

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The thoracolumbar segment is the most commonly injured part of the spine. Vertebral fractures usually develop at T11-L2 (50–60%), most frequently caused by high-energy blunt trauma and in men between 20 and 40 years of age (12). Neurological injury complicates 20–36% of thoracolumbar fractures (34).
Classically, plain radiographic evaluation including anteroposterior and lateral radiographs is carried out first for assessment of the thoracolumbar spine, with advantages of low cost and availability (5). However, about 25% of burst fractures are misdiagnosed as simple compression fractures when only plain radiography is used (6). Computed tomography (CT) depicts more detailed injury characteristics, such as the type of fracture or the extent of central canal compromise (78). Magnetic resonance imaging (MRI) clearly demonstrates soft tissue injuries—for example, those involving ligaments (9) as well as bone marrow (10)—without radiation exposure. MRI may be performed immediately and is particularly beneficial for in patients with neurologic deficits. However, MRI requires earnest patient cooperation and is associated with long scan times and high costs.
The need for standardized, evidence-based clinical guidelines, including recommendations for initial screening imaging, was proposed for the diagnosis of traumatic thoracolumbar spine injury in adults. The Korean Society of Radiology (KSR) and the National Evidence-based Healthcare Collaborating Agency (NECA) organized the development committee and the working group to develop these guidelines (11).
Go to : 
Development of Korean Clinical Imaging Guidelines for Traumatic Thoracolumbar Spine Injury
Committee Composition
The guideline development process was performed via a collaboration of the NECA and the KSR. The NECA is the national research agency, which was inaugurated to provide evidence-based information about medical devices, medicines, and health technology through objective and reliable analysis. The development committee and the working group were mobilized for guideline development. The development committee was composed of medical imaging experts, research methodology specialists, and clinical guideline specialists who supported the overall planning and research methodology. They published an article detailing the methods involved in the guideline adaptation process for diagnostic imaging (11). The working group was composed of expert members of the Korean Society of Musculoskeletal Radiology (KSMR). The KSMR is an organization of radiologists in Korea and a subspecialty society of the KSR, which is primarily involved in the diagnosis and non-surgical treatment of musculoskeletal disorders.
Guideline Adaptation Process
The guideline development process was performed using an adaptation methodology for Korean Clinical Imaging Guidelines (K-CIGs) established by the development committee (11).
Defining the Key Question
The key question selected by the working group was reviewed by the development committee and a consensus group composed of clinical experts who were end-users and referrers-individuals performing clinical imaging tests. The key question was:
What is the primary imaging test for diagnosis in patients with suspected traumatic thoracolumbar spine injury?
Guideline Search
A systematic guideline search was performed using international databases, including Ovid-MEDLINE, Ovid-EMBASE, National Guideline Clearinghouse, Guideline International Network, and major Korean databases, including KoreaMed, KMBASE, and Korean Medical Guidelines and information published up to March 2017. Additionally, the websites of major academic societies and institutions were searched, and hand searching was carried out.
Selection of Searched Guidelines
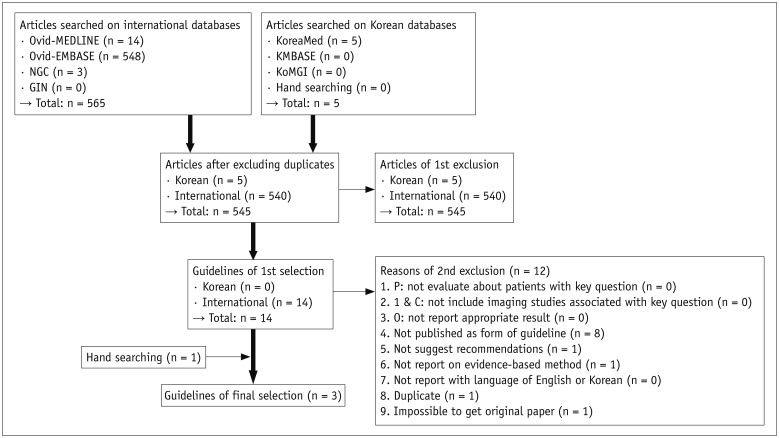
Guideline selection was performed independently based on predefined inclusion and exclusion criteria, in pairs. Articles reporting the conduct and findings of 570 studies addressed the key question, and 545 studies remained after exclusion of duplicates. Fourteen articles remained after screening the titles and abstracts, and one article was added by hand searching. Among these 15 articles, 12 articles were excluded, and three guidelines were selected after on full-text review (Fig. 1).
Quality Appraisal of the Guidelines
The final selected guidelines underwent a quality appraisal process using the Korean Appraisal of Guidelines for Research & Evaluation II tool (12), developed by the guideline development committee (Table 1). Guidelines with a score less than 50 in the “Rigor of Development” domain were not recommended by the development committee. All three guidelines met this condition, and they were selected as relevant to the key question after the quality appraisal process.
