

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Echocardiography is essential in the diagnosis of hypertrophic cardiomyopathy (HCM) in cats. Two-dimensional (2D) echocardiography is used to diagnose HCM based primarily on the presence of morphological abnormalities of the left ventricle (LV), such as LV hypertrophy and narrowing of the LV lumen. These morphological changes can also be induced by dehydration. This condition is known as pseudohypertrophy [1], which is a mimic of LV hypertrophy. Pseudohypertrophy (i.e., increased thickness of the LV walls without change in the LV mass) has been observed in cats that were volume depleted by administration of furosemide [1]. It can be difficult to distinguish between pseudohypertrophy and HCM based on echocardiographic assessment of morphology alone.
Dehydration is a commonly encountered clinical situation in cats [234], which can be corrected using fluid therapy. However, fluid therapy can influence the occurrence of congestive heart failure in cats with concurrent HCM. Making an appropriate diagnosis in a cat with a thickened heart is therefore important in deciding on the appropriate fluid regimen.
Diastolic dysfunction is regarded as the main abnormality in HCM [56]. Transmitral flow (TMF) assessment, tissue Doppler imaging (TDI), and speckle-tracking echocardiography (STE) have revealed diastolic dysfunction in cats with HCM [78910]. Furthermore, impairment of diastolic function has been observed during the asymptomatic stage in which the left atrium is not yet enlarged [71011].
We hypothesized that assessment of the diastolic function using echocardiography would aid in the diagnosis of LV pseudohypertrophy induced by volume depletion. This study aimed to assess the echocardiographic indices, particularly with respect to diastolic function, in healthy cats with hypovolemia.
MATERIALS AND METHODS
Animals
This experimental study protocol was approved by the Azabu University Animal Care and Use Committee (No. 170203-2).
Nine experimental cats were used in this study (4 females, 5 males; age 60 month; weight 2.58–4.49 kg). No cats were undergoing any treatment. In all cats, a complete clinical assessment was performed to exclude systemic diseases; this comprised a physical examination, complete blood count, performance of biochemical blood tests, electrocardiography, echocardiography, and thoracic radiography. There were no abnormal findings in any cats in this study.
The cats were housed in separate cages (1 cat per cage); they were provided commercially available cat food, and had access to water ad libitum.
Experimental protocol
Cats were subjected to both a placebo and a dehydration protocol. Echocardiographic parameters were measured, as well as body weight (BW) and systolic blood pressure (SBP); a blood sample was collected for measurement of the serum total protein (TP), packed cell volume (PCV), and serum angiotensin-converting enzyme (ACE) activity at the start of each intervention. An intravenous (IV) catheter was placed in the cephalic vein through which saline or furosemide could subsequently be administered. All cats were assigned to the dehydration intervention first. Subsequently, a complete clinical assessment was re-performed after a 21-day wash-out period, at which point it was confirmed that baseline conditions had returned to normal and were the same as the baseline conditions prior to the dehydration protocol.
Furosemide (Lasix [20 mg/2 mL], Nichi-Iko Pharmaceutical, Toyama, Japan) was administered via IV at a dose of 2–4 mg/kg/h until a body weight reduction of 7%–10% was reached; if weight reduction was < 7%, furosemide was administered to a cumulative total of 14 mg/kg over a period of 5 h, based on the dose previously reported [1]. If the target BW was achieved, SBP and echocardiographic parameters were measured (Dehydration protocol). BW was determined without emptying the urinary bladder. The cats had free access to water during the experiment. Immediately after the dehydration protocol was completed, isotonic saline (0.9% NaCl, Otsuka Pharmaceutical, Japan) was administered over several hours, in accordance with standard fluid therapy guidelines, until cats had achieved rehydration and BW reached baseline [1].
For each cat, saline was administered using the same volume and at the same intervals as those for furosemide during the dehydration protocol (Placebo protocol), thus ensuring an identical administration regimen for both protocols.
