

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Chronic rhinosinusitis (CRS) is a chronic inflammatory disease of the sinonasal mucosa lasting for at least 12 weeks. Based on the presence of nasal polyps (NPs), the clinical phenotype of CRS is categorized into CRS with nasal polyp (CRSwNP) and CRS without nasal polyp (CRSsNP).1 However, this dichotomization of the phenotype does not demonstrate the pathology of CRS at the cellular and molecular levels. Recently, endotypes of CRS based on inflammatory profiles have emerged to help identify clinical features and aid in disease management.234567
Endotyping systems, however, are of limited practical use because they often require invasive procedures, such as nasal tissue biopsy. According to the Japanese Epidemiological Survey of Refractory Eosinophilic Chronic Rhinosinusitis (JESREC) clinical scoring system for endotyping,8 CRS patients can be categorized into the following groups based on blood eosinophilia, clinical parameters, and CT findings: 1) non-eosinophilic CRS (non-ECRS), 2) mild eosinophilic CRS (ECRS), 3) moderate ECRS, and 4) severe ECRS. These subgroups demonstrate a significant correlation with the recurrence and refractoriness of CRS. Moreover, clinicians can easily evaluate patients with this scoring system, because the JESREC scoring system does not require an invasive procedure. However, despite the advantages of this system for practical endotyping of CRS, the JESREC scoring system might overrate the prognosis of patients with non-ECRS with nasal polyps (non-ECRSwNP) because the system does not differentiate CRSwNP from CRSsNP.8 Consequently, as the majority of CRSsNP appears to be subclassified into non-ECRS, the prognosis of non-ECRS may be influenced by that of CRSsNP, which shows better treatment outcomes than CRSwNP.9 Therefore, non-ECRSwNP should be evaluated separately from non-ECRS without NPs to prevent overestimation of the prognosis and to compare ECRSwNP and non-ECRSwNP properly in terms of NPs. Considering the high prevalence of non-ECRSwNP in the Asian population,10 validation of the JESREC system with CRSwNP alone is necessary, as this would enable proper assessment of the prognosis in non-ECRSwNP.
Go to : 
MATERIALS AND METHODS
Study population
A retrospective analysis was performed among 134 CRSwNP patients who were prospectively enrolled and underwent functional endoscopic sinus surgery after maximal medical treatment. Functional endoscopic sinus surgery was performed by one experienced surgeon (DWK). The diagnosis was based on clinical history, clinical examination, and findings on nasal endoscopy and CT of the sinuses according to the guidelines of the European Position Paper on Rhinosinusitis and Nasal Polyps 2012 (EPOS 2012).11 Exclusion criteria were as follows: 1) patients younger than 18 years, 2) previous treatment with antibiotics, systemic or topical corticosteroids, or other immunemodulating drugs during the last 4 weeks before surgery, and 3) conditions, such as unilateral rhinosinusitis, allergic fungal sinusitis, antrochoanal polyp, ciliary dyskinesia, or cystic fibrosis. NP tissues were obtained during functional endoscopic sinus surgery. All samples were fixed with 10% formaldehyde and embedded in paraffin for histological analysis. The atopic status of the subjects was assessed with ImmunoCAP assay (Phadia, Uppsala, Sweden) to detect specific IgE antibodies to the six common aeroallergen mixtures (house dust mites, molds, trees, weeds, grass, and animal dander). Patients who had allergen-specific IgE levels >0.35 IU/mL to one or more allergens were considered atopic.12 The diagnosis of asthma was based on personal history and lung function analysis by the allergists. Lund-Mackay CT scores and global osteitis scores13 were calculated with the CT scans before surgery. Odor threshold was evaluated using the butanol threshold test (BTT), which was performed as described in our previous study.14 Other clinical characteristics, such as smoking history, alcohol intake history, and body mass index, were analyzed. JESREC score was calculated in the 134 patients based on their results of nasal endoscopy, CT scans, and blood eosinophil infiltration.8
Patients with CRSwNP were categorized into non-ECRSwNP, mild ECRSwNP, moderate ECRSwNP, and severe ECRSwNP groups according to the JESREC scoring system.8 Additionally, the disease control status of individual patients was evaluated at 1 year after surgery and classified into three categories according to the EPOS 2012 guidelines11: controlled, partly controlled, and uncontrolled. These patients were further divided into two groups: 1) disease-controlled group (patients in controlled status) and 2) disease-uncontrolled group (patients in partly controlled or uncontrolled status). Prognostic factors for disease control status were investigated according to the JESREC classification. This study was approved by the Institutional Review Board of Seoul National University Hospital, Boramae Medical Center (No. 10-2018-80).