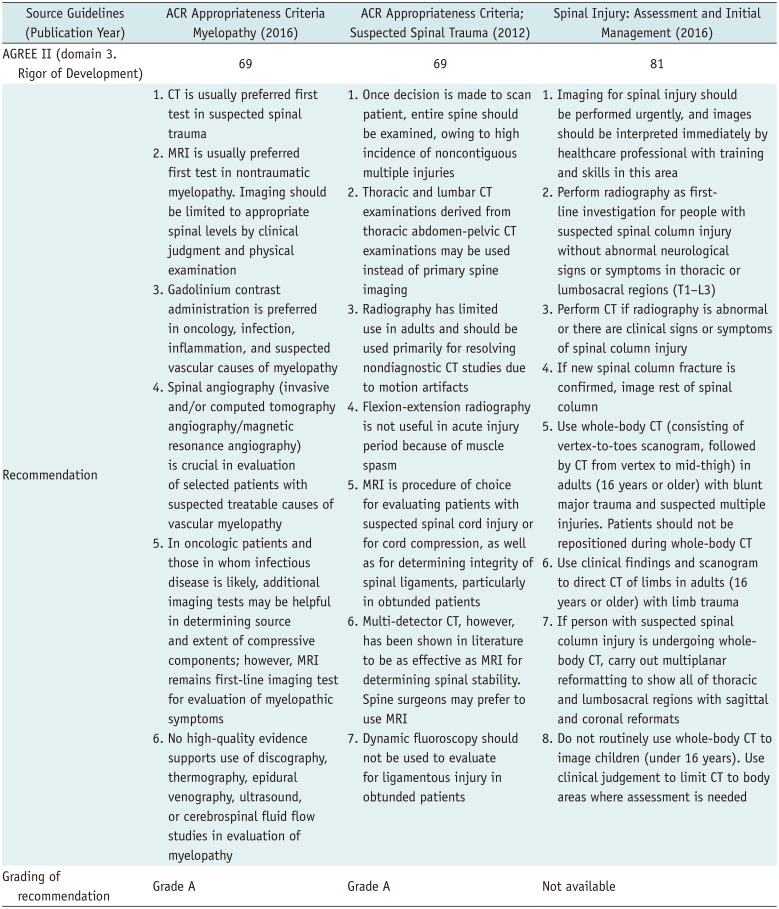
Table 1
Recommendations Matrix of Existing Guidelines (Key Question)
![]()
Grading the Level of Evidence and Drafting the Recommendation Document
The working group members reviewed relevant literature supporting the recommendations stated in the final selected guidelines. Grading the level of evidence of each source of evidence was performed according to the evidence level criteria of the K-CIGs (11).
Agreement of the Recommendation Grades
The draft version of the recommendation document prepared by the working group was reviewed and discussed by the development committee. The final level of evidence and grade of recommendations were determined through consensus between the development committee and the working group, according to the criteria of the K-CIG (11).
Finalizing the Recommendation Document
The Delphi method was used for formal consensus. The consensus group was composed of clinical imaging experts, clinical imaging guideline-related academic societies (end-users), and research methodology experts. The agreement level for recommendation, recommendation grading, and evidence level ranged from strongly disagree (level 1) to strongly agree (level 9). After two rounds of assessment, a consensus was reached.
Seventeen experts from the consensus group answered, and the results of the Delphi were as follows: mean degree of agreement on recommendation was 7.2 (standard deviation: 1.5) in the first survey and 7.4 (standard deviation: 1.0) in the second survey. The coefficient variation decreased from 0.2 to 0.1 which means the extent of agreement between panels increased.
External Review and Approval of Clinical Guidelines
Final recommendations were reviewed by clinical experts. Feedback and modification were reflected in the documents. K-CIG grades were submitted to the Korean Academy of Medical Sciences for approval and dissemination. Final approval was determined on March 13, 2018.
Go to :
Recommendation
Key Question: What Is the Primary Imaging Test for Diagnosis in Patients with Suspected Traumatic Thoracolumbar Spine Injury?
Recommendation
We recommend thoracolumbar spine CT without intravenous contrast enhancement for the diagnosis of traumatic thoracolumbar spine injury (Recommendation grade B, Evidence level II).
Go to :
Evidence Summary
After reviewing several guidelines for the diagnosis of thoracolumbar spine injury in adults with trauma, three guidelines were selected (131415). Previous studies recommended an imaging test to confirm thoracolumbar spine injury when any of the following are present: localizing signs of thoracolumbar injury, a neurologic deficit, cervical spine fracture, Glasgow Coma Scale score less than 15 points, major distracting injury, or a history of alcohol or drug addiction (161718). CT has been reported to be more accurate than plain radiography in the diagnosis of thoracolumbar spine injury (819202122232425). The sensitivity and specificity of plain radiography for the depiction of thoracolumbar fracture have been estimated to be 49–82% and 55–93% compared to CT, respectively (678192024262728293031). Furthermore, reformatted image using axial chest CT or abdominopelvic CT may be helpful to assess thoracolumbar spine injury (78212430313233343536). Because coincident fractures of multiple spinal levels are relatively common, multi-detector CT (MDCT) may be recommended as the first-choice imaging modality (822232435363738). Meanwhile, isolated unstable ligamentous injury without thoracolumbar fracture is rare; thus, additional MRI evaluation is not usually recommended when CT findings are normal (394041). CT demonstrated 0–88% sensitivity and 94–100% specificity for diagnosing of soft tissue injury, except spinal cord injury, compared with MRI (42434445).
Go to :
Considerations for Recommendation
Harm and Benefit
MDCT has a relatively high risk of radiation exposure than plain radiography when used as an initial screening imaging test for the diagnosis of thoracolumbar spine injury. If chest CT or abdominopelvic CT are conducted, reformatted images may be used for assessment of thoracolumbar spine injury without additional thoracolumbar spine CT.
Acceptability and Applicability
CT is available in the majority of hospitals in Korea, and its benefits include short scanning times, and no requirements for IV contrast administration or keeping patients nil per os. As a result of the evaluation of domestic acceptability and applicability of these three guidelines, it was concluded that the acceptability and applicability of thoracolumbar spine CT without IV contrast enhancement are reasonable for diagnosing thoracolumbar spine injury.

Go to :
SUMMARY
This is the first evidence-based clinical imaging guideline document for the screening of thoracolumbar spine injury in Korea, and it was developed using an adaptation process. The primary recommendation is that thoracolumbar CT without IV contrast enhancement should be the first-line imaging modality for the diagnosing thoracolumbar spine injury in patients with suspected spinal trauma.
Go to :
 XML Download
XML Download