

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Temporomandibular disorders (TMD) are defined as clinical syndromes characterized by pain and dysfunction of the temporomandibular joint (TMJ) and related masticatory muscles.1 Many factors have been suggested to cause TMD, such as unstable occlusion, psychological factors, and genetic predisposition.2 Among the potential factors, there has been considerable controversy regarding the relationship between occlusal interference and TMD; this has led to questions regarding whether orthodontic treatment is associated with TMD. Notably, the association between orthodontic treatment and TMD remains a controversial issue. Some clinicians have reported that occlusal factors, including orthodontic treatment, are not related to the presence of TMD.3 Other authors have reported that orthodontic treatment is related to the presence of signs and symptoms of TMD.45 Importantly, most orthodontic patients are children and adolescents; the periods in which they undergo orthodontic treatment coincide with the periods that exhibit the greatest prevalence of TMD. Most orthodontic patients are women, in whom TMD is more common. Such age- and gender-related coincidences cause difficulty in defining the relationship between orthodontic treatment and TMD; analyses of the association between TMD and orthodontic treatment should adjust for age- and gender-related effects. However, most previous studies have not consider the effects of such confounding factors and did not target representative populations.
The purpose of the present study was to investigate the relationship between a history of orthodontic treatment and the presence of TMD, using National Health Data, and to analyze the results while adjusting for confounding factors.
MATERIALS AND METHODS
Study population
The data analyzed in this study were from the 2012 Korean National Health and Nutrition Examination Survey (KNHANES). The KNHANES is a nationwide survey conducted by the Division of Chronic Disease Surveillance at the Korean Centers for Disease Control and Prevention. This survey is conducted once per year for the entire population. All participants signed an informed consent form. The survey comprised health interviews, health examinations, and a nutrition survey. Trained interviewers performed face-to-face interviews with a structured questionnaire. Trained and calibrated examiners inspected the physical status of each participant. In this survey, a total of 8,057 participated; the overall participation rate was 80.8%. The participant rate was 79.2% for the health interview and examination portion. Exclusion criteria for this study were age < 19 years (1,765 participants) and missing values in the health assessment or questionnaires (725 participants). The final sample size was 5,567 participants.
Variables
Clinical and laboratory data were obtained by use of questionnaires and clinical examinations. Higher education levels were defined as completion of high school or further education. Household income earners in the lowest quartile were classified as low-income group. Mild-to-moderate alcohol drinkers were those who had < 30.0 g alcohol/day. Regular exercise was defined as physical activity performed at least three times per week for at least 20 minutes per session.
Body mass index (BMI) was calculated as weight in kg, divided by height in m2. Waist circumference was measured at the narrowest point between the lower border of the rib cage and the iliac crest. Metabolic syndrome was defined in accordance with the American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement criteria for Asians. Metabolic syndrome was diagnosed by three or more of the following criteria: 1) waist circumference ≥ 90 cm in men or ≥ 80 cm in women; 2) fasting triglyceride ≥ 150 mg/dL or use of lipid-lowering medication; 3) high density lipoprotein cholesterol < 40 mg/dL in men or < 50 mg/dL in women or use of cholesterol-lowering medication; 4) blood pressure ≥ 130/85 mm Hg or use of antihypertensive medication; and 5) fasting blood glucose ≥ 100 mg/dL or current use of anti-diabetic medication.
Subjective mental stress rate, suicidal thoughts, and diagnosis of depression were selected as psychological variables. Subjective mental stress rate was classified as high (Likert scale 1, 2) and low (Likert scale 3, 4), based on questionnaires that used a 4-point Likert scale, from 1 (very severe) to 4 (almost never). The participants also responded “yes” or “no” to the following questions: “Have you ever thought about suicide?” and “Are you diagnosed with depression by your doctor?”
Chewing difficulty and speaking difficulties were evaluated by using a yes/no questionnaire. A history of orthodontic treatment was evaluated by using a yes/no questionnaire. All TMD examinations were performed by trained and calibrated dentists. TMD signs and symptoms were assessed in accordance with the criteria of the World Health Organization: 1) TMJ clicking; 2) tenderness of the anterior temporal and/or masseter muscle areas; and 3) reduced jaw mobility. Clicking was defined as an audible or palpable TMJ sound. Tenderness was defined by using two-finger pressure and was measured twice at the thickest muscle area. Reduced jaw mobility was defined as < 30 mm, or less than three-finger width of inter-incisal distance. TMD was defined as the presence of at least one of the above signs or symptoms, once or more per week, within the most recent 1 year.
