected with HPV 31 was 14.3% (CI=9.1–19.4), with 14.9% for HPV 33 (CI=7.9– 21.1) [20]. HPV 52 and 58 are among the 5 most common types associated with cervical cancer in Eastern and Southeastern Asia [131423]. In this study, overall prevalence of HPV 52 and 58 infections was more common than HPV 31/33 infection (28.9% vs 9.3%). Therefore, the prevention of HPV 52 and 58 infections is important to reduce the burden of precancerous cervical disease.
Most HPV infections are self-regulated for one to 2 years, and development of cervical cancer may take a long time even in patients with persistent HPV infection. This study is not a prospective study with repeated HPV results in the same patient so that actual progression from normal to cervical cancer for individual HPV types may be an indirect consideration. However, this study has strengths that relatively large sample size including all grades of disease in the cervical carcinogenesis. The cases of each disease group are well balanced. The results of our study provide important information regarding difference in the CIN2/3/cancer and normal/CIN1 prevalence of individual HPV types and different distribution of HR-HPV according to age. The results can be helpful for individualized management with HPV genotype-based screening.
Our study indicates that HPV 16, 31, 33, 52, and 58 infections are associated with significant risk of high-grade disease and might play important roles in the development of cervical cancer. Fortunately, these oncogenic HPV infections can be prevented by vaccination. The quadrivalent and bivalent HPV vaccines prevent precancerous lesions related to HR-HPV 16 and 18 [2425]. Recently, a nonavalent vaccine became available to protect against HR-HPV 31, 33, 45, 52, and 58, in addition to HPV 16 and 18 [26]. Our data will be useful in the assessment of effectiveness of HPV vaccination and will provide additional information on the risk of developing cervical cancer in HPV infected women.
 XML Download
XML Download