Histological evaluation
Immunohistochemical staining was performed using the Polink-2 and polymerized horseradish peroxidase (HRP) broad DAB-Detection System (Golden Bridge International Labs, Bothell, WA, USA). After deparaffinization, sections were incubated in 3% hydrogen peroxidase to inhibit endogenous peroxidase activity. Subsequently, heat-induced epitope retrieval was performed by microwaving the samples in 10 mmol/L citrate buffer (pH 6.0). These sections were incubated for 60 minutes at room temperature in a primary antibody, rabbit anti-human neutrophil elastase (1:500; Abcam, Cambridge, UK). The sections were then incubated in broad antibody enhancer and polymer-HRP and were stained with the DAB detection system. Finally, the slides were counterstained with hematoxylin, and eosinophil counts were determined by hematoxylin and eosin staining. The number of positive cells was counted in the five densest visual fields (×400) by two independent observers, and the average values were calculated.
Statistical analysis
Continuous variables of demographic and clinical characteristics are presented as a median and interquartile range (IQR), and were analyzed using the Mann-Whitney U-test with a two-tailed test for unpaired comparisons. Fischer's exact test and chi-square test were performed to evaluate categorical variables, such as disease control status of the non-ECRSwNP and ECRSwNP groups. Values statistically significant in univariate analysis for potential prognostic factors were included in binary logistic regression analysis for multivariate analysis. Jonckheere-Terpstra test was applied to evaluate disease control status and tissue eosinophil counts according to JESREC classification. A receiver operating characteristic (ROC) curve of the tissue neutrophil and eosinophil counts was generated to find the best cutoff for predicting disease control status. The area under the curve (AUC) for each potential predictor was calculated: an AUC with a value close to 1 indicates a high accuracy of prediction. Among several cutoff points, the lowest (1-sensitivity)2+(1-specificity)2 value was selected as the optimal cutoff value. All statistical analyses were performed using R for Windows, version 3.4.2 (R Foundation for Statistical Computing, Vienna, Austria). All p values <0.05 were considered statistically significant.