Statistical analysis
All data are presented as mean ± standard errors or percentage. Logistic regression analyses were used to evaluate associations between orthodontic treatment and TMD. Regression analyses were performed in accordance with KNHANES statistical guidelines. Odds ratios (ORs) and 95% confidence intervals (CIs) were estimated after adjustment for potential confounders.
Four multiple regression models were used. Model 1 was not adjusted. Model 2 was adjusted for age, while Model 3 was adjusted for age and sex because TMD is more prevalent in young female than in male. Model 4 was adjusted for the variables in Model 3, as well as income, education, subjective mental stress rate, suicidal thoughts, and diagnosis of depression; this approach was used because psychological problems have been suggested to cause TMD. Income and education levels were also regarded as confounding factors because orthodontically treated populations have a higher socioeconomic status.
SAS version 9.2 (SAS Institute Inc., Cary, NC, USA) was used for statistical analysis and p < 0.05 was considered to indicate statistically significant differences.
RESULTS
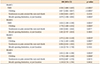
The mean age of the orthodontic treatment group was lower than that of the group without orthodontic treatment (Table 1). Most participants in the orthodontic treatment group were female (62.4%). Those in the orthodontic treatment group had lower age, lower BMI, smaller waist circumference, reduced incidence of metabolic syndrome, and less difficulty when chewing and speaking. They also exhibited higher levels of both education and household income. TMD symptoms within the most recent 1 year were more frequent in the orthodontic treatment group, when no regression analysis was performed. Clicking and functional impairments significantly differed between the orthodontic treatment group and the group without orthodontic treatment. However, the presence of tenderness or pain around the ears and cheeks did not differ between the groups.
Table 2 shows adjusted ORs and their 95% CIs. For orthodontic treatment and TMD, adjusted ORs and their 95% CIs were 1.614 (1.189–2.190), 1.573 (1.162–2.129), and 1.612 (1.182–2.196) for Models 2, 3, and 4, respectively (p < 0.05). Adjusted ORs and their 95% CIs for orthodontic treatment and clicking were 1.778 (1.289–2.454), 1.742 (1.265–2.400), and 1.770 (1.280–2.449) for Models 2, 3, and 4, respectively (p < 0.05). Adjusted ORs and their 95% CIs in orthodontic treatment and tenderness or pain were 1.043 (0.661–1.644), 0.994 (0.632–1.563), and 0.978 (0.607–1.576) for Models 2, 3, and 4, respectively (p > 0.05). Adjusted ORs and their 95% CIs in orthodontic treatment and mouth opening limitation were 1.201 (0.797–1.810), 1.142 (0.754–1.730), and 1.118 (0.734–1.704) for Models 2, 3, and 4, respectively (p > 0.05). These results indicate that TMJ clicking was more frequent in the orthodontic treatment group; however, TMJ pain or dysfunction did not show any difference between the orthodontic treatment group and the group without orthodontic treatment.
DISCUSSION
This study evaluated the association between orthodontic treatment and TMD in a national sample of the South Korean population. The results indicate that orthodontic treatment was associated with TMJ clicking, but was not associated with tenderness or pain and functional impairment of the TMJ.
The American Association of Dental Research defines TMD as a group of musculoskeletal and neuromuscular conditions involving the TMJ, masticatory muscles, and other associated tissues.6 The most common symptoms of TMD are TMJ sounds, pain, and limited mouth opening. However, TMJ clicking is used to screen for TMJ intra-articular disorders.78 Disc displacement with reduction without limited opening has not been considered as a symptom requiring treatment.78 TMJ clicking is a clinically normal condition.89
In the present study, the orthodontic treatment group showed higher ORs and corresponding 95% CIs in TMD. Hwang and Park5 also reported similar results and concluded that a history of orthodontic treatment could be related to increased symptoms of TMD. However, care must be taken when interpreting these results. The present subgroup analysis showed that TMJ pain or dysfunction was not associated with orthodontic treatment. Moreover, the present subgroup analysis suggested that higher ORs in TMD seem to reflect a higher prevalence of TMJ clicking in the orthodontic treatment group. However, Hwang and Park5 did not perform any subgroup analysis. Therefore, it is inappropriate to conclude that orthodontic treatment is related to TMD without any subgroup analysis.