Echocardiographic examination
In this study, echocardiographic images were taken using an ultrasound unit equipped with a 7-MHz transducer (Vivid 7 dimension, GE Medical System, Japan). All echocardiographic examinations were performed by one sonographer (KS). Cats were gently restrained in a lateral recumbent position without sedation or anesthesia. All echocardiographic images were analyzed with commercial software (EchoPAC PC, GE Medical System). Three consecutive measurements were performed and an average of the 3 values was obtained for each parameter.
Aortic diameter (AoD) and left atrial diameter (LAD) at end-systole were assessed by using the right-sided parasternal short-axis view at the level of the aortic valve with an existing 2D method [1213]. Left ventricular internal diameter (LVIDd), LV free wall thickness (LVFWd), and interventricular septum thickness (IVSd) at end-diastole were assessed by using the right parasternal short-axis view at the level of the chordae tendineae with M-mode images. The heart rate (HR) was also determined on the basis of M-mode images.
Diastolic function was evaluated with a pulse wave, color TDI, and STE. The left apical four-chamber view was used to characterize TMF patterns. Color flow Doppler imaging was applied to facilitate positioning of a cursor in line with mitral inflow. In addition, a sampling gate was positioned in line with this flow at the level of the open mitral valve tips [13]. The peak early (E) and late (A) diastolic filling velocities were measured and used to calculate the E/A ratio.
All color TDI examinations were performed using an existing method [14]. Lateral and septal aspects of the mitral annulus were evaluated with the left 4-chamber apical view. A 2×2-mm sample volume was used without angle correction. Lateral and septal peak early diastolic velocities (Lat E′ and Sept E′, respectively) were measured and used to calculate the E/E′ ratio.
Longitudinal strain rate was measured using STE as previously described [10]. Peak longitudinal strain rate during early diastole (SrLe) was measured with the left apical 4-chamber view in 6 segments: basal, middle, and apical regions of both lateral and septal walls. Average measurements from these 6 ventricular segments were used to calculate the SrLe used for statistical analysis.
Serum ACE activity
Blood samples (approximately 1 mL) were collected in tubes without anticoagulant before and after furosemide or saline administration. All samples were centrifuged to obtain serum (3000 rpm, 10 min). ACE activity was measured with an ACE assay kit (ACE Color, Fujirebio, Japan).
Systolic blood pressure
Non-invasive measurement of SBP was performed with Doppler sphygmomanometry (Hadeco, Japan), using an inflatable cuff on the tail as previously described [15]. Hair was clipped before positioning of the probe, and the cuff was inflated manually such that the pulse signal was not discernible; it was then gradually deflated. In this study, SBP was the pressure at which the Doppler signal became discernible during cuff deflation. Multiple measurements were performed at each time point in a consecutive manner. The mean value of 5 stable measurements was used for statistical analyses.
Statistical analysis
All measurements are expressed as mean ± standard deviation. Statistical analyses were performed using SPSS Statistics version 21.0 (IBM, USA). Cats that showed separation of peak early diastolic velocity from peak atrial systolic velocity on echocardiography in both protocols were used for all statistical analysis.
BW, PCV, SBP, serum ACE activity, conventional echocardiographic indices, E, E′, and SrLe recorded before each protocol were compared with the Wilcoxon signed-rank test to evaluate carry-over effects of furosemide.
To fulfill the primary aim of this study (i.e., evaluating the effects of the interventions), the difference between the baseline value (pre-) and the value recorded following the protocol (post-) was calculated for all measurement variables, and a comparison between the protocols was performed using the Wilcoxon signed-rank test.
To evaluate the effects of intervention, affected indices were detected by comparing values recorded pre- and post-each protocol using the Wilcoxon signed-rank test. Differences were regarded as significant when p < 0.05.
RESULTS
Animals
All protocols were performed within 5 h to 5 h 30 min. Out of the nine cats, six had E and A waves that were suitably separated in both protocols for them to be included in all subsequent analyses. Out of these six cats, there were four females and two males. All cats received a total of 14 mg/kg of furosemide in the dehydration protocol.