Go to :
RESULTS
Non-ECRSwNP and ECRSwNP
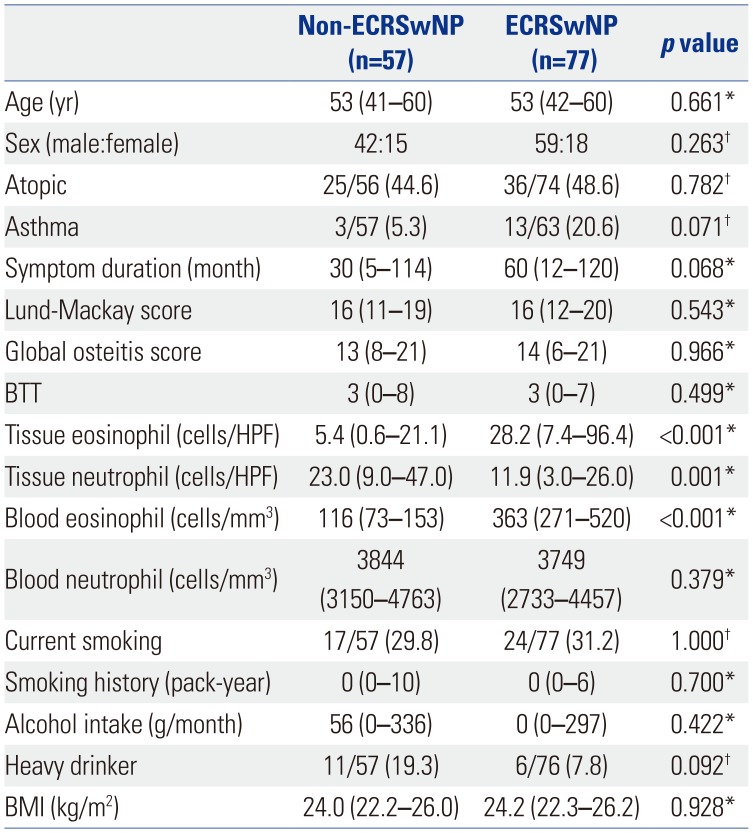
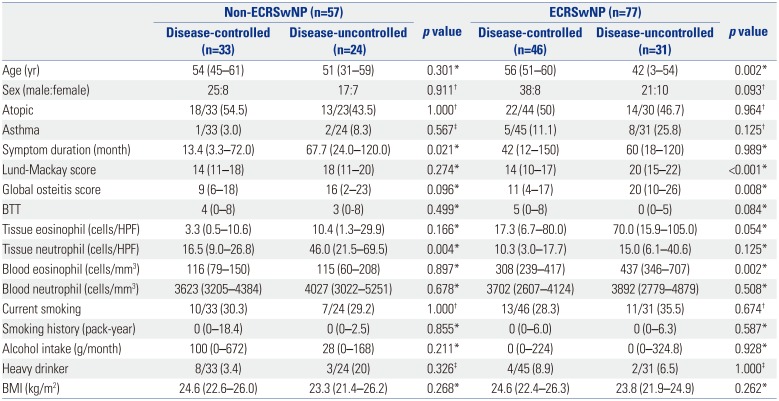
There was a significantly increasing trend in the tissue eosinophilic counts from non-ECRS to severe ECRS (p<0.001) (Fig. 1). The patients were divided into non-ECRSwNP and ECRSwNP groups; the clinical characteristics of both groups are demonstrated in Table 1. Tissue and blood eosinophil counts were higher in the ECRSwNP group (p<0.001), while the tissue neutrophil count was higher in the non-ECRSwNP group (p=0.001).
 | Fig. 1Eosinophils count of all patients according to JESREC classification. Classification revealed a significant difference in tissue eosinophil counts. *p<0.01, †p<0.001. JESREC, Japanese Epidemiological Survey of Refractory Eosinophilic Chronic Rhinosinusitis; ECRSwNP, eosinophilic chronic rhinosinusitis with nasal polyps; HPF, high power field.
|
Table 1
Clinical Characteristics of Non-ECRSwNP and ECRSwNP Groups
![]()
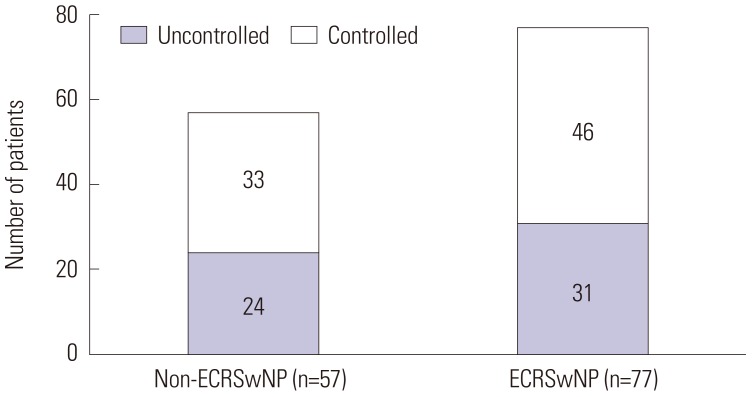
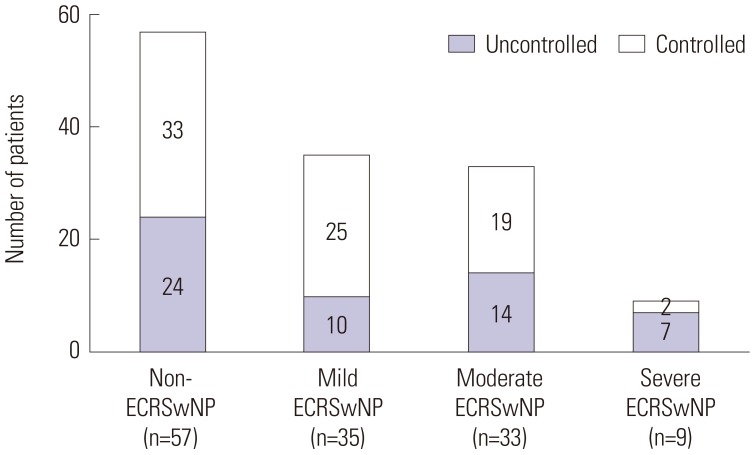
Comparison of disease control status revealed no significant difference between non-ECRSwNP and ECRSwNP groups (p=0.970) (Fig. 2). Additionally, disease control status did not show any significant difference among subgroups and did not reflect the degree of eosinophilic inflammation according to classification (p=0.245) (Fig. 3). Meanwhile, however, subgroup analysis of the ECRSwNP group (mild, moderate, and severe ECRSwNP) revealed a significant difference in disease control status that reflected degree of eosinophilic inflammation by classification (p=0.021). These results implied that the classification reflects the effect of eosinophilic severity on ECRSwNP, but does not predict the clinical outcomes of non-ECRSwNP.