The orthodontic treatment group showed a higher prevalence of TMJ clicking in the present study. There are several possible explanations for this result. First, greater prevalence of TMJ clicking in the orthodontic treatment group may be associated with the participants' states of malocclusion before orthodontic treatment. TMD has been a topic of interest in dentistry, especially with regard to orthodontics and malocclusion. Various studies have been performed to determine relationships between TMJ and malocclusion. Some studies have shown that children with malocclusion, such as a deep bite and unilateral crossbite, tended to experience additional symptoms of TMD with increased age.310 Other clinical studies showed that the mean overbite of the group with TMJ clicking was greater than that of the group without clicking.11 Furthermore, subjects with Class II malocclusion showed increased rates of TMD among orthodontic treatment patients.12 Similarly, girls with normal occlusion showed reduced prevalence of TMJ clicking, compared to girls with Class II malocclusion who had or had not received orthodontic treatment.13 However, most orthodontists have indicated that orthodontic treatment does not increase or decrease TMD signs and symptoms, despite the association of malocclusion with TMD.1415 Some studies have reported that TMJ clicking was not reduced after treatment for TMD.1617 The results of the present study suggested that patients with malocclusion and malocclusion-related TMJ clicking might seek orthodontic treatment; however, their TMJ clicking was not affected by orthodontic treatment.
Second, the increased prevalence of TMJ clicking in the orthodontic treatment group may be associated with the age and sex of the patients. Most patients who visit orthodontic clinics are adolescents and young females. The percentage of male patients in the orthodontic treatment group was lower than in the group without orthodontic treatment in the present study. Some studies reported that TMJ clicking increased with age until adulthood.181920 A recent longitudinal study reported that TMJ clicking increased by 3.3-fold in individuals under 40 years of age.21 In the present study, the mean age of participants in the orthodontic treatment group was 31 years, while that of the non-orthodontic treatment group was 47 years. Accordingly, the age group more affected by TMJ clicking might seek orthodontic treatment; this phenomenon might be reflected in this result.
Third, occlusal interference during orthodontic treatment may be related to the increased prevalence of TMJ clicking in the orthodontic treatment group, although the effects of occlusal interference on TMJ and masticator systems are controversial. Occlusal interference is inevitable during orthodontic treatment. TMJ clicking has been reported as a result of occlusal interference, especially due to lateral deviation between retruded and intercuspal positions.2223 However, some patients who exhibited TMD signs and symptoms that resulted from occlusal interference were returned to normal after removal of the interference.24 Notably, subjects without TMD adapted to the interference.25 Some studies have reported that occlusal interference affects the activities of both the masticatory muscle and the TMJ.2627 Occlusal interference increases muscle pain in TMD patients.2627 However, subjects without a history of TMD showed fewer symptoms and better adaptation to occlusal interference. These results are similar to our findings; the present study showed that TMJ pain or dysfunction did not differ between the two groups.
We fully understand that these results should be cautiously interpreted because this study has some limitations. First, the data used in this study were only obtained from one Asian country, South Korea. Therefore, it is difficult to create a generalization about the results of the present study. However, South Korea has a very homogenous ethnic population and the results of this study are more consistent than other population-based studies. Second, it was impossible to show a cause-andeffect relationship between orthodontic treatment and TMD because the present study was a cross-sectional study, rather than a longitudinal study. Third, TMD was not diagnosed by the use of radiographs, such as magnetic resonance imaging, because national survey data were used in the present study. However, clinical diagnostic criteria for pain-related TMD and one intraarticular TMD have shown adequate validity (sensitivity ≥ 0.80, specificity ≥ 0.97), although radiographs were used as the reference standard.28 Fourth, it is impossible to investigate the previous TMD status of the patients who sought orthodontic treatment because these data were not surveyed. Fifth, the data in the present study did not provide any information regarding the nature of the original malocclusion and types of orthodontic treatment because this survey did not include any interviews or examinations to assess these characteristics. Future well-controlled longitudinal studies are needed to clarify the relationships between type of orthodontic treatment or malocclusion and TMD. Sixth, there was no consideration of the possibility of bias due to differences in sample sizes between the two groups. The number participants in the orthodontic treatment group was approximately 4% of that in the control group (i.e., the group that did not receive orthodontic treatment). Because of this difference in size, the incidence of TMJ clicking may be relatively high.
Despite these limitations, the present study provides sufficient epidemiological information regarding orthodontic treatment and TMD. The present study used data from a nationally representative sample and analyzed it in the context of multiple covariates. Most studies have investigated age- or gender-specific samples and did not include adjustments for confounding factors associated with TMD.132930 This study showed that TMJ pain or dysfunction was not associated with orthodontic treatment after adjustment for age, sex, and other confounding factors. However, there remains a need to record TMD symptoms and signs, especially TMJ clicking before and during orthodontic treatment, for medico-legal purposes.

 XML Download
XML Download