BW, PCV, TP, SBP, and serum ACE activity
The results of measurements of BW, PCV, TP and SBP are shown in Table 1. The post-intervention TP measurements were significantly increased with the dehydration protocol compared to placebo. There were no significant differences in other indices pre- compared to post-intervention for either protocol (p > 0.05). SBP was statistically unchanged when compared before and after the Dehydration protocol, although the one cat showed decreased SBP from 167 mmHg to 90 mmHg. During the placebo protocol, pre and post-intervention SBP measurements increased from 140 mmHg to 190 mmHg in one cat, but were not statistically different in the rest of the sample.
Table 1
The results of measurements of BW, SBP, and PCV in both protocols (mean ± SD)

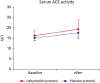
Serum ACE activity measurements are depicted in Fig. 1; there was no significant difference pre- compared to post-intervention for either protocol (p > 0.05).
Echocardiography
Tables 2 and 3 and Fig. 2 show echocardiographic examination results. No significant differences were observed in echocardiographic indices between the baseline of the two protocols. Administration of furosemide induced significant increases in the LV wall thickness (IVSd and LVFWd) and diminished chamber diameters (LVIDd and LAD). There were 2 cats whose IVSd dimensions exceeded 5.5 mm after furosemide administration. Neither protocol altered the HR or AoD. Volume depletion did not affect SrLe, E/E′ ratio, or E/A ratio; however; the A wave, E wave, Lat E′, and Sept E′ were significantly decreased during the dehydration protocol compared to placebo protocol. During the dehydration protocol, the A wave, E wave, Lat E′, and Sept E′ were significantly decreased post- compared to pre-furosemide administration. There were no significant differences in these indices pre- compared to post-saline administration during the placebo protocol.
Table 2
The results of conventional echocardiographic examination in both protocols (mean ± SD)

IVSd, interventricular septal thickness at end-diastole; LVIDd, left ventricular internal diameters at end-diastole; LVFWd, left ventricular free wall thickness at end-diastole; AoD, aortic diameter at end-systole; LAD, left atrial diameter at end-systole; HR, heart rate; SD, standard deviation.
*p < 0.05 compared to Placebo protocol; **p < 0.01 compared to Placebo protocol.
Table 3
Echocardiographic diastolic indices in both protocols (mean ± SD)
SD, standard deviation; E wave, peak early diastolic filling velocity; A wave, peak late diastolic filling velocity; Lat E′, lateral peak early diastolic velocity; Sept E′, septal peak early diastolic velocity; SrLe, peak longitudinal strain rate during early diastole.
*p < 0.01 compared to Placebo protocol; **p < 0.05 compared to Placebo protocol.
Fig. 2
Echocardiographic diastolic indices. No significant differences were present in SrLe, E/A ratio, and E/E′ ratio between the Dehydration and Placebo protocols.
SrLe, peak longitudinal strain rate during early diastole; E wave, peak early filling velocity; A wave, late filling velocity; E′, peak early diastolic myocardial velocity at the mitral annulus, Lat E′, lateral peak early diastolic velocity; Sept E′, septal peak early diastolic velocity; SrLe, peak longitudinal strain rate during early diastole.
*p < 0.05 compared to Placebo protocol; **p < 0.01 compared to Placebo protocol.

DISCUSSION
In our model, volume depletion was induced by administration of furosemide, a potent short-acting diuretic. Although BW and PCV were not changed, LVIDd and LAD were significantly decreased in all cats during dehydration compared to the placebo protocol. Thus, the reduction in the dimensions of the LV and LA showed a decreased preload. In addition, the LV wall thickness was significantly increased in all cats during volume depletion, and there were 2 cats whose LV thickness exceeded 5.5 mm (pseudohypertrophy). Since PCV was measured several hours after collecting the blood sample in some cats, this may have led to some technical errors in this measurement. This aside, these results show that volume depletion was successfully induced in this study.