Prognostic factors
Based on their disease control status, all patients were divided into two groups as follows: 1) disease-controlled group (n=79) and 2) disease-uncontrolled group (n=55). The clinical profiles were compared between the two groups to investigate prognostic factors. Univariate analysis revealed that some potential prognostic factors, such as young age, high Lund-Mackay CT scores, high global osteitis scores, and high levels of tissue eosinophilia and neutrophilia, were associated with worse disease control status (p<0.05) (Table 2). Subsequently, age, Lund-Mackay CT scores, global osteitis scores, tissue eosinophilia, and neutrophilia were included in multivariate analysis, which showed age, Lund-Mackay CT scores, tissue eosinophilia, and tissue neutrophilia to be correlated with disease control status (p<0.05) (Table 2).
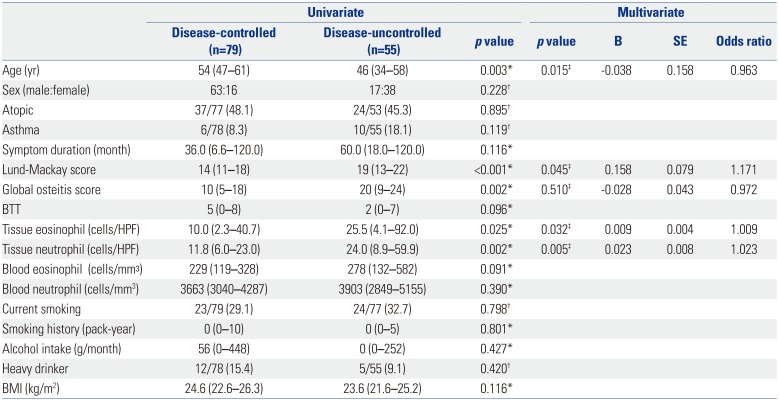
Table 2
Prognostic Factors for Disease Control Status
![]()
Subgroup analysis of non-ECRSwNP and ECRSwNP
Patients with worse disease control status had higher tissue neutrophil counts in subgroup analysis of the non-ECRSwNP group (p=0.004) (Table 3). Conversely, ECRSwNP patients with higher tissue eosinophil count tended to exhibit worse disease control status (p=0.054). Additionally, subgroup analysis of the ECRSwNP group revealed that young age, high Lund-Mackay CT scores, high global osteitis scores, and high blood eosinophil count were associated with worse disease control status (p<0.05). To determine the subjects with worse disease control status among the patients with non-ECRSwNP and ECRSwNP, respective tissue neutrophil and eosinophil counts were analyzed on ROC curves (Fig. 4). The AUCs were 0.731 and 0.631 for tissue neutrophil and eosinophil counts, respectively. The best threshold value with optimal sensitivity and specificity yielded a value of ≥40.0 for tissue neutrophil cells, with HPF demonstrating a sensitivity and specificity of 56.5% and 90.3%, respectively, in the non-ECRSwNP group (Fig. 4A) and a value of ≥43.6 for tissue eosinophil cells, with HPF demonstrating a sensitivity and specificity of 66.7% and 61.3%, respectively, in the ECRS group (Fig. 4B).
 | Fig. 4ROC curves of tissue neutrophil and eosinophil counts for predicting the disease control status. (A) ROC curve for tissue neutrophil counts in the non-ECRSwNP group. (B) ROC curve for tissue eosinophil counts in the ECRSwNP group. The predictive ability was calculated based on the AUC. ECRSwNP, eosinophilic chronic rhinosinusitis with nasal polyps; ROC, receiver operating characteristic; AUC, area under the curve.
