

 PDF
PDF ePub
ePub Citation
Citation Print
Print


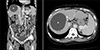
A 57-year-old woman with a medical history of alcoholic liver cirrhosis was admitted to the emergency room with epigastric pain and progressive leg edema. Vital signs were normal, and the patient's abdomen was soft. The patient had normal kidney and cardiac function. Esophagogastroduodenoscopy showed neither gastritis nor peptic ulcers. Contrast-enhanced computed tomography (CECT) revealed that a 10.2-cm hepatic cyst had indirectly compressed the inferior vena cava (IVC) (Fig. 1). Six months previously, the cyst size was 8.8 cm, and the IVC was not compressed. Percutaneous transhepatic aspiration of the cyst was performed under sonographic guidance, and 275 mL of serosanguineous fluid was obtained causing an approximately 2 cm decrease in the cyst diameter. All symptoms resolved after the procedure, and cytologic examination of the aspirated fluid confirmed no evidence of malignancy. One week later, a follow-up CECT showed improvement of the IVC compression (Fig. 2). Therefore, the intracystic hemorrhage of a simple hepatic cyst leading to a focal narrowing in the IVC was considered the cause of epigastralgia and swelling of the legs. Fortunately, the patient has had no recurrence without any additional treatment for 3 years after the needle aspiration without sclerotherapy.
Although most hepatic cysts are asymptomatic, they can cause serious complications, such as obstructive jaundice, rupture, infection, and intracystic hemorrhages.1 Symptoms of hemorrhagic hepatic cysts include nausea and abdominal pain.2 Hepatic cysts may also cause obstructions on the IVC, which may lead to massive edema of the legs.3 In most cases, the causes of the intracystic hemorrhage are unclear.2 It is important to differentiate hepatobiliary cystic neoplasms from simple hepatic cyst complicated by intracystic hemorrhages.4 Treatment options for symptomatic hepatic cysts include surgery and needle aspiration with or without injection of a sclerosing agent into the cyst.3

 XML Download
XML Download