It has previously been reported that E wave, E′, E/A, and SrLe were decreased in cats with HCM and E/E′ was increased in human patients with HCM [78910]. We hypothesized that these indices were useful to distinguish pathological hypertrophy due to HCM from pseudohypertrophy. The current study revealed that E/E′, SrLe, and E/A showed no changes after dehydration. However, the E wave and E′ were significantly affected by volume depletion. Therefore E/A, SrLe and E/E′ could be indices that distinguish HCM and pseudohypertrophy.
This study revealed that Lat E′ and Sept E′ were significantly decreased in cats with normal diastolic function who were volume depleted. E′ is generally known as a preload-independent index of diastolic function [16], and several studies have demonstrated that E′ is decreased in cats with HCM [9141718]. In humans, relatively abrupt changes in preload have been observed after hemodialysis is performed. Tamano et al. [19] demonstrated that E′ did not change after hemodialysis in human patients; however, Ie et al. [20] have reported contrary results that showed E′ was decreased after hemodialysis. Tamano et al. [19] reported that discrepancies in the results were due to differences in the amount of fluid removed from the patients, the basal conditions of the patients, and differences in cardiac function. Diastolic function in our cats was normal at baseline, and volume depletion was acutely induced. Therefore, E′ was possibly affected by the rapid reduction of the preload.
TDI is angle dependent [21], therefore, technical error can be another possible cause of the decreased E′. Reduction of the preload significantly reduced the LV lumen, resulting in changes in the position of the mitral annulus. A previous report stated that the movement of the septal side of the annulus was more parallel to the ultrasonic beam; thus, it showed less effects due to translational movement of the heart, relative to the movements of other regions [22].
The results of TMF assessment in the current study showed that the E and A waves were both significantly decreased during the dehydration protocol, resulting in an unchanged E/A ratio. Several studies have revealed that the E wave is strongly influenced by preload, although the extent of preload reduction influence on the A wave is reportedly inconsistent [232425].
Our group previously reported that STE showed greater sensitivity than TDI for evaluation of left ventricular diastolic function in cats with HCM [10]. One of the diastolic STE parameters, SrLe, did not change during dehydration in the current study. Strain and strain rate during systole are reportedly affected by the preload and afterload [2627]; however, to the best of our knowledge, the influence of the preload reduction on SrLe is not well known. Fredholm et al. [28] reported that an increased preload or an elevated HR increases the strain rate during diastole. The HR in the current study was not significantly changed; therefore, a further study is warranted to determine the factors that influence the diastolic STE parameters when the preload is changed.
The E/E′ ratio may be a useful tool for evaluation of LV filling pressures because it combines the effects of transmitral driving pressure and myocardial relaxation [293031]. In our study, both the E wave and E′ were significantly decreased, resulting in an unchanged E/E′ ratio. Although the E/E′ ratio was applied to estimate LV filling pressure, we found that it not was affected by preload reduction.
The present study had a number of limitations. First, we used an acute dehydration model. Serum ACE activity and SBP did not significantly change during volume depletion. These results implied that experimentally-induced dehydration may be different from dehydration occurring in cats with chronic diseases. Second, the E wave and the A wave are often summated because of high HR in cats, and this summation was present in three of nine cats in the present study. Third, the sample size was small. Fourth, echocardiographic indices are influenced by many other factors associated with volume depletion. Acute changes in echocardiographic parameters after hemodialysis reportedly may be explained by several mechanisms, including the change in serum ionized calcium concentration, increased oxidative stress during hemodialysis, and sympathetic hyperactivity [30]. Similar changes may have occurred in cats that were administered furosemide. Fifth, echocardiographic examination and analysis were not performed in a blinded manner.
In conclusion, we showed that acute dehydration induced by using furosemide affected the echocardiographic parameters, especially those of the diastolic function, in healthy cats. Volume depletion significantly affected both echocardiographic diastolic indices and conventional echocardiographic parameters. The cats' hydration status should be considered when interpreting echocardiographic parameters.
 XML Download
XML Download