|
Table 3
Subgroup Analysis of Non-ECRSwNP and ECRSwNP Groups
![]()
Go to :
DISCUSSION
In the past, CRS was simply divided into two phenotypes based on the presence of NPs. However, this simple classification has a limited ability to categorize the various inflammatory profiles of CRS for successful treatment planning. Moreover, the distinct features of NP emphasize the necessity of endotyping7; hence, endotyping systems of CRS have been investigated recently. The majority of NPs in the United States and Europe are TH2-biased and eosinophilic, with the expression of IL-4, IL-5, and IL-13.15 Conversely, only a minority of NPs are TH2-biased in Asian countries; the majority are TH2-negative and neutrophilic with the expression of IFN-γ and/or TH17.1516 Therefore, endotyping is essential to distinguish the broad spectrum of CRS in order to aid in proper management. The JESREC scoring system is a novel scoring system that can be easily used by clinicians because it does not require invasive procedures, such as nasal tissue biopsy. However, the patients with NP in the non-ECRS group may not have been properly assessed in the previous study,8 because the non-ECRS group also involved a majority of CRSsNP patients. Therefore, the prognosis of patients with NP in the non-ECRS group were possibly overestimated due to the favorable treatment outcomes of patients with CRSsNP. Considering the prevalence of non-eosinophilic NP in Asia, the prognosis of patients with NP was compared between non-ECRS and ECRS in this study.
In the present study, 134 patients with CRSwNP were classified into four groups. In contrast to the Japanese study,8 the classification did not demonstrate a significant difference in disease control status, and there was no significant difference between non-ECRSwNP and ECRSwNP groups. However, the subgrouping of ECRSwNP demonstrated a significant difference in disease control status that reflected degree of eosinophilic inflammation by the classification, which suggests severe eosinophilic infiltration was associated with a lower disease-controlled rate in patients with ECRS. The division of patients into disease-controlled and disease-uncontrolled groups to investigate factors associated with disease control status revealed tissue eosinophilia as a potential prognostic factor in multivariate analysis of all patients. This finding was consistent with the results of previous studies.171819 However, in the subgroup analysis, tissue eosinophilia was related to disease control status in the ECRSwNP group, but not in the non-ECRSwNP group. Instead of tissue eosinophil count, high tissue neutrophil count was found to be a potential prognostic factor in the non-ECRSwNP group. This reflects the existence of two different endotypes of CRSwNP. Furthermore, the prognosis of CRSwNP was not significantly different between eosinophilic NP and neutrophilic NP in a few previous studies.1920 Additionally, the disease-uncontrolled rate of CRS patients with neutrophilic NP was reported to be close to 50% in previous Chinese studies,2122 a finding which is consistent with the present study. Neutrophils are traditionally considered as acute inflammatory cells, and their role in CRSwNP is not well known. Interestingly, in the study by Wang, et al.23 IL-36γ/IL-36R was found to be closely associated with neutrophils in NPs and to play a role in CRS perpetuation. Furthermore, oncostatin M, which is primarily released from neutrophils, was involved in barrier disruption, which is one of the major pathologic mechanisms of NPs.2425 In the present study, we assumed that neutrophils might be a major pathologic driver in patients with non-ECRSwNP rather than those with ECRSwNP. Further investigation should be performed to reveal the pathogenesis of neutrophils in NPs of non-ECRS and ECRS.
In the present study, patients were classified based on the JESREC scoring system, and clinical characteristics and disease control status were evaluated. In contrast to a previous study,8 only patients with CRSwNP were included in this study, and patients with ECRS and non-ECRS were compared without CRSsNP-induced overestimation of non-ECRS. Therefore, the prognosis of eosinophilic and non-eosinophilic NP could be compared properly. However, there are two limitations in this study that hinder comparison with the results of the aforementioned study. First, the evaluation tools for prognosis were different. Recurrence and refractory rates were used to assess the subjects' prognosis in the study by the Japanese group, whereas EPOS control criteria were employed to determine prognosis in this study. Second, this study was performed for a smaller population, compared with the previous study; hence, further investigation with a large population of CRSwNP is required.
In conclusion, there was no significant difference in disease control status in non-ECRSwNP and ECRSwNP groups according to JESREC classification. Tissue neutrophil was identified as a potential cellular marker for disease control status in non-ECRSwNP, whereas tissue eosinophil was a marker in ECRSwNP. Accordingly, clinicians should consider the heterogeneity of NPs and different prognostic factors when consulting with patients with CRSwNP.
Go to :
 XML Download
XML Download